
Remember me


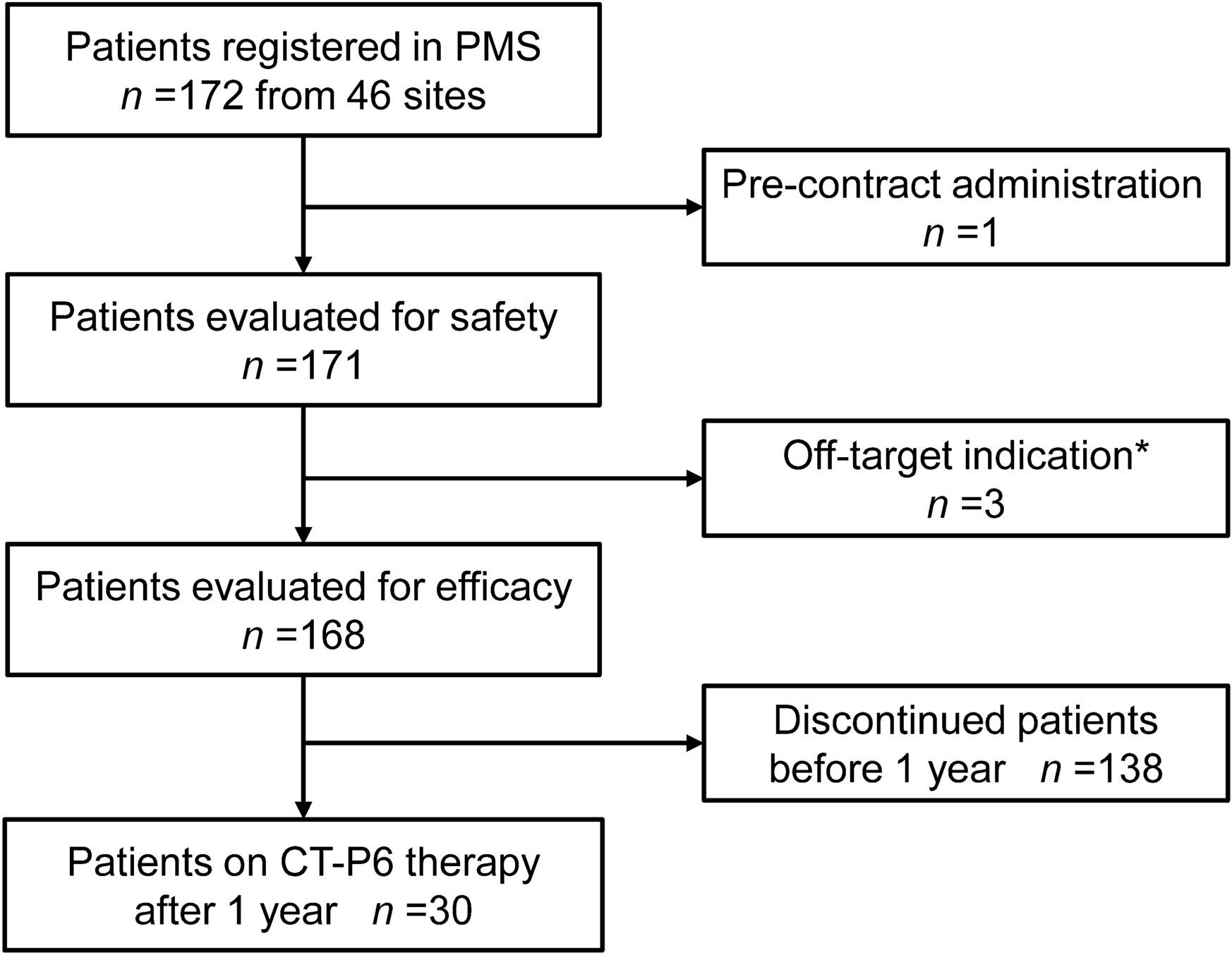

In this prospective cohort study, a total of 172 patients were registered from 46 clinical sites in this PMS, and 171 patients who received at least one dose after August 2018 were included in the safety analysis (Fig. 1). The baseline patient characteristics of 171 patients in the safety analysis are presented in Table 1. The mean age was 69.1 years, and 95.9% of patients had ECOG performance status of 0–1. High HER2 expression was confirmed in 69.6% of patients as IHC3+ and in 28.7% as IHC2+ with ISH positive. Three patients were excluded from the efficacy analysis population owing to a lack of ISH testing with IHC2+. Prior to the administration of CT-P6, the originator trastuzumab was administered to 20 patients. Among them, 11 patients (6.4%) were directly switched to CT-P6, and 9 patients (5.3%) received CT-P6 after a period following the discontinuation of the originator trastuzumab.
Fig. 1
Patient diagram. *Patients with only HER2 protein expression (2+) and no gene amplification test results
Table 1 Patient baseline characteristics, tumor status, prior medication, and treatment pattern of CT-P6 therapyPatients were treated with CT-P6 chemotherapy in various treatment settings as follows: (A) 100 patients (58.5%) at first-line therapy for inoperable advanced tumors without prior treatment, (B) 13 patients (7.6%) at first-line postoperative therapy starting within 3 months after noncurative resection, (C) 17 patients (9.9%) at first-line therapy for recurrence more than 6 months after curative resection, (D) 24 patients (14.0%) at second-line therapy for recurrence after postoperative adjuvant therapy, and (E) 17 patients (9.9%) at second- or later-line therapy for recurrence after chemotherapy with or without gastrectomy.
Chemotherapeutic agents combined with CT-P6 comprised mainly fluoropyrimidines and platinum agents. The most frequent regimen was a combination of S-1 and oxaliplatin, used in 77 patients (45.0%). Paclitaxel or irinotecan was administered to only seven patients, six of whom received these drugs as second-line or later therapy for recurrence after fluoropyrimidine and/or platinum treatment. Initial and cumulative doses of CT-P6 and combined agents are presented in Supplementary Table S2.
SafetyThe incidence of treatment-related adverse events was 88.3%, including 32.2% with grade ≥ 3 adverse events (Table 2). Among them, CT-P6-related adverse events of all grades and grade ≥ 3 were reported in 67.3% and 15.8%, respectively. Those incidences were slightly higher in the 151 trastuzumab-naïve patients, at 70.9% and 17.2%, respectively, whereas in the 20 excluded patients with prior originator trastuzumab treatment, adverse events were less frequent at 40.0%, with grade ≥ 3 events reported in 1 patient (5%). The common adverse events with incidence > 20% were anemia, neutropenia, thrombocytopenia, diarrhea, nausea, anorexia, and peripheral neuropathy. About 10% of these adverse events were not related to CT-P6 and were attributable to the combined chemotherapeutic agents. In contrast, all IRs, cardiac disorders, and ILD were related to CT-P6. The incidence of the reported adverse events related to CT-P6 chemotherapy is listed by System Organ Class in Supplementary Table S3.
Table 2 Incidence of treatment-related and CT-P6-related adverse events in 171 patients in the safety analysis populationInfusion ReactionsIRs were the most frequent and specific adverse events to CT-P6, occurring in 21 patients out of 171 patients (12.3%) per 1416 infusions (1.5%). Twenty out of the 21 IRs occurred on the first administration of CT-P6. All IRs were nonserious and resolved within a day. There were no treatment discontinuations due to IRs, and no recurrent IRs were reported with subsequent CT-P6 infusions. Regarding the infusion time, 95.9% of the first administrations were infused for 90 min or more, and the 20 IRs occurred with this standard infusion time. After the second dose, 84.4% of patients received infusions for less than 90 min, but no IRs were reported with this rapid infusion. No IRs occurred in the 11 patients switched from originator trastuzumab, including 4 patients who received the first CT-P6 infusion in less than 60 min.
Univariate analysis using the Cox regression model showed significant associations of IRs with a history of drug allergy, higher baseline CRP levels (≥ 0.5 mg/dL), and prior gastrectomy. Subsequent multivariable analysis identified CRP as the only significant independent risk factor (HR 5.08, 95% CI 1.65–15.6, p = 0.005) (Table 3).
Table 3 Cox regression analysis of baseline patient factors on infusion reactions to CT-P6Cardiac DysfunctionCardiac adverse events were reported in four cases (2.3%), including two cases of grade 1 cardiac dysfunction leading to heart failure. A 63-year-old male showed grade 1 abnormalities in echocardiogram (global longitudinal strain = 12%, cardiac index = 1.7 L/min/m2) on the sixth infusion of CT-P6. Treatment was paused for 105 days and then resumed for seven courses after recovery. Another patient was an 84-year-old male. Left ventricular ejection fraction decreased from baseline > 50% to 48.2% on the fourth infusion with ventricular premature contractions (grade 1). He recovered without interrupting treatment and continued 19 courses of CT-P6 therapy. Two cases of severe ischemic heart disease were reported. A 73-year-old female died of a myocardial infarction 14 days after switching back to the originator trastuzumab following two courses of CT-P6 in combination with cisplatin and S-1. She had dehydration from chronic diarrhea, and the causality with the medications remained uncertain. This was the only adverse event leading to death in this PMS. A 75-year-old male experienced chest pain and ST elevation on ECG the day after the first course of CT-P6 therapy (grade 4). He discontinued CT-P6 therapy and transitioned to palliative care. The causality was unclear, with multiple risk factors of hypertension, dyslipidemia, cerebral infarction, exertional dyspnea, and anemia (see details in Supplementary Table S4).
Interstitial Lung DiseaseILD occurred in four patients, an incidence of 2.3%. All four patients discontinued treatment and received corticosteroid therapy. Recovery was confirmed in two severe patients (grade 2 and grade 3), but the outcomes of two grade 1 patients were not available owing to treatment discontinuation (tumor progression and subsequent conversion surgery). All four patients were male, with a mean age of 68.3 years, and had abnormalities on pretreatment imaging (emphysema, ground-glass opacities, and lung metastases). Additionally, three patients had respiratory complications, including pharyngitis, interstitial pneumonia, and chronic obstructive pulmonary disease (COPD). Platinum agents and fluoropyrimidines were administered prior to or concurrently with CT-P6 in all four patients, and two patients received paclitaxel and/or irinotecan (Supplementary Table S5).
EfficacyTumor ResponseTumor response was assessed in 125 patients with measurable lesion by the treating physicians. Three patients (2.4%) achieved CR, resulting in an ORR of 34.4%. The DCR, including SD, reached 82.4% in patients with advanced HER2-positive gastric cancer treated with CT-P6 chemotherapy (Fig. 2a). When excluding the 12 patients who had received prior trastuzumab treatment, the ORR and DCR were 33.6% and 82.3%, respectively, showing similar results.
Fig. 2
Effect of CT-P6 therapy for HER2-positive advanced gastric cancer. a Best overall response and b Kaplan–Meier curve for progression-free survival. CI, confidence interval; CR, complete response; NE, not evaluable; PD, progressive disease; PR, partial response; SD, stable disease
Treatment ContinuationThe median PFS for CT-P6 treatment was 7.4 months (95% CI 5.4–9.4 months), as determined by Kaplan–Meier analysis (Fig. 2b). Out of 168 patients, 30 patients (17.9%) continued CT-P6 therapy for the entire 1-year observation period. In addition, seven patients (4.2%) completed the planned treatment, and eight patients (4.8%) underwent conversion surgery after a good tumor response with CT-P6 therapy. The success rate of conversion to surgery was 8.2% among the 98 patients with primary inoperable tumors who had not undergone surgery or prior chemotherapy. The chemotherapy regimen leading to conversion surgery was a combination of fluoropyrimidine and platinum agent with CT-P6, with an average of 6.1 treatment courses (range 3–16 courses). The patient characteristics and treatment effects are summarized in Supplementary Table S6.
Treatment had to be discontinued in 123 patients (73.2%) within 1 year. Disease progression was the most common reason, in 89 patients (53.0%), and adverse events led to treatment discontinuation in 16 patients (9.5%) (Table 4).
Table 4 Treatment persistence of CT-P6 and survival rates after a 1-year observation periodRisk Factors for Progression-Free SurvivalCox regression analyses were conducted to identify risk factors for PFS in 156 patients treated with CT-P6 in combination of fluoropyrimidine with or without platinum agent. Twelve patients who received other type of chemotherapy were excluded from the analysis. On univariate Cox regression analysis, basic factors such as sex (female versus male), age ≥ 65 years, and HER2 expression (IHC3+ versus 2 +) did not show significant association with PFS (HR 0.89, 1.11, and 0.88, respectively) (Supplementary Table S7) and were therefore not included in the subsequent multivariable analysis. The significant risk factors for PFS on multivariable analysis were primary site at the gastroesophageal junction versus stomach (HR 2.03, 95% CI 1.08–3.83, p = 0.029), number of metastases ≥ 3 (HR 2.00, 95% CI 1.14–3.52, p = 0.016), no gastrectomy (HR 0.37, 95% CI 0.19–0.69, p = 0.002), prior chemotherapy (HR 4.51, 95% CI 2.26–8.98, p < 0.001), and no concurrent use of platinum agent (HR 0.37, 95% CI 0.20–0.68, p = 0.001). PS (1–3 versus 0) and liver metastasis showed a tendency to be associated with shorter PFS, with HRs of 1.43 (p = 0.125) and 1.55 (p = 0.058), respectively (Fig. 3).
Fig. 3
Multivariable Cox regression analysis of baseline factors on progression-free survival. *p < 0.05, **p < 0.01, ***p < 0.001, CI, confidence interval; HR, hazard ratio
Patient Subgroup AnalysisFurther analyses were conducted on outcomes in patient subgroups classified by the status of gastrectomy and prior chemotherapy (i.e., treatment setting) and by concomitant chemotherapy (i.e., regimen), which were significant factors for PFS on previous multivariable analysis.
Outcome by Treatment SettingAs shown in Fig. 4, the response rate, treatment duration, and treatment discontinuation rate of CT-P6 therapy varied among the five treatment settings throughout the different stages of gastric cancer treatment. Patients receiving first-line postoperative therapy within 3 months after noncurative resection (group B) could not achieve CR or PR owing to the absence of measurable lesions and were all assessed as SD. Nevertheless, their treatment duration was significantly long, and the treatment discontinuation rate was the lowest among the five patient groups. Tumor response and treatment duration were similar in patients at first-line therapy for inoperable advanced tumors (group A) and those at first-line therapy for recurrence after curative resection (group C). In contrast, patients at second-line therapy for recurrence after postoperative adjuvant therapy (group D) and those who received second- or later-line therapy for recurrence after chemotherapy (group E) had relatively short treatment durations and higher rates of treatment discontinuation due to disease progression.
Fig. 4
Differences in outcomes by CT-P6 treatment setting in HER2-positive advanced gastric cancer. a Tumor response based on all physician-reported assessments, b treatment duration, and c treatment discontinuation rate. *p < 0.05, **p < 0.01, #Patient decision and hospital policy, CR, complete response; PR, partial response; SD, stable disease
In the comparison between first-line therapy (group A + B + C) and second- or later-line therapy (group D + E), no significant differences were observed in ORR (32.5% versus 30.8%) or DCR (84.2% versus 84.6%). However, first-line therapy had a significantly longer treatment duration compared with second- or later-line therapy (182 versus 142 days, p < 0.05) and a lower discontinuation rate due to disease progression (48.0% versus 68.3%, p < 0.05). The incidence of treatment-related adverse events of grade ≥ 3 was similar among these patient groups, ranging between 25.0% and 35.3% (data not shown).
Outcome by RegimenPrimarily, S-1 (103 patients) and capecitabine (45 patients) were used in combination with CT-P6, with 5-FU used in 8 patients. Platinum agent was not combined with fluoropyrimidine in 24 patients, and the remaining patients received either oxaliplatin (109 patients) or cisplatin (23 patients). There were no significant differences in response rates or treatment duration between S-1-containing and capecitabine-containing regimens. The response rate to fluoropyrimidine plus CT-P6 without platinum agent was very low (4.3%). The rate was higher at 33.3% when combined with oxaliplatin and higher still at 59.1% (including 9.1% CR) when combined with cisplatin. In addition, cisplatin-containing regimens enabled 18.2% of patients to proceed to conversion surgery, although the rate of treatment discontinuation due to adverse events was relatively high (13.6%). Consequently, its treatment duration was comparable to the oxaliplatin-containing regimens (Supplementary Fig. S1).
Comments (0)