
Remember me



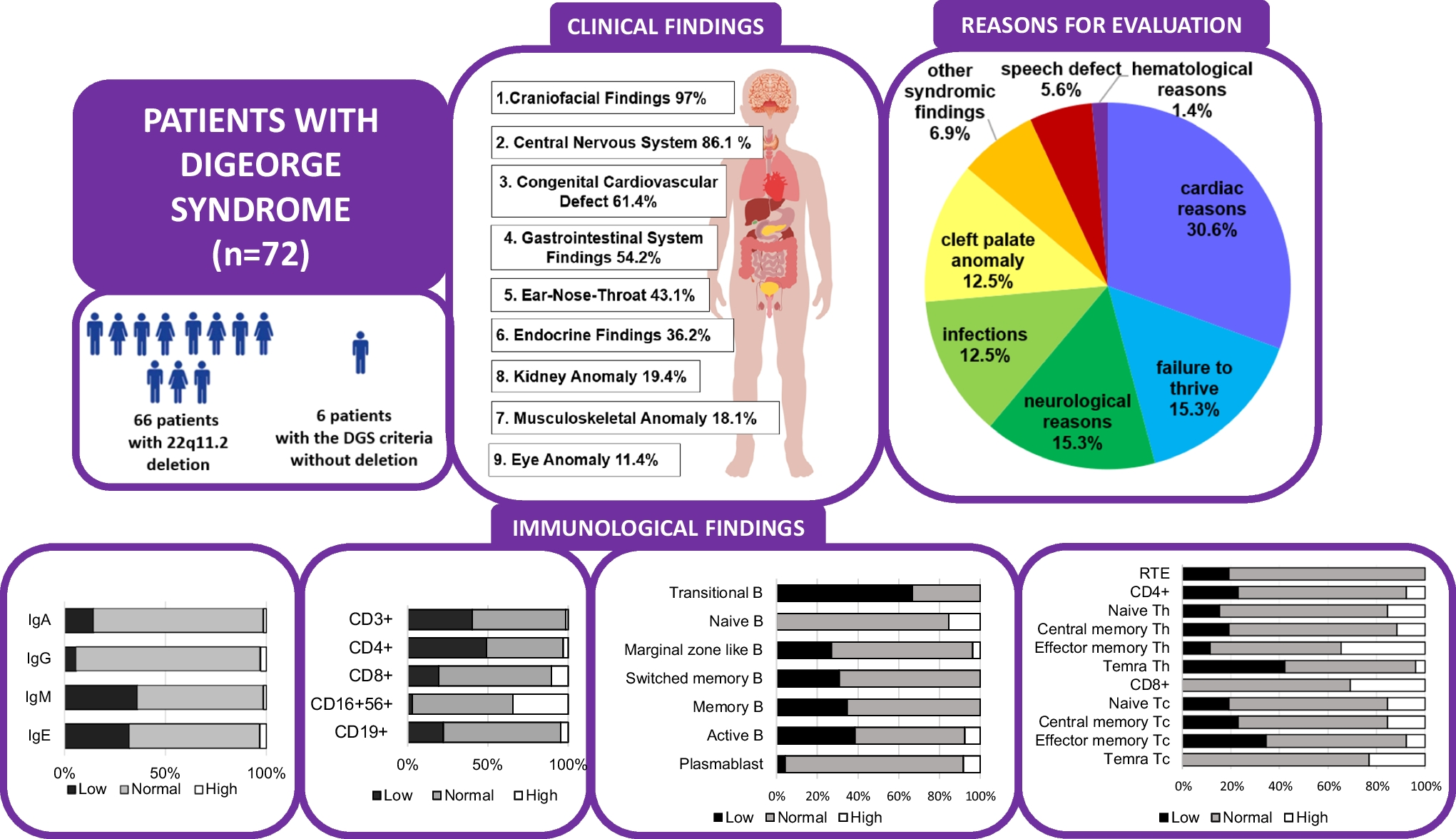

A seventeen-year-old male patient presented with widespread pustules, ulcers, and crusty skin affecting the entire body, including the scalp, since the age of forty days. There was no parental consanguinity. Dermatologic examination revealed occasional hemorrhagic dry ulcers, pustules, and hypopigmented atrophic scars on an inflammatory background. These lesions were rare on the trunk but most prominent on both lower extremities (Fig. 1A). Almost complete hair loss and atrophic scarring were observed on the scalp. No pathological findings were noted in other systemic examinations. Laboratory investigations showed microcytic anemia (hemoglobin 10 g/dL and MCV 66 fL) and elevated acute phase reactants: serum amyloid A (107 mg/L; normal 0–6,8 mg/L), C-reactive protein (39 mg/L; normal 0–5 mg/L), and erythrocyte sedimentation rate (27 mm/hour; normal 2–20 mm/hour). Peripheral blood flow cytometry demonstrated a decreased number of class-switched B cells (6,6 cells/µl). Elevated serum IgA (533 mg/dL) and IgG (2850 mg/dL) levels suggested ongoing chronic inflammation. Histopathologic evaluation of a skin biopsy revealed tissue rich in keratinocytes.
Fig. 1
A. Crusted scars and ulcerated lesions on the lower extremities. B. No new ulcers observed on the lower extremities after six months of baricitinib treatment
Prior to presentation at our clinic, the patient had been diagnosed with various conditions, including atopic dermatitis and psoriasis. He was treated with conventional topical therapies, including corticosteroids and topical tacrolimus, without significant clinical benefit. Additionally, he had received monthly intravenous immunoglobulin (IVIG) therapy for three years. We discontinued IVIG after observing no regression in skin lesions and subsequently initiated Anakinra at 200 mg/day for six months. However, Anakinra treatment failed to achieve significant improvement.
Clinical exome sequencing identified three variants in the NLRP1 gene: Chr17:5433995 C > T:NM_033004:exon12:c.G3326A: p.R1109H (paternal, CADD score 0.707, rare), Chr17:5462417 C > A:NM_033004:exon4:c.G1599T: p.Q533H (paternal, CADD score 26.2, 10 homozygotes in gnomAD), Chr17:5487069 G > T:NM_033004:exon1:c.C209A: p.A70D (maternal, CADD score 21.9, very rare). The A70D variant affects the pyrin domain, potentially enhancing the interaction between adapter proteins and prolonging caspase activation. Based on the identification of NLRP1 mutations, baricitinib, a Janus kinase (JAK) inhibitor, was initiated at a dose of 4 mg/day. Clinical improvement was evident by the second month of treatment, with a marked therapeutic response observed by the sixth month, including substantial healing of skin lesions. Baricitinib therapy was associated with a reduction in inflammation, facilitation of ulcerated tissue repair, and prevention of contractures and post-inflammatory scarring (Fig. 1B). At 22 months, a disease flare occurred, attributed to the temporary unavailability of baricitinib within the country. Nevertheless, by month 25, clinical stability was reestablished without further flares or the requirement for additional systemic therapy. No adverse events were documented during the two-year follow-up period.
Comments (0)