
Remember me
Of the 58 patients initially considered, 40 were included in the final analysis based on having completed at least 24 weeks (6 months) of follow-up from the initiation of BKZ therapy. The remaining 18 patients were excluded because they had not yet reached the 6-month follow-up milestone at the time of data collection. The median age was 55.0 years (47.4–62.0), with female patients representing 50% of the cohort (20/40). The median BMI was 27.0 (24.0–29.3), with 6 out of 40 (15%) classified as obese. Full demographic details are summarized in Table 1.
Table 1 Demographic characteristics of patients enrolled in the studyMost patients (35/40) were managed in combined dermatology–rheumatology clinics. In 31 of the 40 cases (77.5%), BKZ was initiated to address both active joint and skin involvement, while in the remaining 9 cases (22.5%), treatment was started primarily because of active joint disease. The most commonly adopted dosing regimen was 320 mg every 8 weeks, administered in 35 patients (87.5%). In these patients, treatment was initiated with an induction regimen, consisting of 320 mg administered at weeks 0, 4, 8, 12, and 16. At baseline, the median DAPSA score was 22.9 (17.9–28.7), SJC 3.0 (0.8–5.3), and TJC 4.5 (3.0–7.3). Dactylitis was present in 6 patients (15%), while median LEI was 0.0 (0.0–1.3). Only two patients (5%) were in DAPSA LDA at baseline and none in DAPSA remission. Vulgar psoriasis was the predominant skin phenotype, present in 36 out of 40 patients (90%) with a median PASI score of 13.0 (4.4–16.0). Nail involvement was documented in 17 out of 40 patients (42.5%),
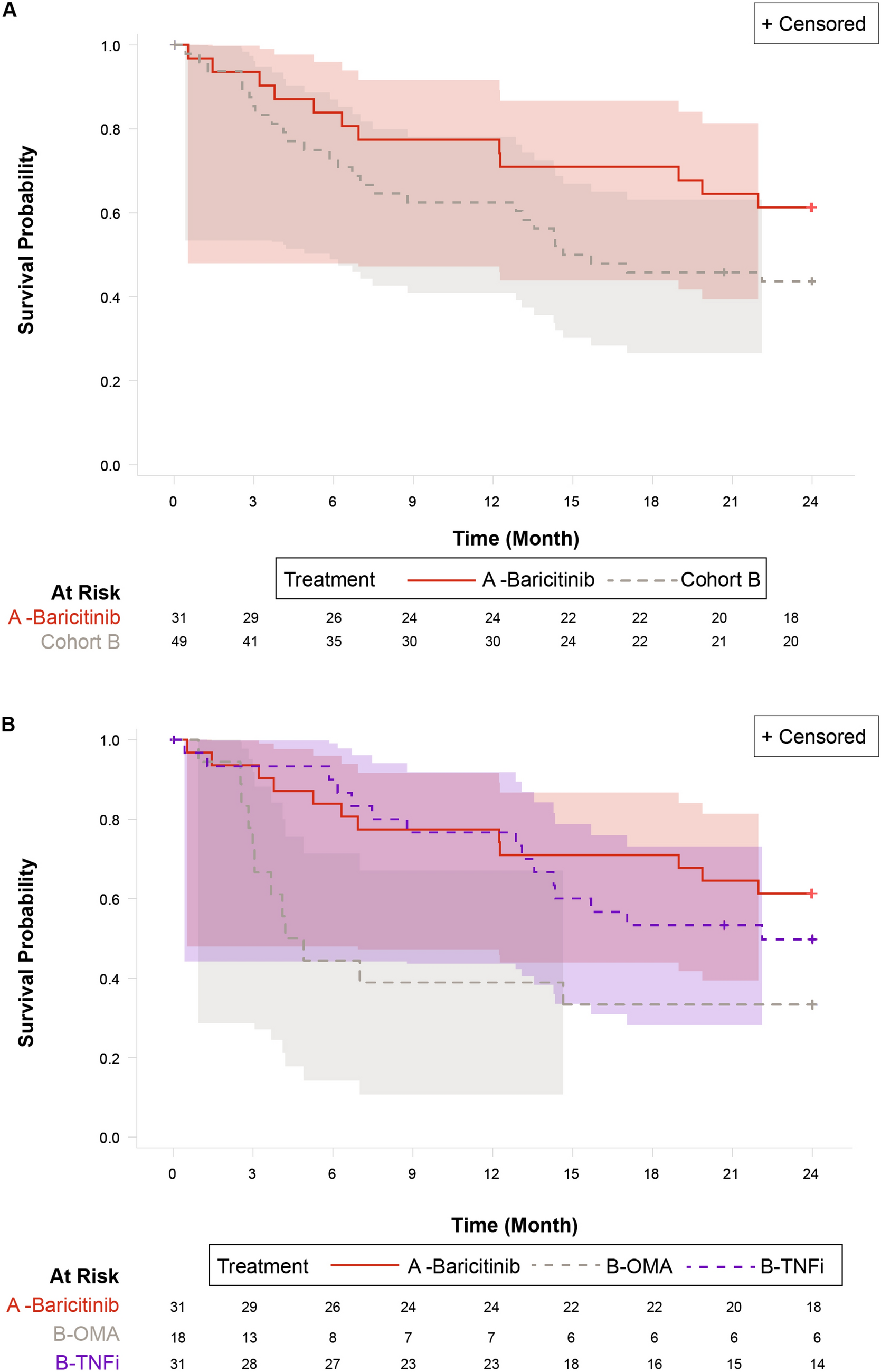
History of Previous b/tsDMARDs FailurePrior to initiating BKZ, most patients had experienced multiple treatment failures. The median number of previously failed b/tsDMARDs was 3.0 (2.0–3.3), and the median number of failed mechanisms of action was 2.0 (1.8–3.0). Among the 40 patients included in the analysis, 30 (75%) had failed at least two different classes of b/tsDMARDs and were therefore classified as having D2T-PsA (Fig. 1A, B) [17, 18, 22,23,24]. Regarding prior biologic and targeted synthetic therapies, tumor necrosis factor inhibitors (TNFi) were the most frequently used (92.5%), followed by IL-17Ai (62.5%), while IL-23 inhibitors (IL-23i) and JAK inhibitors (Jak-i) were prescribed less frequently (Fig. 1C).
Fig. 1
A, B Number of prior b/tsDMARD class failures before initiation of BKZ; C Previous b/tsDMARDs classes failed. bDMARDs biologic disease-modifying antirheumatic drugs, tsDMARDs targeted synthetic disease-modifying antirheumatic drugs, TNFi tumor necrosis factor inhibitors, IL17Ai interleukin-17A inhibitor, IL-23i interleukin-23 inhibitors, Jak-I Janus kinase inhibitors
Three out of 40 patients received BKZ as their first-line b/tsDMARD because of concomitant moderate to severe skin involvement. The treatment decision in all these cases was made within a combined dermatology–rheumatology clinic setting.
Effectiveness of BimekizumabAt week 24, BKZ was maintained in 37 out of 40 patients (92.5%). Three patients (7.5%) discontinued BKZ because of lack of efficacy: one due to primary inefficacy, and two following disease reactivation at week 24 despite partial improvement at week 12.
Disease activity, as measured by DAPSA, showed a marked improvement, with scores decreasing from 22.9 (17.9–28.7) at baseline to 10.7 (6.9–13.6) at week 12 (p < 0.001), and further to 6.0 (3.1–12.8) at week 24 (p < 0.001) (Fig. 2). By week 24, 29 out of 40 patients (72.5%) had achieved at least LDA, and 10 out of 40 (25%) reached DAPSA remission.
Fig. 2
Trends in DAPSA and PASI during follow-up. DAPSA Disease Activity in Psoriatic Arthritis, PASI Psoriasis Area and Severity Index
As shown in Fig. 3, treatment with BKZ led to a rapid and significant improvement in peripheral joint involvement. Median SJC decreased from 3.0 (0.8–5.3) at baseline to 0.0 (0.0–2.0) at week 12 and 0.0 (0.0–1.0) at week 24 (p < 0.001 for both). TJC showed a similar trend, dropping from 4.5 (3.0–7.3) at baseline to 2.0 (0.0–2.0) at week 12 and 1.0 (0.0–2.0) at week 24 (p < 0.001) (Table 2).
Fig. 3
Trends in DAPSA variables over time. SJC swollen joint count, TJC tender joint count, VAS visual analog scale, PGA Patient Global Assessment, CRP C-reactive protein
Table 2 Comparison of clinical and laboratory parameters during the study periodAlthough enthesitis was infrequent at baseline (as assessed by LEI), significant improvement was noted: by week 24, 9 out of 11 patients (81.9%) with enthesitis at baseline had achieved complete resolution (p = 0.011). Dactylitis, initially present in 6 patients (15%), resolved in nearly all cases by week 12, with 1 patient (2.5%) still showing signs of dactylitis at week 24 (p = 0.011).
Patient-reported outcomes (PROs) also improved significantly. Pain VAS and PGA decreased from 7.0 (6.0–8.0) and 7.5 (6.5–8.0) at baseline to 3.0 (2.0–4.3) and 3.0 (2.0–4.0) at week 12 (p < 0.001), with further reductions at week 24 to 2.0 (1.0–5.0) and 2.0 (1.0–4.5), respectively (p < 0.001).
Skin involvement, as assessed by the PASI score, also improved markedly. The median PASI decreased from 13.0 (IQR 4.4–16.0) at baseline to 0.0 (IQR 0.0–2.0) at week 24 (p < 0.001).
Among the 33 patients with baseline PASI ≥ 3, complete skin clearance (PASI 100) was achieved in 11 (33.3%) at week 12, and in 17 (51.5%) by week 24.
Results from the linear mixed-effects model confirmed a statistically significant effect of time on multiple clinical and laboratory parameters (Table 3).
Table 3 Linear mixed model analyses of clinical and laboratory parameters during the study periodSwitch Intra-IL-17i ClassA total of 25 out of 40 (62.5%) patients had been previously treated with IL-17Ai, accounting for 30 treatment courses. Among these, 8 patients (32%) experienced at least one primary failure to IL-17Ai, while the remaining 17 out of 25 (68%) had secondary failures.
In the primary failure group, only 2 out of 8 patients (25%) achieved LDA at 24 weeks, and none reached remission. In contrast, among the 17 patients with only secondary failures, 14 (82.4%) achieved at least LDA at week 24, and 6 (35.3%) achieved DAPSA remission (Fig. 4).
Fig. 4
Proportion of patients with primary or secondary failure to prior IL-17A inhibitors and rates of low disease activity and remission among them. DAPSA Disease Activity in Psoriatic Arthritis, LDA low disease activity, REM remission
At 24 weeks, the median DAPSA score was significantly higher in the primary failure group compared to the secondary failure group (19.3 [13.6–22.3] vs 4.1 [3.0–8.6], p = 0.002).
Safety Profile of BimekizumabNo serious adverse events (SAEs) were reported during the follow-up period. The most commonly observed adverse event was oral candidiasis, occurring in 6 out of 40 patients (15%). All cases were classified as mild by the treating physicians. Importantly, none of these cases led to treatment discontinuation (Table 4).
Comments (0)