
Remember me




Twenty patients with confirmed diagnoses of SCID were included for data analysis, of which sixteen were typical SCID, three were leaky-SCID, and one had Omenn Syndrome (Table 1). A higher number of diagnoses were observed in 2020–2021 (n = 7), coinciding with the period of the NUPAD-UFMG pilot NBS program for SCID.
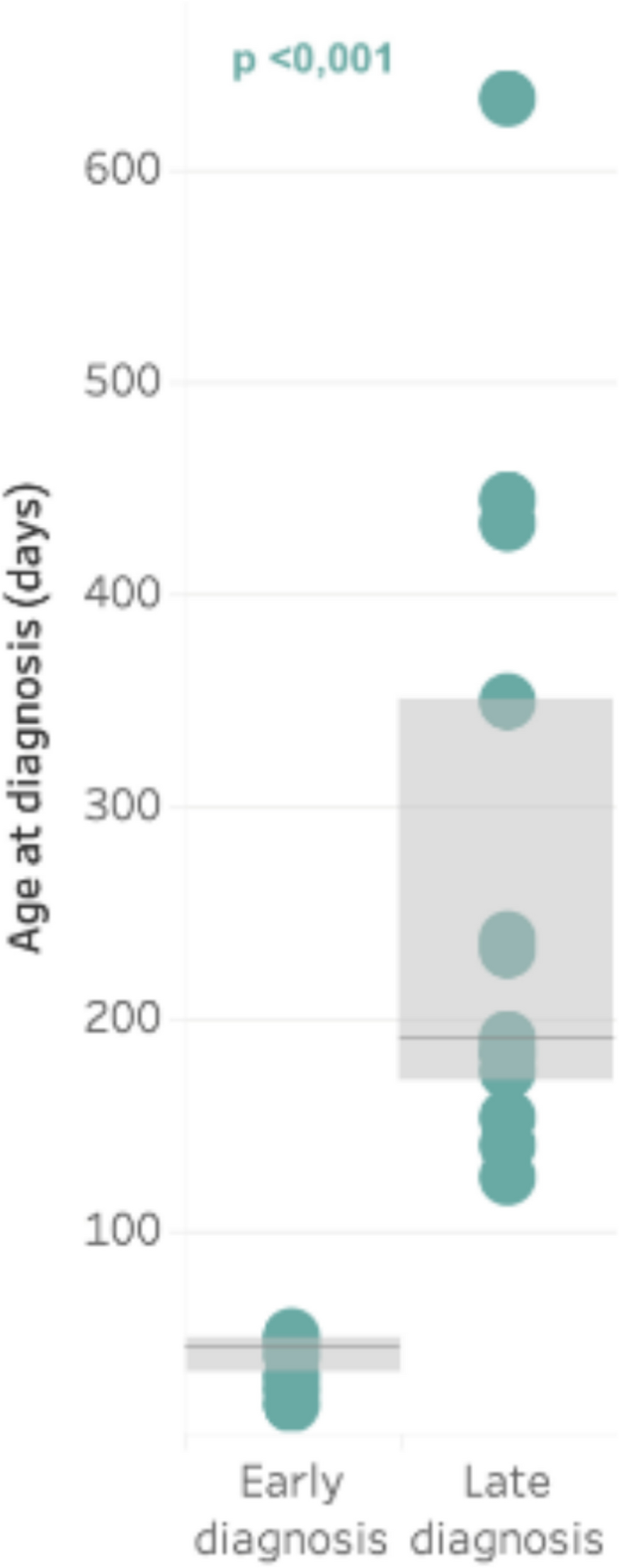
Table 1 Demographic, laboratory, phenotypic, and genotypic profile of the study populationThe male-to-female ratio was 4:1. Only seven patients were diagnosed early at birth. Of these seven, six were referred to the service from the NBS for SCID, and one, due to family history, had the opportunity for curative treatment with HCT. Thirteen children were diagnosed late by clinical presentation; five had severe infections at diagnosis and died within a few months; one was lost to follow-up, one died while awaiting HCT, and the other six were transplanted (Table 2). The overall median age at diagnosis was 164 days (IQR: 47–233), with the oldest age being 633 days in a child diagnosed as leaky-SCID (P11), and the youngest age was 18 days in a patient from NBS. The median age at diagnosis in the group of early diagnosis patients was 41 days (IQR: 28–47; ranging from 18 to 50 days), contrasting with the median age of those patients diagnosed later, by clinical history, of 190 days (IQR: 175–349; ranging from 125 to 633 days) (p < 0.001). (Fig. 1).
Table 2 Clinical characterization of patients and outcome After HCTFig. 1
Comparison of age at diagnosis between early and late diagnosis groups. MW: Mann–Whitney Test. Early diagnosis: by NBS or positive family history; Late diagnosis: by clinical presentation
Consanguinity was present in more than half of the families for which these data were available (8 out of 15 patients). A history of early deaths in the family was found in 9 of 18 patients (50%), with only one family (P5) having received genetic and immunological counseling.
VaccinationAll patients received the Bacillus Calmette-guérin (BCG) vaccine at birth, except for patient P5. Eighteen of the twenty patients had records in their medical files regarding the presence or absence of alterations secondary to vaccination. Eight of these eighteen patients (44.4%) experienced some complication related to the BCG vaccine, with 5 (62.5%) having a loco-regional reaction (BCGitis) and 3 (37.5%) with disseminated disease (BCGosis). The six patients from the NBS started prophylaxis with Rifampicin and Isoniazid upon diagnosis, and only one (0.17%) patient presented a loco-regional reaction, treated with a quadruple regimen (Rifampicin, Isoniazid, Ethambutol, and Clarithromycin), without complications. The group of patients who were diagnosed later presented more severe complications after vaccination, including disseminated BCGosis. Three patients in this group have BCG complications associated with their death’s causes (Table 3). Patients with later diagnoses had also received other live agent vaccines, such as rotavirus and yellow fever, according to the vaccination schedule established by the Brazilian National Immunization Program. After this vaccination, one patient (P14) had severe encephalitis from Yellow Fever.
Table 3 Genetically undefined SCID patientsLaboratory, Phenotypic, and Genotypic ProfileFifteen out of nineteen patients (78%) presented severe absolute lymphopenia in the blood count with lymphocytes < 2,500 cells/μL of blood at the time of diagnosis. One patient did not have a record of the absolute lymphocyte count. Three patients (P1, P7 and P8) had CD3 + lymphocytes > 300 cells/μL. They were included in this historical series because they met the minimum criteria for the diagnosis of SCID established in 2009 [21, 40], and were diagnosed before 2015 [21, 40]. Six out of nineteen patients (31.5%) presented hypogammaglobulinemia associated with lymphopenia at diagnosis, and one patient did not have a record of the immunoglobulin G (IgG) value. Out of the nine patients who underwent TREC screening, 8 had undetectable values, and one presented a result of 2.3 copies/μL of peripheral blood (normal range > 25 copies/μL) (Table 1).
The most prevalent phenotype was T-B + NK + with seven patients (35%), followed by T-BlowNK + with four patients (20%), T-B-NK + with three patients (15%), T-B-NK with two patients (10%), and T-BlowNK- with one patient (5%). In three patients (15%), B lymphocyte and NK cell counts were not performed due to the unavailability of the service and the severity of the condition at diagnosis.
Genetic analysis through next-generation sequencing revealed mutations in hemizygous in the IL2RG gene (4 patients), in homozygous in RAG1 (2), CD3δ (2), IL7R (1), and in compound heterozygous in ADA (1) and PNP (1). Nine patients did not have a genetic diagnosis. Three of them showed mutations in heterozygous (JAK3 (1), LIG4 (1), and RMRP (1)) that do not explain the disease. One did not present a mutation in the genetic panel of 17 genes for SCID available at the service (IL2RG, JAK3, ORAI1, GATA2, RAG1, RAG2, LCK, ADA, PNP, CD3D, CD3G, CD3Z, CD3E, IL7R, LIG4, DCLRE1 C, NHEJ1). Five of these patients were not submitted to genetic analysis due to the unavailability of the test at the time. Despite not having a genetic diagnosis, all of them met the minimum criteria of clinical and immunophenotyping for Severe Combined Immunodeficiency (SCID) (Tables 1, 3) [21, 40].
Clinical Characterization of Patients and Final OutcomeTable 1 outlines the evaluated patients’ key demographics, laboratory characteristics, phenotypic, and genotypic profiles.
Several patients did not receive a genetic diagnosis. Nonetheless, they met the clinical and immunophenotyping criteria [21, 40] for Severe Combined Immunodeficiency (SCID) (Tables 1, 3). Specifically, patients P12, P14, and P20 presented with heterozygous mutations in the JAK3, LIG4, and RMRP genes, respectively. P12 presented with BCGitis and acute otitis media requiring intravenous antibiotic therapy. P14 had yellow fever encephalitis (post-vaccination) and died at the time of diagnosis. Despite undergoing genetic counseling, this family had another baby with the same mutation and identical immunophenotyping, but in homozygous form. This infant was not included in this analysis as they were born after the data collection period for this study. P20 had a TREC of zero copies in NBS and CD3 < 300 cells/μL. He started prophylactic therapy promptly after diagnosis and had no infections until HCT (Tables 3, 5). Patient 1 (P1) was admitted to the hospital at 3.5 months of age due to gastrointestinal sepsis, disseminated candidiasis, failure to thrive, and BCGitis. She was diagnosed at 5 months of age, but despite all medical interventions, she passed away within one month of her diagnosis (Table 1).
The patients were divided into two groups, early and late diagnosis, to assess the impact of early diagnosis on the disease outcome. The timing of diagnosis was also considered to evaluate whether the infection status before HCT at different ages would directly impact the survival of these patients after HCT. After the diagnostic confirmation with lymphocyte immunophenotyping, antimicrobial prophylaxis were started according to the Latin American Consensus on managing patients with SCID of 2019 [43].
Early DiagnosisOut of the seven patients diagnosed early, only 1 (P16) had been hospitalized before diagnostic confirmation at 30 days of life due to difficult-to-treat acute otitis media, requiring intravenous antibiotic therapy. During follow-up, even with appropriate prophylaxis, 5 of 7 patients (71.4%) were admitted to the ward to treat infectious events (Table 2), requiring parenteral antibiotic therapy without serious complications. Five of the seven also presented confirmed infection by RT-PCR for COVID-19 with mild symptoms. Patient 18 developed drug-induced hepatitis at 7 months. It was impossible to return to antimicrobial prophylaxis after repeated attempts, opting for rigorous observation and maintaining prophylaxis only with intravenous human immunoglobulin until HCT was performed (Table 2).
All patients in this group underwent curative treatment with HCT. The median age of patients at HCT was 380 days (IQR: 251–571; ranging from 185 to 623 days), and the median time between diagnosis and transplantation was 330 days (IQR: 226–524; ranging from 167 to 582 days) (Table 4). The earliest HCT was performed at 6 months of life (185 days), and the latest at 1 year and 8 months (623 days). One patient (P19) had failed to thrive since birth and had been hospitalized on two occasions previously. This patient underwent HCT at 9 months but succumbed to complications in the immediate post-HCT period. As the patient underwent HCT in another service, it was impossible to access clinical evolution details (Table 2). Patient P15 underwent HCT at 11 months of life (348 days) after treatment for acute CMV gastroenteritis, and the procedure was successful. However, a year after the transplant, he presented with an acute respiratory infection without a defined agent, which evolved into respiratory failure and death at 1 year and 11 months. Therefore, in this group of patients with early diagnosis, 5 out of 7 (71.4%) were successful in HCT and are alive and well, all with more than 3 years of follow-up. Although no patient underwent transplantation before 3.5 months of life, it was observed that the two patients who did not present infectious episodes before the procedure were alive at more than 3 years of age. Only three of the five patients who had infectious episodes before HCT survived (60%) (Table 2).
Table 4 Relationship of the time interval between diagnosis and HCT for patients with early and late diagnosisLate DiagnosisThirteen out of the twenty patients studied (65%) were diagnosed later due to clinical presentation. Of these thirteen, five (38,5%) presented with severe infection at diagnosis, requiring admission to an intensive care unit (ICU) and leading to death during the first hospitalization, and one (P4) died at a second infection while waiting for HCT (Table 5). Of the remaining seven, one patient (P7) discontinued follow-up at the service after diagnosis, making it impossible to access the outcome data. The other six patients in this group underwent HCT (P2, P6, P8, P11, P12, P13). Of these six, two died after the procedure, and four (66%) were alive at the last evaluation, with a median follow-up time of 9 years (ranging from 7 years and 6 months to 16 years) (Table 2).
Table 5 Causes of death after late diagnosis and before HCTHCTThe median age of patients at HCT was 539 days (IQR: 400–1022; ranging from 328 to 3294 days), with no significant difference from the early diagnosis group (380 days; p = 0.234). (Table 4). The earliest HCT was performed at 12 months of life (335 days) and the latest at 9 years (2851 days) (Table 4). The median time between diagnosis and the transplant was 322.5 days (IQR: 225–426; ranging from 96 to 2851 days), similar to the median found in the early diagnosis group (330 days; p = 0.731) (Table 4).
Survival OutcomeThe percentage of survivors in the study population was 47.3% (9 out of 19 patients, excluding one patient who was lost to follow-up), with a median follow-up time of 7 years (ranging from 3 to 15 years). As no patient in this cohort underwent HCT before 3.5 months of age to assess the direct impact of early transplantation on survival, we evaluated the effect of early diagnosis (at birth or by positive family history) on survival.
The 2-year overall survival (OS) of the whole group was 45.3% (95% CI 22.3–68.2%) (Fig. 2a). Comparing the 2-year OS between the early diagnosis group at 71.4% (95% CI 37.8–100%) and the late diagnosis group at 29.2% (95% CI 1.9–56.4%), we found a trend towards a statistically significant difference between the two groups (p = 0.053), showing that early diagnosis can directly impact the survival of patients with SCID (Fig. 2b).
Fig. 2
Overall survival analysis. Kaplan–Meier, Log-rank Test (time in months). Early diagnosis: by NBS or positive family history; Late diagnosis: by clinical presentation. a Overall Survival of the whole group (early and late diagnosis) during Follow-up. b Comparison of Overall Survival of all patients with Early vs. all patients with Late Diagnosis. c Comparison of Overall Survival in Patients with Early vs. Late Diagnosis who had the opportunity to undergo HCT
The percentage of survivors among patients who had the opportunity to undergo HCT was 69.2% (9 out of 13 patients – Table 2). Comparing the 2-year OS of this group of patients, we observed very similar rates between the two groups, 71.4% (95% CI 37.8–100%) for patients in the early diagnosis group vs. 60% (95% CI 17–100%) for patients in the late diagnosis group (p = 0.774), suggesting that early diagnosis alone may not directly impact survival after HCT (Fig. 2c). While waiting for HCT, many patients had infections, which may have contributed to the authors not finding a difference in OS between the two groups (p = 0.774).
Assessing the impact of prior infections on clinical outcomes before HCT, we found a significant difference in the percentage of survivors between patients who underwent transplantation without prior infection and those who underwent transplantation after experiencing infectious conditions. In patients who did not present an infection before HCT, we found a survival percentage of 100% (2 out of 2 patients). In contrast, in those who had an infectious episode before HCT, we found a survival percentage of 60% in the early diagnosis group and 66.6% in the late diagnosis group. However, a statistical comparison was impossible due to the small number in each group, and the late diagnosis without infection group had no representatives.
Comments (0)