
Remember me



From 1 February 2022 to 31 August 2022, 396 questionnaires were collected from patients under treatment in 76 hospitals across Italy; 45 were excluded from the analysis because patients jointly declared the following: they were not receiving specific therapy for bone metastases and there were no bone metastases.
The analysis was performed on 351 (88.6%) questionnaires and showed that the majority of responding patients with cancer were being treated at eight cancer centers (IRCCS Istituto Tumori of Milan, ASST Papa Giovanni XXIII of Bergamo, IRCSS Sacro Cuore Don Calabria of Negrar, Molinette Hospital of Turin, Azienda Ospedaliera Santa Maria of Terni, Casa di Cura INI of Grottaferrata, IRCCS Policlinico A. Gemelli of Rome, and V. Fazi Hospital of Lecce).
The majority of responding patients were being treated at centers in Northern Italy (69%), followed by Central Italy (24%) and the South/Islands (7%).
Age of patients and distribution by cancer disease are summarized in Fig. 1.
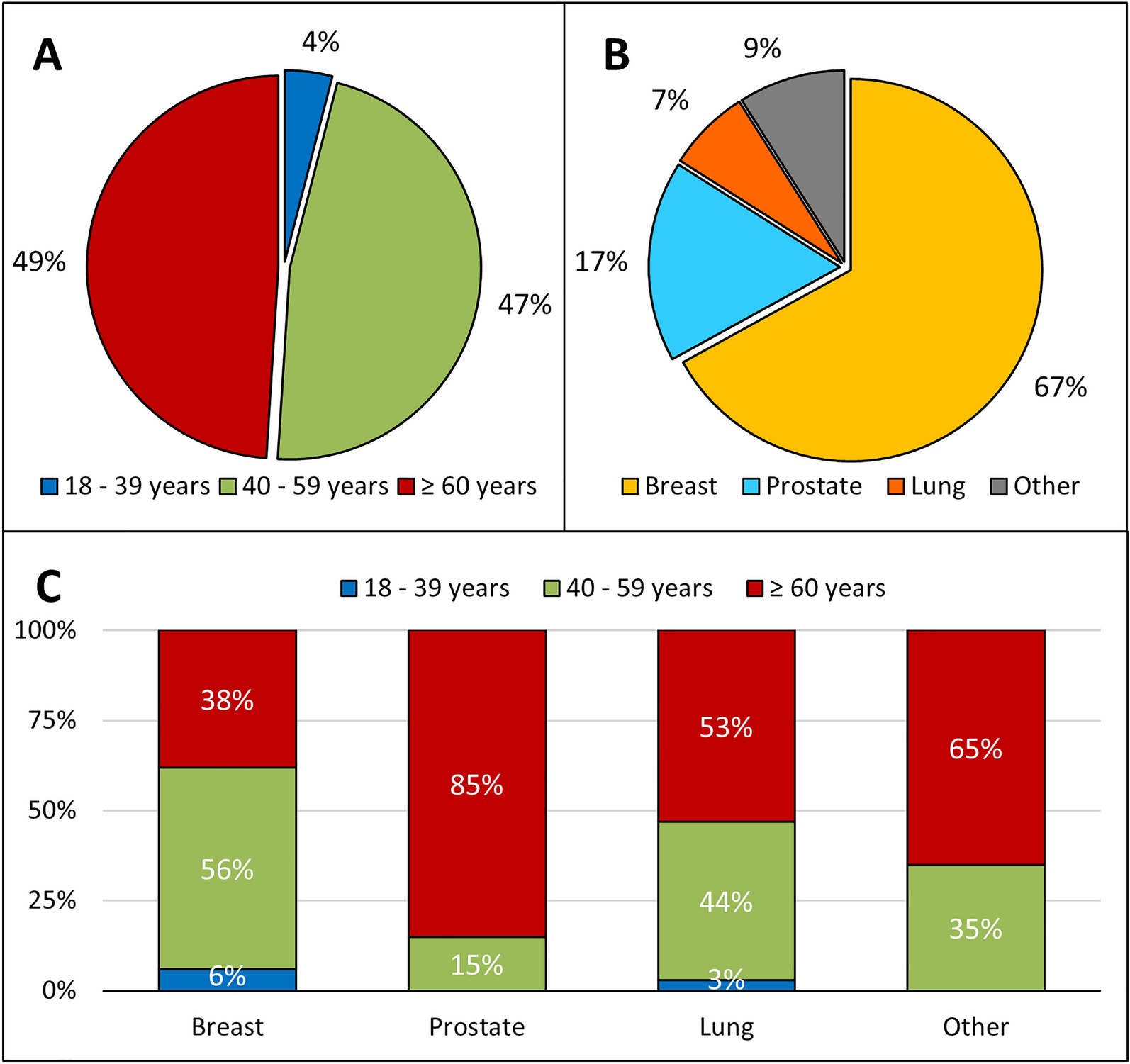
Fig. 1
Patient’s characteristics. Distribution of 351 patients by age (A), by primary cancer site (B), and by the combination of age and primary cancer site (C)
About 50% of patients were ≥ 60 years of age, 47% were 40–59 years old, and only 4% were 18–39 years old. The primary cancer site was the breast (67%) followed by prostate (17%) and lung (7%). Overall, 63% of patients with breast cancer were over 40 years old of age.
About the degree of information that patients claimed to have received about bone metastases and related information sources (questions 5 and 7), the results showed that 75% (263/351) of patients stated that they were “fairly enough/a lot” informed about bone metastases and 82% (288/351) that they “fairly/well” understood the information they received.
Regarding information sources, the patients reported that information on bone metastases was mainly obtained from the oncologist (92%), followed by the general practitioner (32%), the internet (19%), family and friends (7%), magazines (4%), and social groups (1%), with difference between the various age groups (Table 1). The oncologist was the most frequent source of information for the age group ≥ 60 years (95%); the internet was used more frequently by the age group 18–39 years (67%).
Table 1 Sources of information about bone metastases in all patients and by ageA chi-square test of independence revealed that the choice of information sources about bone metastases varied significantly by age group (p = 0.0044). Younger patients tended to rely more on digital resources (e.g., internet) or peer networks, whereas older patients were more likely to seek information from oncologists and general practitioners.
Out of 351 patients with bone metastases, 72% stated that they received information about skeletal complications (question 8) and that the oncologist was the most frequent source of information (85%), followed by the internet (32%), general practitioner (17%), social groups (9%), family and friends (7%), and magazines (2%). The internet, on the other hand, was the information source predominantly used by young people (18–39 years) in comparison to older patients (≥ 60 years): 47% versus 20%, respectively (Table 2).
Table 2 Sources of information about skeletal complications in all patients and by ageA chi-square test of independence indicated a statistically significant difference among age groups for the information sources about skeletal complications (p = 0.0356). Younger individuals were more likely to rely on digital platforms and peer networks, whereas older adults primarily consulted healthcare professionals.
About the patient’s involvement in the care pathway (questions 10 and 11), the results showed that 89% (312/351) of patients said they would like to be involved in the care pathway and that 85% (299/351) said they would ask the doctor questions to better understand their disease and treatment management.
Regarding the degree of patient attention to the issue of bone metastases (question 12), 83% (284/342) of the patients answered that they were “quite a lot/much” attentive on a scale of 1 to 4 (1 = not at all; 2 = a little; 3 = quite a lot; 4 = much), with a mean response of 3.2 (IQR 3–4). The breast patients with cancer (mean 3.3) and the patients aged 40–59 years (mean 3.4) were the most attentive, on average, to bone metastases. In addition, 72% of patients answered that they were “fairly concerned/very worried/feeling anxious” on a scale of 1 to 5 (1 = quiet; 2 = slightly concerned; 3 = fairly concerned; 4 = very worried; 5 = feeling anxious), with a mean response of 3.1 (IQR 2–4). The breast patients with cancer (mean 3.4) and the younger (18–39 years) patients (mean 3.8) reported feeling more anxious.
About the type of therapy for bone metastases and its duration (questions 14–17), 82% (285/345) of patients responded that they were receiving specific therapy: 47% (134/285) zoledronic acid, 49% (140/285) denosumab, and 4% (11/285) other bisphosphonates. Drugs used for bone metastases in relation to age and tumor type are reported in Table 3.
Table 3 Distribution of patients by drugs used for bone metastases in relation to age and tumor typeMore than 80% of patients (240/279; 86%) stated that they had started drug therapy for bone metastases within 2 years. Only a third of patients (107/300; 36%) knew the duration of therapy and 86% (92/107) of these patients stated that they would have to continue therapy for bone metastases for a maximum of 2 years.
Regarding dental checkups (before starting therapy for bone metastases and during therapy and vitamin D and calcium supplementation; questions 18–23), 93% of patients (293/316) had an X-ray orthopanoramic and a dental examination before starting therapy and 78% (262/334) had received information regarding periodic dental checkups during therapy for bone metastases. About periodic dental checkups during drug therapy for bone metastases, 72% (225/311) of patients stated that they had a periodic dental checkup; this percentage was higher in patients younger (92%), with breast cancer (77%) and in therapy with denosumab (85%) (Table 4). Sixty-nine percent (152/221) of the patients responded that they undergo periodic dental checkups every 3–6 months (question 22). Dental complications were reported by only 0.3% of patients who had undergone basal dental evaluations before starting therapy for bone metastases.
Table 4 Distribution of patients by periodic dental checkups in relation to age, tumor type, and drugs administered for bone metastasesDuring specific therapies for bone metastases, 83% of patients (267/320) reported taking oral supplementation with vitamin D and calcium during therapy for bone metastases (question 23).
Table 5 shows the percentage of patients who reported taking/not taking vitamin and calcium supplementation according to age, cancer, and type of drug administered for bone metastases.
Table 5 Distribution of patients by vitamin D and calcium supplementation in relation to age, tumor type, and drugs administered for bone metastasesWhen the various age groups were evaluated, vitamin D and calcium supplementation was taken by 92% of younger patients (18–39 years), 86% of patients aged 40–59 patients, and 80% of over-60 patients.
On the basis of the primary tumor, oral supplementation was taken more by patients with breast cancer (89%) followed by patients with lung cancer (71%) and patients with prostate cancer (67%). According to the type of therapy for bone metastases, vitamin D and calcium supplementation was prevalent in patients treated with denosumab (96%) in comparison to zoledronic acid (73%) (Table 5).
To investigate the association between information provision and adherence to dental checkups, between information sources and adherence to dental checkups, and between information sources and vitamin D intake to assess whether awareness plays a role in supplementation decisions, cross-tabulation analyses were performed.
The results showed that there was a strong association between receiving information on dental checkups during specific therapy for bone metastases (question 20) and actually undergoing those checkups (question 21) (p < 0.001). In contrast, the relationship between patients’ adherence to dental checkups (question 21) and the sources of information about bone metastases (multiple-answer question 6) was not statistically significant (p = 0.074).
In addition, information sources (again derived from multiple-answer question 6) were not significantly associated with vitamin D intake (question 23) (p = 0.155).
Other correlation analyses were performed to investigate the relationships between four clinical and demographic factors (age group, tumor type, region, and macro region) and four key variables (bone metastases, dental controls, vitamin D intake, and information source). The results showed that age group was linked to both dental controls (p = 0.006) and information source (p = 0.004), suggesting that the adherence to dental checkups and the source of information about bone metastasis are directly linked to different age cohorts. Tumor type was also significantly related to dental controls (p = 0.001) and vitamin D intake (p < 0.0001), indicating that the specific tumor profiles might influence a patient’s preventive behaviors and supplement use.
Geographic factors also play an important role. Region shows significant associations with all four variables: bone metastases (p < 0.0001), dental controls (p < 0.0001), vitamin D intake (p < 0.0001), and information source (p = 0.011). This points to substantial regional variations in clinical and behavioral outcomes. Likewise, macro region (North, Centre, South/Islands) correlates significantly with dental controls (p = 0.001), vitamin D intake (p = 0.031), and information source (p = 0.001), suggesting that broader geographic divisions may further shape patient behaviors and information-seeking patterns.
The seventh part of the questionnaire was related to skeletal complications (questions 24 and 25): 47% (159/336) of patients responded that they had skeletal complications. Radiotherapy to bone metastases was the most frequent skeletal-related event (149/159; 94%). Other reported skeletal complications were pathological fractures (37/159; 23%), bone surgery (17/159; 11%), spinal cord compression (10/159; 6%), and hypercalcaemia (3/159; 2%). About half of the patients (167/330; 51%) reported pain at the sites of bone metastases, 90% (208/231) of the respondents said they had reported this symptom to their doctor (questions 26 and 27), and 71% (184/261) of patients stated that they had experienced “quite/much benefit” from specific therapy for bone metastases on the pain symptom (question 28).
The last part of the questionnaire assessed the impact of the COVID-19 pandemic on the treatment pathway for bone metastases (questions 29 and 30), because in the years 2020–2021 many patients reported having difficulty starting or continuing hospital treatment. Out of 344 patients, 75% stated that it had no impact on their treatment pathway and 25% stated that it had an impact; the main problem encountered (49/87; 56%) was a delay in making one or more oncology visits, without compromising the course of the therapy.
Evaluating the impact of the COVID-19 pandemic on the treatment pathway of bone metastases according to the geographical area of the patients’ cancer center of reference, the data showed a lower impact on the course of treatment reported by patients treated at oncological centers in Northern Italy (20%) compared to the other geographical areas (36% in the Centre and 41% in South/Island of Italy).
For complete questionnaire answers, see online supplementary material.
Comments (0)