Chronic kidney disease is defined as abnormalities of kidney structure or function, present for a minimum of 3 months, with implications for health. The best-recognized causes include diabetes, hypertension, and aging. Decreased renal function is represented by GFR < 60 ml/min per 1.73 m2 (GFR categories G3a–G5) with ultrasound changes (renal length and parenchymal thickness reduction) [23].
Global prevalence of CKD in the general population was estimated at 9.1% (8.5 − 9.8%), in 2017, by a systematic analysis [25, 26].
In Italy, the prevalence of CKD is around 7.5% of the adult male population and 6.5% of the adult female population that accounts today for about 2.5 million people affected [27].
According to the Global Burden of Disease study, the prevalence of CKD will increase, over time, driven by population aging, diabetes and hypertension. For this reason, the number of people developing kidney failure and requiring kidney replacement therapy is estimated to increase to more than 5 million by 2030 [25, 26].
Prior studies of CKD in primary antibody deficiencies are scarce and limited to small cohorts. In particular, CKD was reported in a small percentage of patients and in about 2% of CVID patients enrolled in a cohort of 240 UK patients [3,4,5, 28].
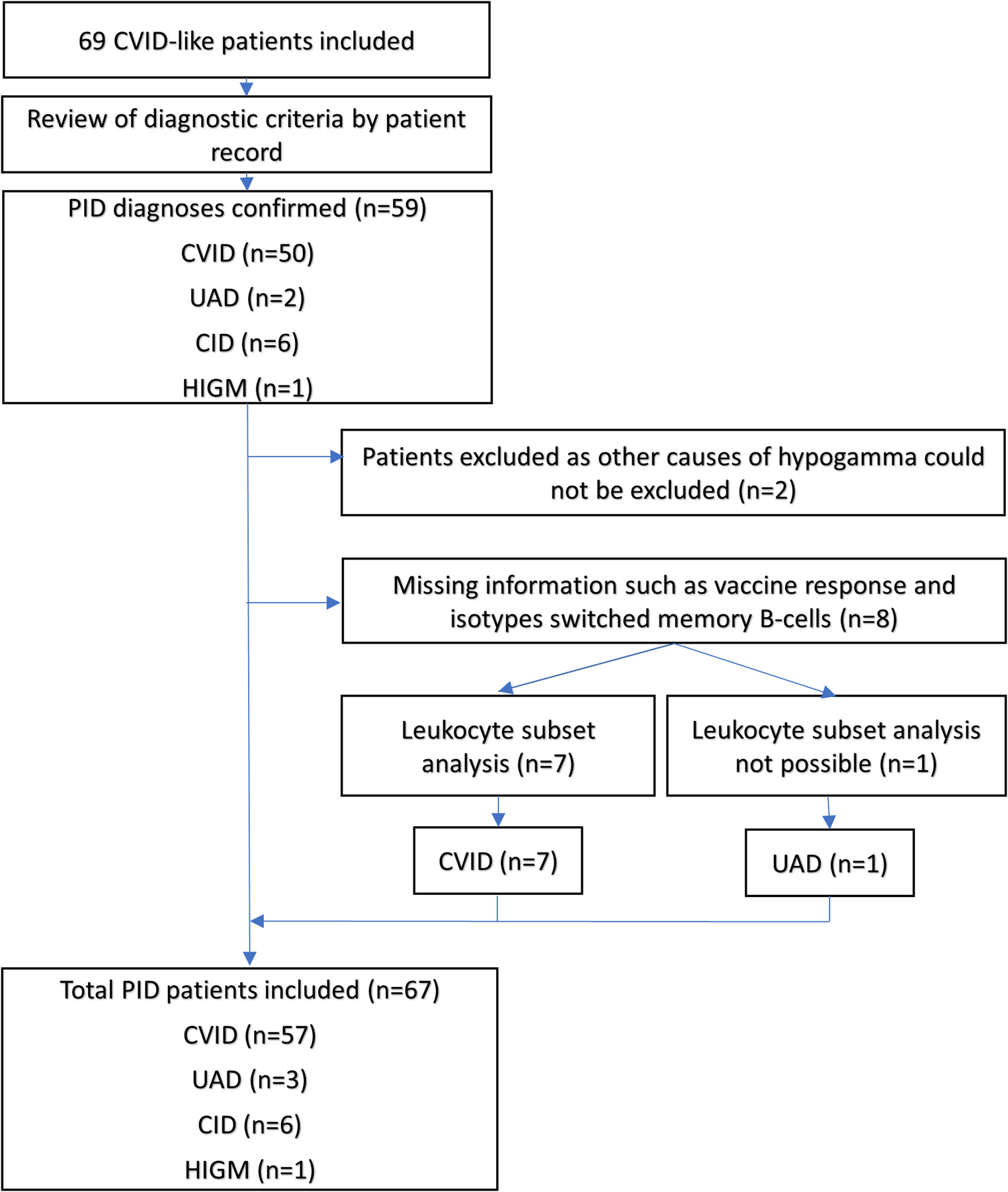
In our cohort of 367 CVID patients, we observed a CKD (GFR < 60 ml/min) prevalence of 6.3%.
Our results are mostly in line with data from the general Italian population and with those recently published [11] on the USIDNET cohort of PAD patients, where 6.8% of patients had renal complications. However, Materne et al. considered in their study all PADs, investigated the prevalence of renal disease with a more general definition, including not just CKD but also nephrolithiasis, nephritis, and other renal diseases and did not specify a GFR-based criterion for CKD. Thus, our CKD prevalence, evaluated only in CVID, has to be considered as higher [11].
In our cohort, CKD is almost completely attributable to age, even when other risk factors such as hypertension, diabetes and dyslipidemia also present in the general population were present.
The association between renal disease and these comorbidities is in line with the progressive aging of our cohort, a probable consequence of improved survival observed in the last years due to the efficacy of modern tailored care and of treatment availability [29]. This is likely the main reason why our prevalence of CKD shows a trend towards the global prevalence and seems to move away from the prevalence reported in older studies.
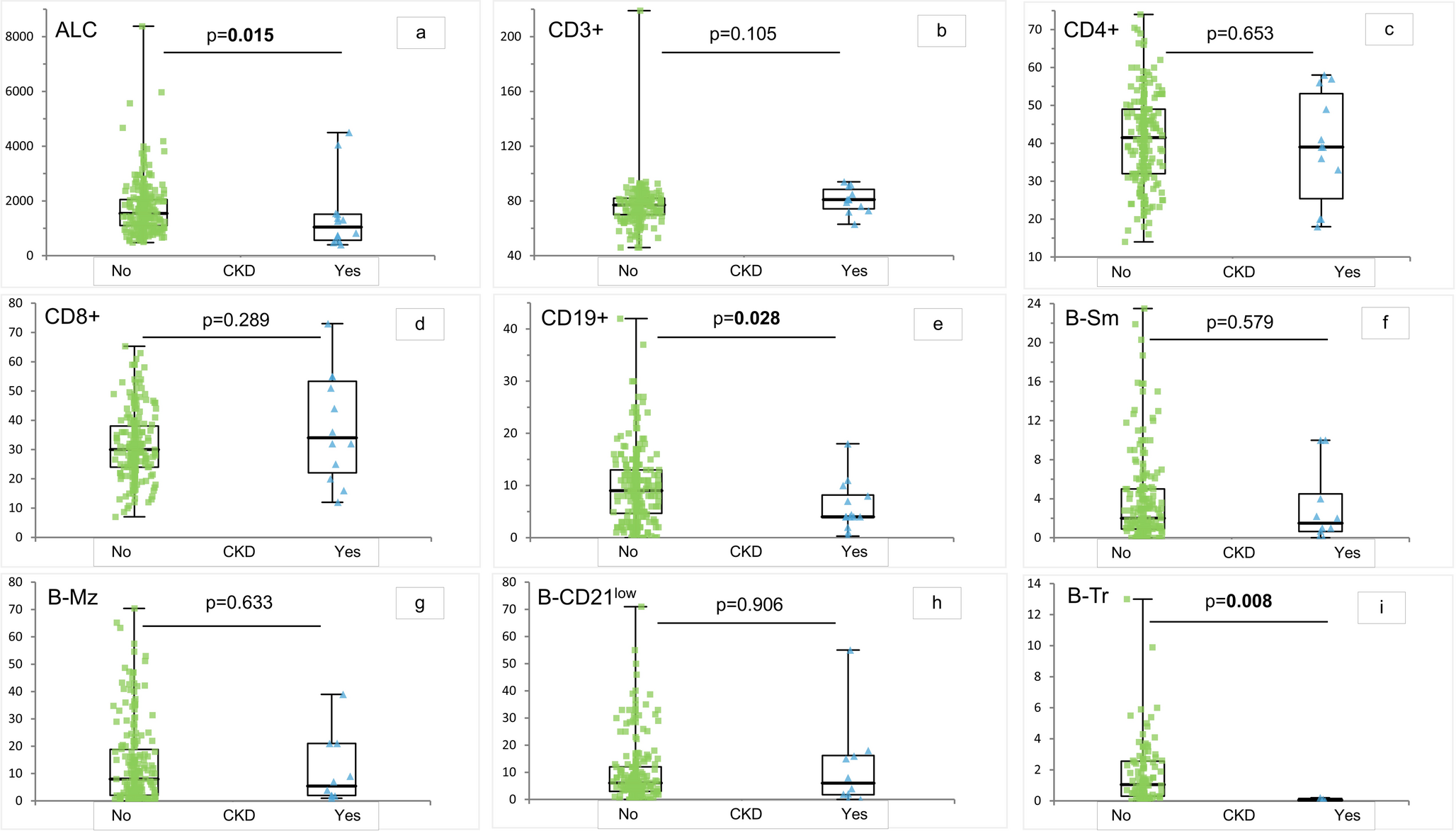
Due to the retrospective design of the study and to the lack of precise information in the clinical records, particularly before CVID diagnosis and regarding patients with a long disease history, we were not able to weigh the number and severity of infections in relation to CKD development. We could only compare the well-known markers of infectious risk such as IgG and IgA levels at diagnosis, memory B cells, IgGTL, bronchiectasis and need for antibiotic prophylaxis. These parameters did not differ significantly between CKD and no CKD patients. Analyzing non-infectious CVID-related complications, we did not observe a significant association between complicated phenotype and CKD, but, also after age-adjustment, we found an increased risk for patients with autoimmune cytopenia that, compared to the other immune-mediated complications, almost always requires glucocorticoids and eventually immune-suppressive treatment. In addition, lymphocytes subsets, the median absolute count of total lymphocytes and the percentage of total B and transitional B cells were significantly reduced in the CKD group whereas class-switched memory B cells were lower, even if without statistical significance. In the general population, CKD has been associated with a reduced total lymphocytes count [30]. Class-switched memory B cells reduction is known to be associated with a higher risk of developing immune dysregulation, including autoimmune cytopenia [11, 31]. A reduction of transitional B cells, as found in our CKD group, seems also to be associated with immune dysregulation [32]. These cells are indeed involved in regulatory processes including the conversion to regulatory T cells. We could speculate that the alteration of the immunological phenotype of a subgroup of CVID patients may influence the inflammatory background and favor chronic organ damage, as already highlighted in pulmonary, gastroenteric tract and cardio-vascular manifestations [3, 33–34]. The lymphopenia may also explain the higher rate of trimethoprim-sulfamethoxazole prophylaxis use in CKD patients. Accordingly, we also reported a higher prevalence of COPD and CKD in our cohort, a well-known association also in the general population [35]. In fact, the vicious circle infection-inflammation [36], typical of COPD, might explain the use of trimethoprim-sulfamethoxazole antibiotic prophylaxis, in the attempt to prevent lung damage and remodeling [37]. Notably, compared to azithromycin, trimethoprim-sulfamethoxazole prophylaxis was commonly used also to prevent PCJ infection in patients with severe lymphopenia or in those receiving glucocorticoids or immune-suppressive treatment (for example, in case of AI cytopenia). We know that inflammation is a common feature of CVID, explained both by immune dysregulation and infectious events [38]. In line with an increased inflammatory milieu and with the presence of lymphopenia, the neutrophil-to-lymphocyte ratio, a prognostic marker of worse renal outcomes [18], and CKD showed a positive correlation by binomial logistic regression analysis, corrected for age, supporting a more pronounced inflammatory state in patients with renal and cardiovascular comorbidities [33, 39].
Regarding Ig replacement therapy, as supported by the age-adjusted analysis, the higher prevalence of IVIG use in the CKD cohort might be mainly related to the older age of the CKD patients, who tend to prefer a hospital-based rather than a home-based immunoglobulin administration. In fact, in Italy, IVIG is administered only in a hospital setting, allowing for a more frequent contact between patients and medical staff. This is supported also by other studies where older patients, displaying a severe phenotype and a high rate of complications, still preferred the IVIG compared to the SCIG treatment [40].
Finally, in CVID patients who developed CKD, as expected, we observed a significant association with ultrasonography alterations including changes in cortico-medullary differentiation and longitudinal bipolar diameter at US, mainly related to arterial hypertension and cardiovascular risk factors, as well as pyelectasis and nephrolithiasis. This latter might induce an obstruction of the urinary tract that alters the urinary flow and might further promote infections and renal damage over time in patients with increased infectious burden [41].
Our study has some limitations, mainly due to the retrospective design and unavailability of data exactly reporting the time of CKD onset and its evolution, as well as the exact number of infectious episodes and antibiotic courses. Furthermore, results of the genetic screening were not available for the whole cohort. However, the number of enrolled patients, coming from a single Country and with homogenous ethnicity, makes it a valuable source of information on a poorly investigated issue.
In summary, CKD in CVID is largely related to aging and age-related comorbidities, together with disease-related immune dysregulation and inflammation. So, autoimmune cytopenia, lower B cell percentage, increased neutrophil-to-lymphocyte ratio and need of trimethoprim-sulfamethoxazole rather than azithromycin antibiotic prophylaxis may help to identify a subgroup of patients with a more “inflammatory” phenotype that over time promote the development and worsening of CKD, besides the clear effect of age.





Comments (0)