
Remember me



No publicly available CMs for B cell ALL were identified; the results of the targeted literature review were used to create an initial CM (data not shown). This was for a broad population of adults with leukemia, as not enough published evidence existed specifically for adults with B cell ALL. Thus, interviews in this patient population were conducted. The initial CM informed the content and initial analysis of CE interviews and then the results of the interviews informed development of an updated, B cell ALL-specific CM.
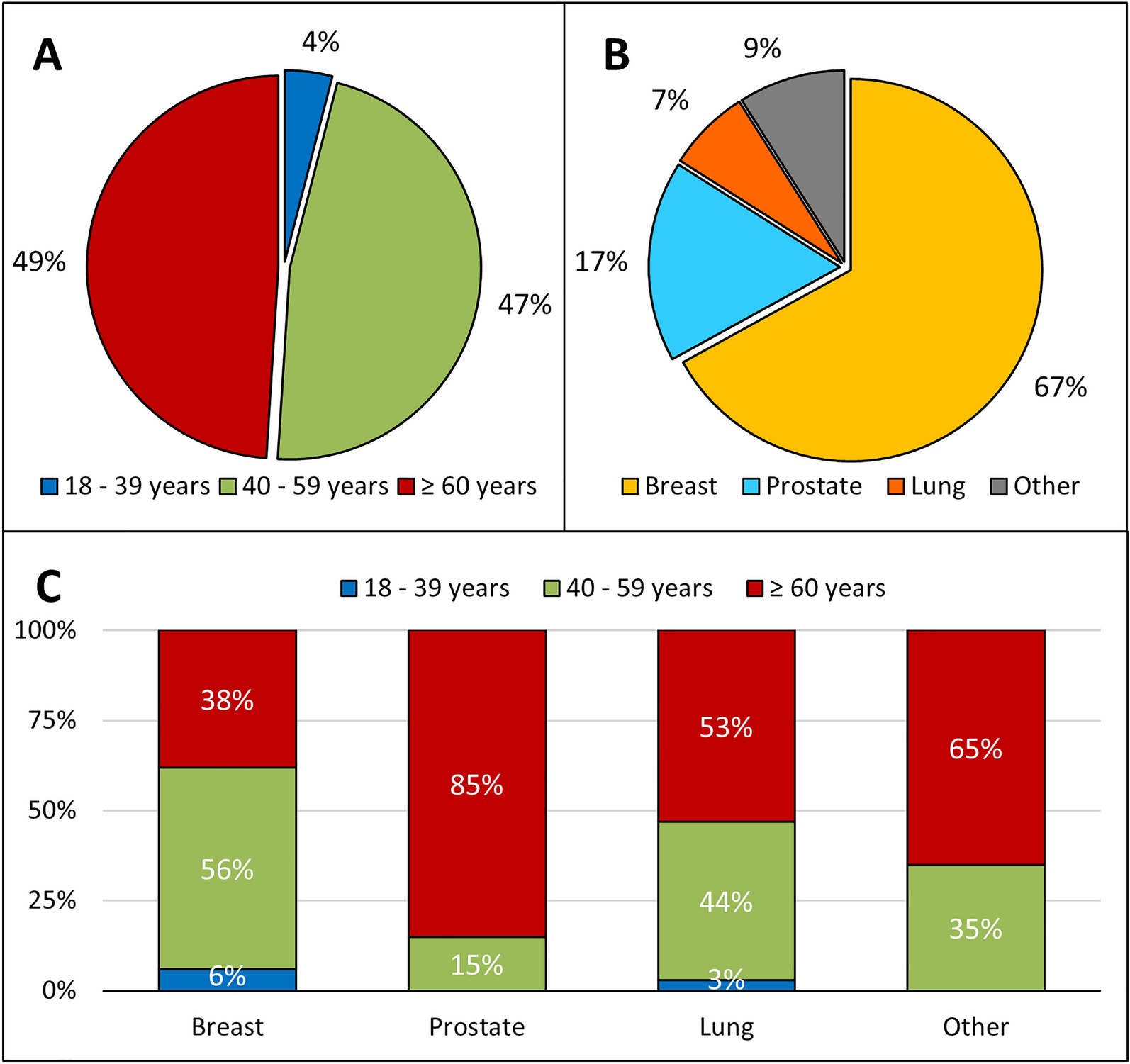
Study ParticipantsCE interviews were conducted with 20 participants who met the eligibility criteria (11 recruited through the patient advocacy group, 9 through third-party vendors), all of whom were USA-based. The mean age was 57.9 years, 11 (55%) were female, and 16 (80%) were white (Table 1). At the time of screening, 16 participants (80%) had been diagnosed within the last 18 months and interviews were completed within this timeframe for all but one of these participants. Approximately one-third (35%) had Ph+ B cell ALL and one-third (30%) had Ph− B cell ALL; the remaining third were of an unknown Ph status. A detailed account of medications and treatments was not collected. However, in interviews, most participants (n = 16, 80%) indicated that they had received chemotherapy-based treatment for B cell ALL and three (15%) of these indicated they had also undergone a transplant. Three participants (15%) had not started any treatment and one (5%) reported being in a clinical trial (recruited before clinical trial participation being added as an exclusion criterion).
Table 1 Patient demographics and clinical characteristicsSigns and SymptomsParticipants described a broad range of symptoms since onset up until the current time of the interview, including during treatment; 63 different signs and symptoms were reported overall (Supplementary Table S1).
Fatigue and fatigue-related symptoms were most frequent, with all reporting a symptom within this domain (n = 20, 100%). Participants often reported that this was the first indicator that something was not right with their health, but it was also exacerbated by treatment, especially chemotherapy. They described it using a variety of terms including tiredness (n = 17, 85%), fatigue (n = 15, 75%), weakness (n = 11, 55%), exhaustion (n = 8, 40%), and drowsiness (n = 2, 10%).
Gastrointestinal signs and symptoms were also reported by the majority of participants (n = 18, 90%) and included lack of appetite (n = 14, 70%), nausea (n = 12, 60%), and diarrhea (n = 8, 40%). Some participants noted that lack of appetite or nausea occurred before treatment, and some noted this was a side effect of treatment that improved post treatment.
Central and peripheral nervous system symptoms were the next most frequent category (n = 16, 80%) and these included tingling in hands and feet (n = 9, 45%), which was noted during treatment, and headache (n = 8, 40), which was both before and during treatment.
Pain-related symptoms were frequently reported (n = 14, 70%) and were noted as one of the first symptoms before diagnosis. Several types of pain were described, including general (n = 9, 45%), joint (n = 6, 30%), bone, extremity, and muscle (all n = 5, 25%), and even within each type, were described in a multitude of ways, including dull, sharp, or radiating.
The domains of respiratory-, blood-, and mouth-related symptoms were also frequently reported (all n = 14, 70%) with individual symptoms within those domains of shortness of breath (n = 13, 65%), bruising (n = 11, 55%), and mouth sores (n = 8, 40%) being the most frequent, respectively. Shortness of breath and bruising were most often described as part of the initial experience with B cell ALL, whereas mouth sores were reported more for the treatment period. Among individual physical symptoms not assigned to a specific domain, sweating was reported by 12 (60%) participants, and almost exclusively noted around the time of diagnosis.
Around diagnosis, the most disturbing or bothersome symptoms, with ratings provided by more than one participant, included enlarged lymph nodes (average disturbance rating of 9.3), general pain (7.9), congestion (7.5), bone pain (7.2), and sweating (7.0) (Supplementary Table S1). Average disturbance ratings for most signs/symptoms were generally low at the time of interview (all 6.0 or below for any rated by more than one participant) but had worsened between diagnosis and the interview (which included the treatment period for many participants).
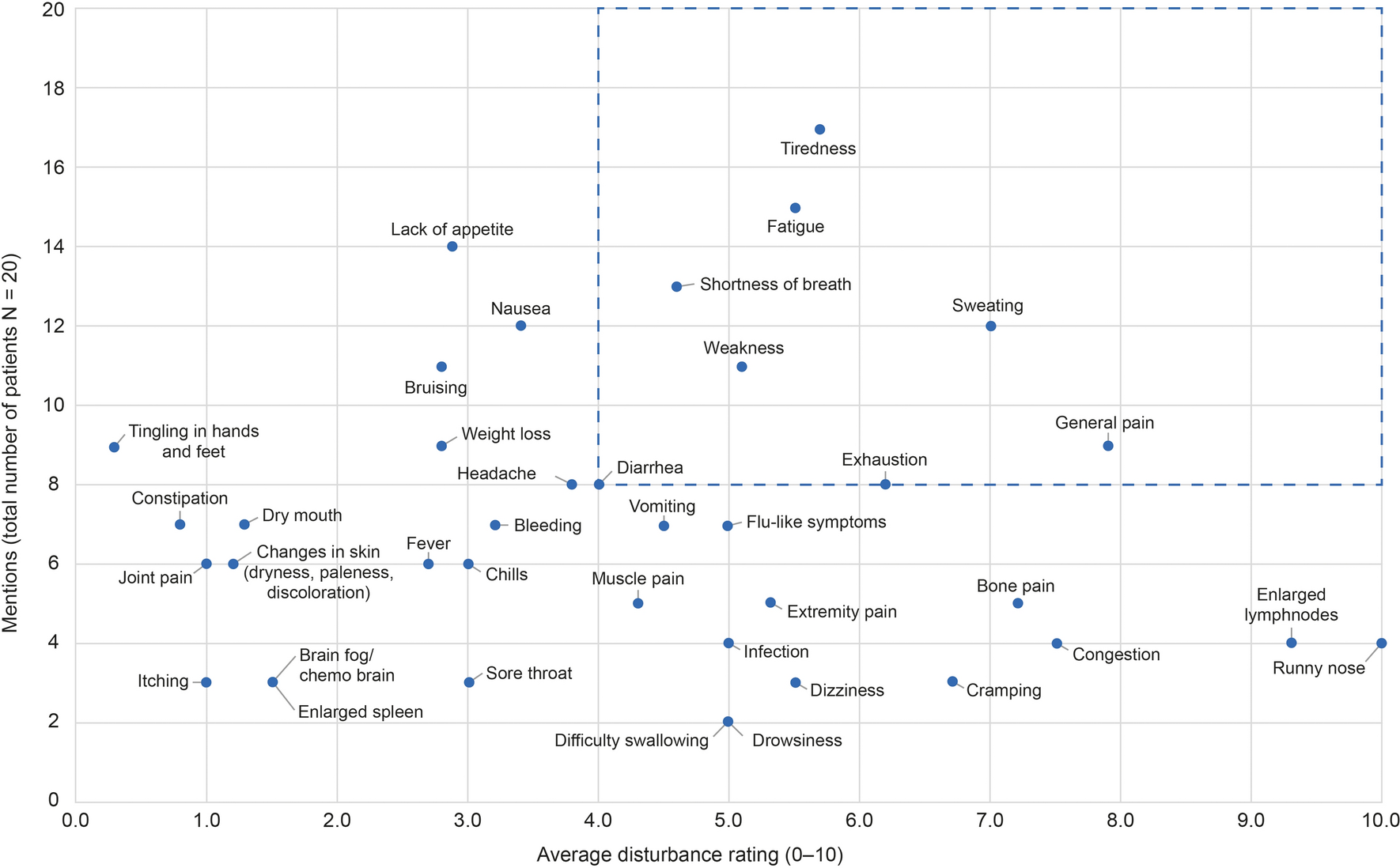
Salient signs or symptoms were defined based on the frequency of occurrence as well as disturbance ratings. Of the 63 identified signs/symptoms overall, 16 were deemed salient for at least one timepoint (Figs. 1, 2, 3; Supplementary Table S2). See Table 2 for example quotes from patients relating to salient signs and symptoms. Following a similar pattern to disturbance ratings, the number of salient signs and symptoms increased after diagnosis, peaking “at worst,” and then decreased again by the time of interview. Eight were salient at diagnosis (fatigue and fatigue-related symptoms [tiredness, weakness, and exhaustion], shortness of breath, sweating, general pain, and diarrhea; Fig. 1) but only four remained salient by the time of interview (all fatigue-related: tiredness, fatigue, weakness, and exhaustion; Fig. 3).
Fig. 1
Mapping signs/symptoms reported by participants versus average disturbance rating around diagnosis. The dashed box denotes salient signs/symptoms, defined as those that were reported by ≥ 40% of participants with an average disturbance rating of ≥ 4/10. Only concepts mentioned by ≥ 2 participants, which have a disturbance rating from ≥ 1 participant, are included. For a full list of signs/symptoms see Supplementary Table S1
Fig. 2
Mapping signs/symptoms reported by participants versus average disturbance rating at worst. The dashed box denotes salient signs/symptoms, defined as those that were reported by ≥ 40% of participants with an average disturbance rating of ≥ 4/10. Only concepts mentioned by ≥ 2 participants, which have a disturbance rating from ≥ 1 participant, are included. For a full list of signs/symptoms see Supplementary Table S1
Fig. 3
Mapping signs/symptoms reported by participants versus average disturbance rating at time of interview. The dashed box denotes salient signs/symptoms, defined as those that were reported by ≥ 40% of participants with an average disturbance rating of ≥ 4/10. Only concepts mentioned by ≥ 2 participants, which have a disturbance rating from ≥ 1 participant, are included. For a full list of signs/symptoms see Supplementary Table S1
Table 2 Example patient quotes on salient signs or symptoms of B cell ALLOwing to the acute onset of B cell ALL, participants had often already begun or completed treatment at the time of interview and thus most participants discussed signs and symptoms experienced during treatment as well as those experienced around diagnosis. While it was not always possible to clarify if these were experienced before or after treatment, some primarily treatment-period signs and symptoms were identified. These included some gastrointestinal items, such as acid reflux/indigestion, feeling bloated, and hemorrhoids, although these were only mentioned by one or two participants each (5–10%). Similarly, some central and peripheral nervous system symptoms such as neuropathy-related numbness or paralysis, brain fog, sensitivity to light or smells, and blurry or starry/double vision were only mentioned in relation to the treatment period (n = 1–3 for each, 5–15%). Other symptoms noted only during the treatment period included change in taste of food (n = 4, 20%), hair loss (n = 10, 50%), and swelling in arms and legs (n = 5, 25%). Otherwise, most signs and symptoms were reported during both diagnosis and treatment periods, but the experience of them could change for individual participants. For example, fatigue-related symptoms sometimes worsened during treatment. Some participants reported that general, radiating, or bone pain improved once treatment started, although for some, pain started after treatment initiation. Similarly, respiratory-related symptoms improved after treatment initiation for some but worsened for others.
ImpactsParticipants described a broad range of ways that B cell ALL and its treatment had impacted their lives; 37 impacts were reported overall. All participants reported emotional impacts, and most reported impacts on physical and social well-being (both n = 16, 80%; Table 3 and Supplementary Table S3). The most commonly reported emotional impact was worry, fear, and nervousness (n = 12, 60%), generally regarding diagnosis and the future; similarly, shock/surprise and sadness/depression (both n = 8, 40%) were commonly experienced. For emotional impacts, average disturbance ratings were 6.5–8.0 around diagnosis, and 8.0–10.0 at worst, although it should be noted that few ratings were collected for all impacts, owing to time constraints. In terms of physical impacts, participants often described how their fatigue or tiredness made them unable to do previous activities or hobbies, which was the most commonly reported single impact (n = 15, 75%); decreased ability for activities of daily living was also common (n = 12, 60%). Sleep was commonly impacted (n = 11, 55%) and this was often attributed to pain or sweating, or mental or emotional concerns. Average disturbance ratings for physical impacts were 1.0–7.0 around diagnosis and 7.5–10.0 at worst. The most common social impact was staying at home/not socializing, reported by nine (45%) participants; reasons included tiredness and risk for infection. Available average disturbance ratings for social impacts were 4.7 around diagnosis and 8.4 at worst. Under the role at work domain, decreased ability to work was also reported for 11 (55%) participants. See Table 4 for example quotes from patients relating to key impacts.
Table 3 Frequency of impact mentions and average disturbance ratingsTable 4 Example patient quotes on key impacts of B cell ALLConcept SaturationOf the 63 signs and symptoms identified across four waves of interviews, 50 (79%) were identified in the first wave, 57 (91%) by the second, and 60 (95%) by the third. Of the 37 impacts identified in total, 27 (73%) were identified in the first wave and 95% were captured in the first three waves. Five new concepts (three signs or symptoms, two impacts) were identified in the final wave of interviews, only one of which was noted by more than one person (cramping: n = 3, 15%).
Final CMBased on the results of the CE interviews, considering number of mentions, disturbance ratings, and timing of when signs/symptoms were reported in relation to treatment, a patient-centered CM for older patients and those with substantial comorbidities with B cell ALL was created (Fig. 4).
Fig. 4
Final CM of patients’ experience with B cell ALL. Signs and symptoms in bold are those that were most salient based on overall number of mentions (≥ 40% of participants) and average disturbance ratings (≥ 4/10). Impacts in bold are those that were reported by ≥ 40% of participants. ALL acute lymphoblastic leukemia, CM conceptual model, Ph+ Philadelphia chromosome positive, Ph− Philadelphia chromosome negative
Comments (0)