In the last few years, the management of RA has improved with the implementation of treat-to-target strategies and the introduction of new therapeutic options, including biologicals and, more recently, JAK inhibitors [28]. Generating evidence of the effectiveness and persistence of these treatments in patients treated in the real world is key to confirming the results shown in RCTs and registries [32, 33]. Here, we describe the characteristics and outcomes of patients with RA treated with baricitinib (cohort A) or with other b/tsDMARD (cohort B) in real-world Spanish clinical setting before the Pharmacovigilance Risk Assessment Committee (PRAC) of the EMA recommendations [28].
In the Spanish subpopulation of this study, patients treated with baricitinib were older, had a longer mean duration of the disease, and included a greater proportion of patients who had previously received b/tsDMARD therapy, although no formal statistical comparison was performed. This suggests that the baricitinib cohort consisted of a more treatment-experienced or refractory population. Longer duration of RA in Spanish patients starting baricitinib mirrors a similar trend among European and non-European patients and the overall European RA-BE-REAL cohort, although we also observed that Spanish patients starting baricitinib were numerically older than those in the European RA-BE-REAL cohort [26, 34,35,36,37,38]. Nevertheless, although a lower proportion of patients were treatment-naïve in the baricitinib cohort (41.9%) (59.2% in cohort B) in alignment with results from the overall European RA-BE-REAL cohort (40% and 61.1% of b/tsDMARD naïve patients in cohort A and B, respectively) [26], the percentages were not as low as in other real-world studies, where less than 30% of the patients were naïve to b/tsDMARDs [35,36,37,38].
Most of the patients treated with baricitinib as monotherapy maintained this regimen throughout the follow-up. After 3 months, 30% of the patients initially on a combined regimen of baricitinib and a csDMARD transitioned to baricitinib in monotherapy, while patients receiving other b/tsDMARDs were less likely to switch to monotherapy (3.7% after 3 months), and changes in their treatment approach tended to occur gradually through the study period. The findings from the clinical trials RA-BEGIN [12], RA-BEAM [13], and RA-BUILD [16] studies demonstrated the superior performance of baricitinib compared to MTX alone and to placebo, regardless of csDMARDs co-treatment, supporting the use of baricitinib monotherapy as a treatment option in clinical practice [39]. Similarly, previous results from a Swedish cohort already pointed to baricitinib being used more frequently as monotherapy than rituximab and TNFi [40]. Moreover, fewer patients were prescribed GCCs at the onset of baricitinib therapy, and among those initially on GCCs, a numerically higher proportion discontinued their use when treated with baricitinib than those on b/tsDMARDs. An analysis of pooled data from previous studies indicated that the effectiveness of baricitinib was not influenced by concurrent use of csDMARDs or GCCs [41]. Although in our study there were variations in the use of concomitant therapies between cohorts, these might be attributed to the distinct profiles of the patients, with baricitinib often being prescribed to an older and more treatment-experienced population. However, current recommendations indicate that concomitant GCCs should be discontinued as rapidly as clinically feasible [7], which could result in a lower number of adverse events in those patients treated with monotherapy or discontinuing earlier the use of GCCs, as previously suggested [42]. Our study did not present safety data. Future research might shed light on this regard.
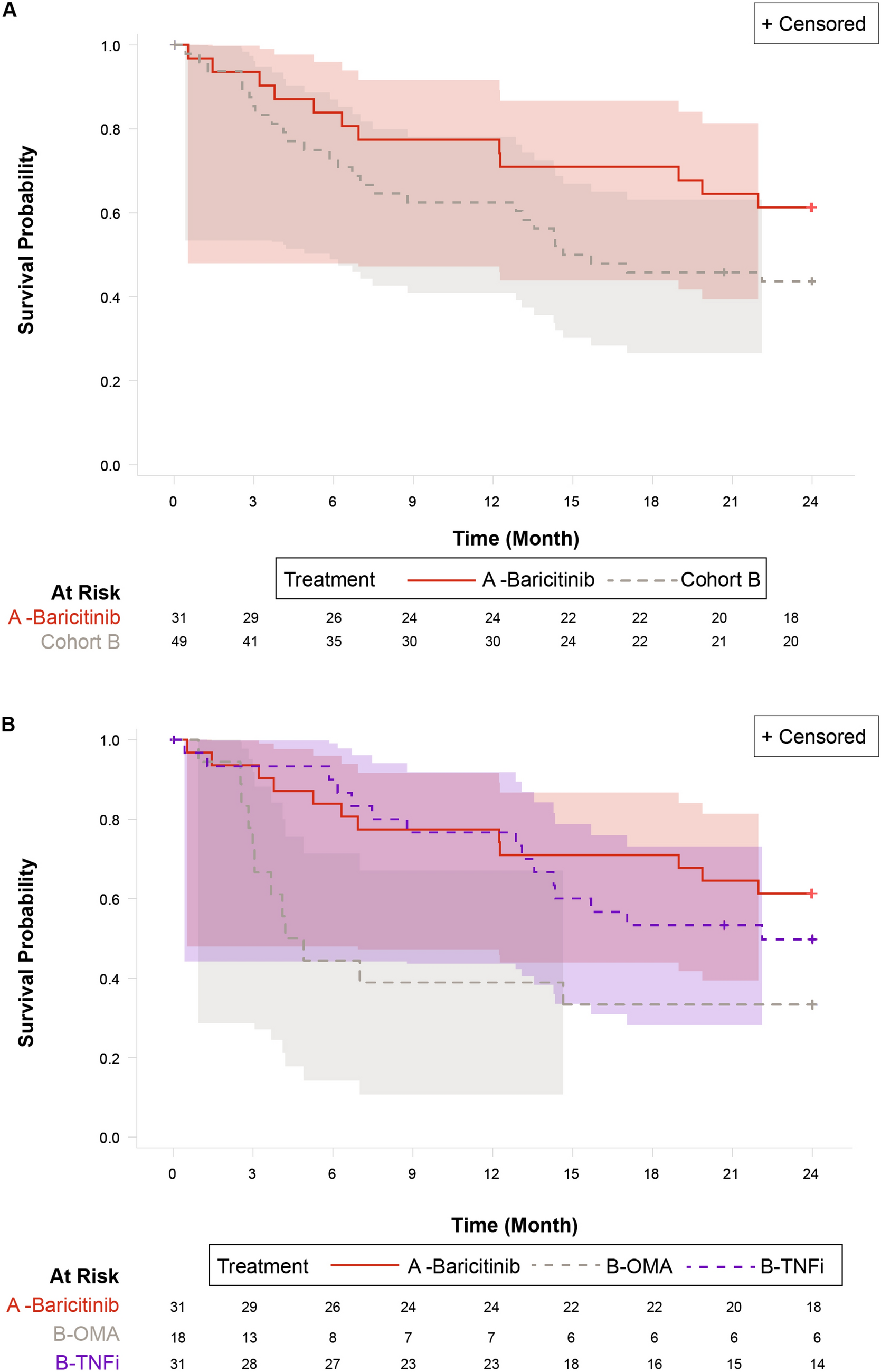
Our results showed that more than half of patients on baricitinib were still on treatment after 24 months. For patients on any other b/tsDMARD, the proportion was two-fifths. While the survival curve almost flattened out at 12 months for the baricitinib cohort, it kept declining for patients in the any b/tsDMARD cohort up to 18 months and then flattened out. The highest decline in drug survival over the 24 months period was observed in the OMA cohort. For the TNFi cohort, however, drug survival declined rapidly after the 12 months follow-up, in line with results observed in other studies [43]. Prior research already pointed to a high survival probability (> 70%) of baricitinib in routine clinical practice at different points in time [38, 44, 45]. This was also seen in the European analysis in the RA-BE-REAL study where, even in treatment-experienced patients, the survival probability of baricitinib after 24 months was 50% [26], while in another real-life study including 139 baricitinib-treated patients, the persistence reached 56.4% after 24 months [46]. Differences in continuation rates between treatments could be explained by the lower percentage of discontinuations due to primary non-response and secondary loss of response with baricitinib and also by the observed lower discontinuations due to adverse events, as suggested in a previous Swiss study [45]. Moreover, a Swedish study pointed to a higher drug survival for baricitinib compared to other treatments, and a Spanish study indicated that the 4-year survival for baricitinib compared with TNF inhibitors was better (HR 0.47, 95% CI 0.24–0.91) [11]. Overall, previous studies show equal or better baricitinib survival than other treatments [11].
Over the 24-month period, mean CDAI scores decreased in both cohorts, showing a consistent reduction in disease activity that was noticeable by month 3. In a prior real-world study which analysed the effectiveness of baricitinib compared to other treatments (273 patients in baricitinib, 154 other tsDMARD, 473 in TNFi and 318 in OMA), similar outcomes were observed, with rates of LDA and remission not differing significantly between treatments [36]. Our results also showed a decrease in the number of swollen and tender joints, with cohort A patients having a more pronounced reduction over the study period. A considerable portion of patients from both cohorts reached either LDA or remission as well. The percentage of patients in cohort A that achieved LDA was 46.4% and in cohort B 29.3%, while 10.7% and 26.8% achieved remission, respectively. The higher remission rate in cohort B should be viewed with caution as the reduction on CDAI scores from baseline was higher in cohort A (− 15.1) than in cohort B (− 12.2) and might be influenced by variations in baseline characteristics and treatment history between cohorts. In the RA-BE-REAL European analysis, results adjusted according to treatment history showed that treatment-naïve patients achieved an overall higher rate of LDA and remission in both cohorts [26], highlighting the importance of early treatment. These findings are consistent with those obtained from RCTs, where a similar proportion of patients treated with baricitinib achieved remission by the end of the third month [12,13,14,15,16]. It should also be noted that although remission is the therapeutic goal in early arthritis, for those patients with refractory disease, LDA is the recommended outcome according to international guidelines [7].
PhyGA and PtGA showed a noticeable decrease after 3 months in both cohorts, a trend that persisted for up to 24 months, pointing to an improvement in disease activity and overall health. Similarly, the HAQ-DI scores showed improvements, in line with the results from previous studies [13, 47]. In the RA-BEAM study, the improvements in PtGA and physical function were statistically significant compared to placebo in 1 week and these improvements were sustained over time, as were other PROs [13, 47].
Pain VAS scores showed a decrease in pain from 3 to 24 months post-treatment initiation. Pain alleviation was more notable and sustained in the cohort treated with baricitinib, whereas in patients treated with any other b/tsDMARD the effect was more pronounced after 6 months but less substantial after 24 months. These findings align with the European RA-BE-REAL study results, which demonstrated statistically significant pain reduction in patients treated with baricitinib [26]. Previous analysis of Spanish and Italian cohorts [25, 42] highlighted baricitinib’s efficacy in pain relief, underscoring its impact on improving HRQoL, as pain remains the most common symptom of RA and is often inadequately controlled [42, 48, 49]. Similarly, according to the results from the RA-BEAM study, patients treated with baricitinib experienced a significantly greater and more rapid pain relief through 24 weeks compared to placebo or adalimumab, regardless of whether they achieved disease control, and this effect was more marked as the pain relief thresholds increased [17, 50]. This evidence suggests that for patients with RA who have not responded adequately to MTX, baricitinib would be a more effective alternative for pain alleviation. In addition, the EQ-5D-5L index scores exhibited a numerical trend towards improvement after initiating baricitinib or other b/tsDMARD. This trend has been previously observed in other studies, independently of the history of previous treatments for RA [47, 51, 52]. The overall increasing percentage of patients reporting “no problems” in the five dimensions suggests a subtle but positive change in HRQoL. This trend is particularly visible for pain/discomfort, where a higher percentage of patients noted improvements. Taken together, these results point to a rapid improvement of PROs after treatment initiation, suggesting that patients quickly perceive pain relief and enhanced HRQoL even if they are treatment-experienced and were not obtaining positive results from other treatments.
A significant strength of our study lies in its contribution of valuable insights regarding the use of baricitinib across patient profiles typically excluded from RCTs, such as those with previous use of multiple b/tsDMARD treatments. Moreover, the multicentre design ensures an understanding of baricitinib usage patterns, effectiveness and persistence among patients with RA within Spanish routine clinical practice. However, we acknowledge that the analyses have some limitations that should be considered when interpreting the findings. The analyses were based on a small sample of patients, and this limits the possibility of conducting comparative analyses and detecting statistically significant differences between cohorts. The analyses were based on observed cases, with a sample size that decreased over time because of discontinuations. While providing valuable preliminary information, the analyses lack the statistical power required to draw conclusions or to generalize the findings to a broader population. Also, potential confounding variables were not controlled for. Moreover, there is a potential selection bias, as the patients were not randomized, and the treatment was prescribed at the discretion of physicians and patients as per clinical practice. Lastly, the safety profile of the treatments was not part of the study objectives, and only reasons for discontinuation related to safety were collected.
Future studies with larger sample sizes and longer follow-up periods are needed to address our study’s limitations. A larger population would allow for more robust comparisons and detailed subgroup analyses across diverse patient profiles, including different ages and prior treatments. Moreover, safety was only analysed through the discontinuation rates due to adverse events. Despite its limitations, this study offers valuable insights into baricitinib’s long-term real-world performance, aligning with the European BE-REAL study while providing specific information relevant to Spanish clinical practice. This can help clinicians optimize treatment strategies on the basis of their patients’ characteristics and the unique healthcare context in which they operate.

Comments (0)