1.
It is critical to diagnose axSpA using the ASAS criteria accurately. This is a cornerstone for implementing targeted therapeutic interventions and achieving optimal patient outcomes. Using these standardized criteria allows healthcare providers to distinguish axSpA from other rheumatological conditions and aids in early disease recognition, essential for preventing irreversible structural damage and preserving patients’ quality of life [10]. The ASAS criteria include two parallel yet complementary diagnostic approaches: the imaging arm and the clinical arm. The imaging arm mandates the presence of sacroiliitis, along with at least one feature of SpA. For the clinical diagnosis, HLA-B27 is required, along with at least two additional features of SpA. This dual-pathway approach ensures comprehensive patient evaluation while maintaining diagnostic accuracy. This step lays the foundation for effective management and treatment outcomes [54].
2.
AxSpA demands a comprehensive, multidisciplinary management approach that integrates various healthcare specialists to address its complex manifestations and optimize patient outcomes. This collaboration is fundamental to delivering care that addresses both the primary musculoskeletal symptoms and the diverse extra-articular manifestations of the disease [4]. Rheumatologists are the key professionals accountable for coordinating care, as they provide diagnostic expertise, treatment planning, and ongoing disease monitoring. Their specialized knowledge in inflammatory arthritis enables them to initiate and adjust appropriate pharmacological interventions, including csDMARDs and biological therapies when indicated. Additionally, physical therapists would provide strategies for managing daily activities and maintaining workplace productivity while protecting joint health. The multisystem nature of axSpA necessitates coordinated specialist care to address its various extra-articular manifestations. Ophthalmologists are crucial in monitoring and treating acute anterior uveitis, which affects almost one-third of patients with axSpA, requiring careful oversight to maintain vision. For gastrointestinal complications, gastroenterologists manage the concurrent IBD present in 5–10% of cases, ensuring treatments benefit both conditions. Similarly, dermatologists provide essential expertise in managing psoriasis and other cutaneous manifestations that occur in approximately 10% of patients, carefully balancing skin and joint treatments for optimal outcomes. This integrated specialist care approach helps ensure comprehensive disease management and improved patient outcomes [55, 56].
3.
A target-oriented treatment strategy for axSpA centers on systematically monitoring disease activity under rheumatologist supervision using validated composite scores every 3–6 months. For patients with steadily active disease in spite of conventional treatment, discussing treatment escalation with biological drugs is important, taking into account the patient’s clinical profile and access to therapy. This approach aims to achieve either remission or low disease activity state, thereby reducing the impact on function and quality of life. Regular assessment using validated measures enables healthcare providers to evaluate treatment responses objectively and make timely therapeutic adjustments through shared decision-making between patients and rheumatologists. This systematic monitoring helps identify the need for treatment modification early, potentially improving long-term outcomes while ensuring standardized documentation of disease activity parameters [57].
4.
Non-pharmacologic strategies play a vital role in managing axSpA. These interventions include physical therapy, which provides specific interventions that focus on spinal mobility, posture correction, and muscle strengthening. Professional physical therapists can develop individualized programs that address specific limitations and help patients maintain optimal joint function while preventing further mobility restrictions. Another strategy is to enhance patient education by providing comprehensive knowledge about their condition, including disease progression, lifestyle modifications, and self-management strategies. Understanding the disease flares and treatment options has a positive effect on the patients. Regular exercise is another effective intervention, particularly a combination of aerobic activities and flexibility training, that helps maintain spinal mobility, improves cardiovascular health, and reduces disease-related fatigue and stiffness. Finally, smoking cessation is crucial as tobacco use is associated with increased disease activity, more severe radiographic progression, and reduced treatment efficacy in patients with axSpA. These methods are effective in improving mobility, reducing discomfort, and enhancing overall well-being [27, 58].
5.
Patients’ engagement in shared decision-making about their treatment is crucial for achieving optimal health outcomes. By thoroughly explaining the available treatment options and taking patient preferences into account, healthcare providers can enhance treatment adherence and boost overall patient satisfaction [59]. Implementing shared decision-making requires improving physicians’ communication skills and educating patients about participation. Challenges for doctors include time constraints and the need for specific skills to establish partnerships with patients. However, involving patients in decision-making may not significantly increase consultation length. Self-management programs have been shown to reduce unplanned hospitalizations for various chronic conditions. Various approaches to support patient engagement include information leaflets, online peer support, counseling, and educational sessions [60].
These key recommendations for managing axSpA are summarized in Table 3. The final guideline statements and recommendations are presented in Table 4.
Table 3 Summary of the principles of management of axial spondyloarthritis (axSpA)Table 4 Strength and level of evidence for the recommendations for adults with active axial spondyloarthritis (axSpA)1. Diagnosis and Assessment of Adults with Active Axial Spondyloarthritis (axSpA)
Recommendation 1: We suggest using treat-to-target (T2T) management to measure disease activity in adults with an axSpA instead of using the usual care “a standard of care approach according to the treating rheumatologist of the patient” (conditional recommendation, low certainty of evidence).
Rationale
This recommendation was informed by a cluster-randomized, controlled, open-label trial (TICOSPA trial) (N = 160) comparing the advantages of a tight control/treat-to-target strategy (TC/T2T) versus usual care in patients with axSpA [61]. The proportion of patients achieving improvements of ≥ 20% (assessed by ASAS 20), ≥ 40% (assessed by ASAS 40), and ≥ 50% (assessed by Bath Ankylosing Spondylitis Disease Activity Index (BASDAI 50)) were non significantly greater in the T2T group in comparison with the usual care group (risk ratio [RR] 1.04, 95% confidence interval [CI] 0.81–1.34; low certainty; RR 1.35, 95% [CI] 0.83–2.21; low certainty; and RR 1.49, 95% CI 0.99–2.24; low certainty; respectively, Table S2). Additionally, there was no significant difference in the percentage of patients achieving Ankylosing Spondylitis Disease Activity Score – Low Disease Activity (ASDAS-LDA), ASDAS-Clinically Important Improvement (ASDAS-CII), and ASDAS-Major Improvement (ASDAS-MI) between the two groups (RR 1.12, 95% CI 0.79–1.60; low certainty; RR 1.33, 95% CI 0.86–2.06; low certainty; and RR 1.74, 95% CI 0.73–4.15; low certainty, respectively, Table S2). Regarding adverse events, the T2T group showed a non-significantly higher incidence in comparison with the usual care group (RR 1.35, 95% CI 0.85–2.16; low certainty, Table S2). Although this trial did not reveal a superiority of the T2T strategy compared to usual care, a greater percentage of patients in the T2T group achieved a ≥ 30% improvement on the ASAS-HI (47.3%) in comparison with the usual care group (36.1%) after 1 year. However, this difference was not statistically significant.
Therefore, the guideline panel deemed the intervention probably feasible, acceptable, and a large saving from a societal health economic perspective. In addition, they judged undesirable effects to be moderate. Other international guidelines align with our recommendation [27, 29].
Recommendation 2: We suggest using an ASDAS-C-reactive protein (ASDAS-CRP) to assess disease activity in adults with axSpA over standard care (a standard of care approach according to the treating rheumatologist of the patient) (conditional recommendation, very low certainty of evidence).
Rationale
This recommendation was based on a prospective observational study comparing the ASDAS versus the conventional clinical measures of disease activity in patients with axSpA treated with tumor necrosis factor
inhibitors (TNFis) (N = 60) [62]. The study indicated that after 22 weeks, the change was significantly higher using the change in ASDAS-CRP versus change in CRP as individualized marker (mean difference [MD] 0.79; very low certainty, Table S3), change in MRI SI joint inflammation (MD 0.46; very low certainty, Table S3), change in total inflammation (MD 0.34; very low certainty, Table S3), and change in the BASDAI (MD 0.76; very low certainty, Table S3) [62]. The study concluded that ASDAS is a valid and responsive measure of disease activity in patients with axSpA treated with TNFi, outperforming traditional measures like CRP and BASDAI [62].
The ASDAS has validated cutoff values for assessing disease activity, recognized by both the Outcome Measures in Rheumatology (OMERACT) and the ASAS [41, 63]. In 2016, the ASAS-EULAR recommendations for axSpA recognized ASDAS as the preferred method for evaluating disease activity, particularly in patients with high disease activity and those receiving bDMARDs [27]. Moreover, it was indicated that the established cutoffs for ASDAS-CRP are more aligned with clinical outcomes compared with ASDAS-ESR [64].
The guideline panel deemed the intervention to be probably acceptable and feasible. On the other hand, this recommendation is conditional and based on very low certainty of evidence, indicating the need for further research to strengthen these findings.
Recommendation 3: We recommend frequent monitoring every 3–6 months for adults with an axSpA, particularly when starting a new therapy, rather than less frequent monitoring every 12 months or more. The specific frequency should be tailored based on individual symptoms, severity, and treatment needs (strong recommendation, moderate certainty of evidence).
Rationale
Indirect evidence was used to address this recommendation because of the lack of direct evidence. A meta-analysis of 55 RCTs and cohort studies (N = 3976) evaluated the impact of TNFi on the spine and SI joint inflammation in patients with axSpA, as assessed by MRI at various follow-up intervals [65]. The disease activity after 12 weeks, as assessed by the SPARCC score in the spine and the SI joint, showed a reduction in the TNFi group in comparison with the placebo (MD − 4.85, 95% CI − 10.99 to 1.28 and MD − 3.19, 95% CI − 4.8 to − 1.58; moderate certainty; respectively, Table S4). When disease activity was evaluated by the ASspiMRI-a, the TNFi group demonstrated a greater reduction after 13 weeks compared to the control (MD − 1.67, 95% CI − 5.2 to 1.87; low certainty, Table S4). However, after 2 years of follow-up, the results favored the control (MD 1.34, 95% CI − 6.3 to 8.98; low certainty, Table S4).
The guideline panel determined that frequent monitoring is acceptable, likely cost-effective, feasible, and may enhance equity. Therefore, they strongly recommended frequent monitoring every 3 to 6 months. However, the exact frequency should be decided individually, depending on symptoms, severity, and treatment, which aligns with other international guidelines [29].
2. First-Line Treatment for Adults with Active Axial Spondyloarthritis (axSpA)
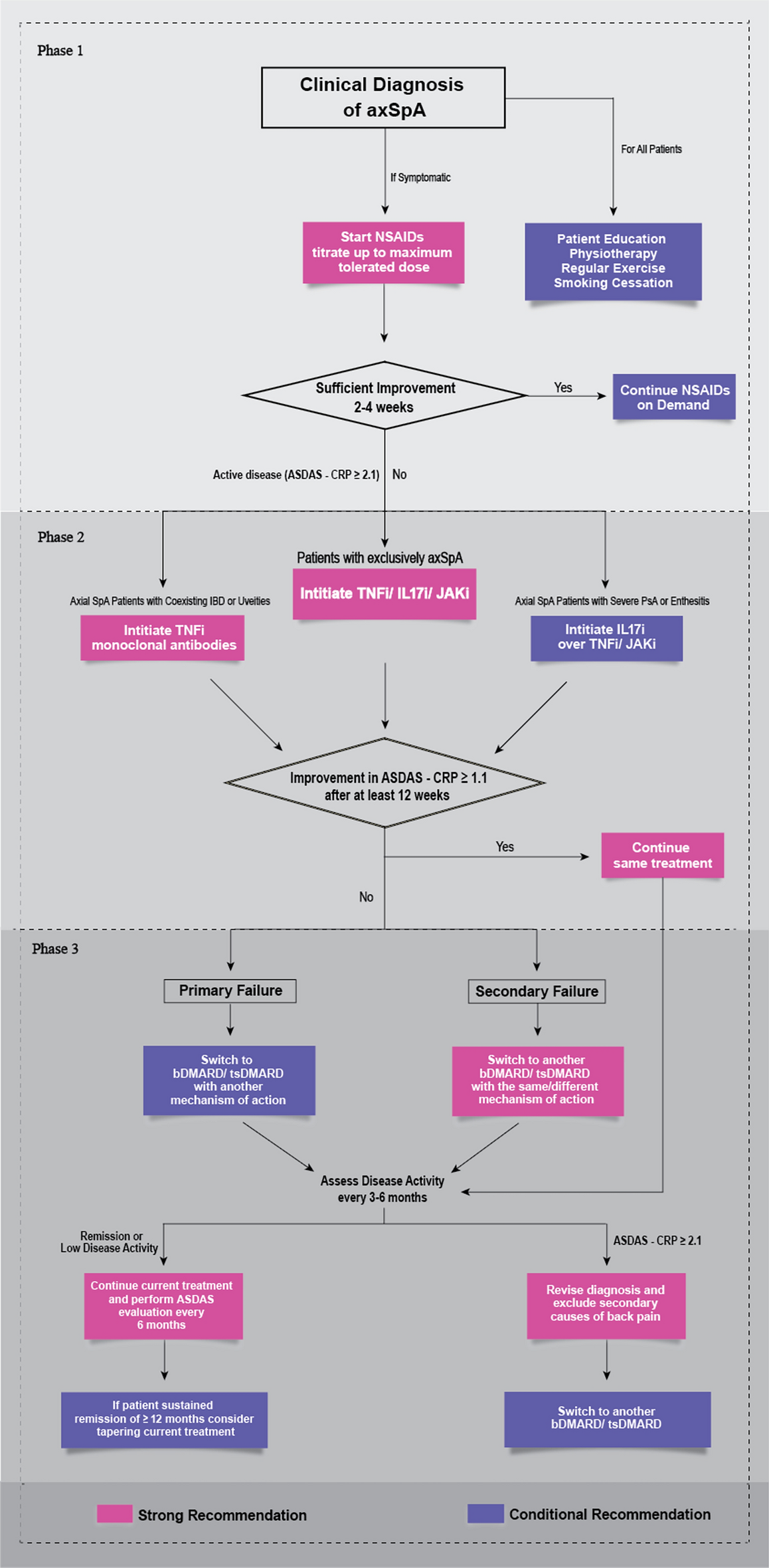
Recommendation 4: We recommend starting therapy with Nonsteroidal anti-Inflammatory drugs (NSAIDs) for symptomatic patients, using them as the primary treatment for 2 to 4 weeks (strong recommendation, moderate certainty evidence). Thereafter, we suggest on-demand use based on symptoms.
Remarks: For symptomatic adult patients with active axSpA, we suggest against continuous NSAIDs treatment. Continuous treatment may be associated with the risk of gastrointestinal bleeding, kidney injury, and cardiovascular disease.
Rationale
Our recommendation is based on an RCT study (N = 167) that aimed to compare the effect of continuous versus on-demand therapy with NSAIDs in patients with AS [66]. The continuous treatment group exhibited greater spinal radiographic progression (assessed by mSASSS) compared to the on-demand group (MD 0.49; moderate certainty, Table S5). However, this difference was not statistically significant. In patients with complete sets of radiographs, this difference was even more pronounced (MD 0.8; low certainty, Table S5) [66].
Furthermore, disease activity (assessed with BASDAI) was lower in the continuous versus the on-demand group during 2 years of treatment (MD − 0.5; low certainty, Table S5).
Regarding safety outcomes, total serious adverse events (SAE), SAE related to cardiovascular disorders, and SAE associated with IBD (colitis or Crohn’s disease) were not significantly different between both groups (RR 0.91, 95% CI 0.53–1.55; very low certainty; RR 0.33, 95% CI 0.04–3.12; moderate certainty; and RR 0.91, 95% CI 0.53–1.55; moderate certainty; respectively, Table S5).
On the contrary, an RCT by Wanders et al. concluded that continuous NSAIDs use reduced radiographic progression compared to on-demand use in symptomatic patients with AS [67]. However, SAEs were higher among subjects in the continuous-treatment group (19.8%) in comparison with those in the on-demand group (15.5%) [67].
The guideline panel suggests initiating treatment with NSAIDs for at least 4 weeks, followed by on-demand use for patients with persistent symptoms. NSAIDs were assessed as having negligible cost and savings, with a probable reduction in equity, and deemed likely feasible and acceptable. Once NSAIDs are started, periodic monitoring of disease activity and assessing the treatment response are essential. It is also important to consider the potential gastrointestinal, renal, cardiovascular, and other risks associated with NSAIDs use.
Recommendation 5: For adults with active axSpA requiring non-steroidal anti-inflammatory treatment, we suggest using either standard NSAIDs or COX-2 inhibitors (conditional recommendation, very low certainty evidence).
Remarks: COX-2 inhibitors may be preferred for patients with a history of gastrointestinal complications or IBD, as they are associated with a lower risk of gastrointestinal side effects compared to regular NSAIDs.
Rationale
This recommendation is informed by a network meta-analysis of RCTs (N = 3647) comparing different NSAIDs in the treatment of AS; no significant differences were found in the main findings between diclofenac and two other commonly used NSAIDs, celecoxib and etoricoxib [68].
Regarding the functional ability, diclofenac showed no significant difference compared to celecoxib (MD − 0.47, 95% CI − 3.65 to 2.31; low certainty, Table S6) or etoricoxib (MD 5.29, 95% CI − 2.21 to 12.3; very low certainty, Table S6) [68]. Similarly, pain scores showed non-significant differences: diclofenac had a slightly lower, but non-significant, effect in comparison with celecoxib (MD − 1.66, 95% CI − 6.34 to 3.03; low certainty, Table S6) and a slightly greater, though still non-significant, effect compared to etoricoxib (MD 6.67, 95% CI − 2.2 to 16.13; low certainty, Table S6) [68].
In terms of disease activity, as assessed by the patient’s global assessment of disease activity, and treatment response, assessed with ASAS 20, diclofenac again showed no significant difference compared to celecoxib (MD − 1.56, 95% CI − 6.76 to 3.8; low certainty; odds ratio [OR] 1.16, 95% CI 0.77–1.55; respectively, Table S6) or etoricoxib (MD 7.93, 95% CI − 1.74 to 17.43; very low certainty; MD 0.42, 95% CI 0.16–1.08; low certainty; respectively, Table S6) [68].
For total adverse events, the diclofenac group had a higher non-significant incidence compared to celecoxib (OR 1.14, 95% CI 0.65–1.89; low certainty, Table S6) and etoricoxib (OR 1.29, 95% CI 0.48–3.59; low certainty, Table S6). Similarly, gastrointestinal adverse events were observed more repeatedly, but not significantly, in the diclofenac arm in comparison with celecoxib (OR 1.68, 95% CI 0.86–3.13; low certainty, Table S6) and etoricoxib (OR 1.11, 95% CI 0.31–4.06; low certainty, Table S6).
A systematic review assessed the safety of COX-2 inhibitors used for treating rheumatological manifestations of IBD and found no significant difference in the exacerbation of IBD between the COX-2 inhibitors and placebo. After 12 weeks of treatment, the exacerbation rate in the COX-2 inhibitors arm was lower than the placebo (17% vs. 19%, respectively) (RR 0.88, 95% CI 0.45–1.69) [69]. Another study found that 14-day treatment with celecoxib shows no higher relapse rate among patients with ulcerative colitis who had a present or previous history of arthralgia, nonspecific arthritis, or other diseases amenable to NSAIDs treatment [70]. In addition, several studies reported that NSAIDs use was associated with IBD onset or clinical exacerbation [72,73,73].
The guideline panel suggested using both COX-2 inhibitors (celecoxib, etoricoxib) and NSAIDs for patients with active axSpA. However, they emphasized the importance of regularly monitoring disease activity and adverse events, beside assessing the degree of response. Special consideration should be given to these medications’ potential gastrointestinal, renal, and cardiovascular effects.
3. Second-Line Treatments for Adults with axSpA
Recommendation 6: For adults with active axSpA, we recommend using either TNFi (including infliximab, etanercept, certolizumab, adalimumab, and golimumab), interleukin-17 inhibitors
(IL-17is) (ixekizumab, secukinumab, and bimekizumab), or Janus kinase inhibitors (JAKis) (upadacitinib and tofacitinib) (strong recommendation, moderate evidence).
Rationale
The guideline panel recommended either TNFi therapy, IL-17i, or (JAKi) for adults with active axSpA, acknowledging their efficacy. However, they advised against using JAKi in patients with a history of thrombosis or those at high risk for cardiovascular disease. This recommendation was informed by a large network meta-analysis (N = 8937) comparing treatment options for AS [74]. TNFi showed better health status outcomes than JAKi when assessed by ASAS 20 (RR 0.77, 95% CI 0.60–0.99; very low certainty, Table S7), but results were not significant for ASAS 40 or ASAS 5/6 (RR 0.76, 95% CI 0.47–1.19; very low certainty; OR 0.66, 95% CI 0.33–1.26; very low certainty; respectively, Table S7) [74].
An RCT involving 270 patients across 75 centers in 14 countries assessed the efficacy of tofacitinib 5 mg twice daily compared to placebo [75]. Significant improvements were noted in ASAS 20 (RR 1.92, 95% CI 1.42–2.59; moderate certainty, Table S8) and ASAS 40 (RR 3.25, 95% CI 1.99–5.30; moderate certainty, Table S8). Disease activity, assessed by ASDAS, showed a mean improvement of 0.97 (95% CI − 1.164 to − 0.776; high certainty, Table S8), while high-sensitivity C-reactive protein (hsCRP) levels decreased by 0.96 (95% CI − 1.24 to − 0.68; high certainty, Table S8) [75]. Moreover, the tofacitinib group had a greater frequency of partial remission (RR 5.11, 95% CI 1.80–14.56; high certainty, Table S8) and ASAS 5/6 response (RR 5.93, 95% CI 3.17–11.10; high certainty, Table S8). Adverse events were described in 54.9% of the tofacitinib group and 51.5% of the placebo group, with SAE in 1.5% and 0.7%, respectively [75].
On the basis of this evidence, JAKi has demonstrated significant efficacy in decreasing disease activity and symptoms while maintaining favorable safety outcomes, making it a valuable treatment option for axSpA, consistent with other guidelines. However, concerns remain regarding the potential risks of venous thromboembolism and cardiovascular events, particularly in patients with high cardiovascular risk factors or those on long-term JAKi therapy [27, 29].
A cohort study also found similar drug discontinuation rates and 1-year responses between JAKi and TNFi in patients with rheumatoid arthritis (RA) [76]. The guideline panel acknowledged the efficacy of JAKi (e.g., upadacitinib, tofacitinib) for active axSpA but highlighted their high cost. They emphasized the importance of regular monitoring for disease activity (e.g., ASDAS) and adverse events, as well as screening for cardiovascular complications, malignancy, and thrombosis before initiating JAKi. Additionally, other international guidelines recommend avoiding JAKi in patients over 65 or those with high cardiovascular risk [27]. Research priorities include head-to-head trials comparing TNFi and JAKi, as well as long-term remission, safety, and economic evaluations.
The panel also suggested IL-17A inhibitors (e.g., secukinumab, ixekizumab) or IL-17A/F inhibitors (e.g., bimekizumab) for adults with active axSpA.
A network meta-analysis compared bimekizumab’s efficacy and safety to other bDMARDs. For ASAS 20 improvement, bimekizumab showed non-significant advantages over ixekizumab (OR 1.01, 95% CI 0.61–1.61; low certainty, Table S9) and secukinumab (OR 1.24, 95% CI 0.86–1.79; low certainty, Table S9). For ASAS 40 improvement, bimekizumab had non-significantly lower odds compared to ixekizumab (OR 0.92, 95% CI 0.57–1.44; low certainty, Table S9) but significantly higher odds compared to secukinumab (OR 1.6, 95% CI 1.01–2.6; low certainty, Table S9). Bimekizumab also showed better partial remission outcomes compared to secukinumab (OR 1.65, 95% CI 1.08–2.51; low certainty, Table S9) [77].
Phase 2 and 3 RCTs have demonstrated that bimekizumab provides rapid and sustained improvement in SpA outcomes without significant adverse events [78, 79].
This evidence highlights the effectiveness of bimekizumab with significant improvements compared to placebo as observed in a ≥ 20% improvement in health status measured by ASAS 20 (OR 3.22, 95% CI 2.3–4.35, moderate certainty, Table S10), 40% improvement measured by ASAS 40 (OR 4.02, 95% CI 3.08–5.19, moderate certainty, Table S10), and partial remission assessed by ASAS-PR (OR 5.02, 95% CI 3.62–6.84, moderate certainty, Table S10) [77].
A recent RCT randomized subjects with active psoriatic arthritis and previous inadequate response or intolerance to TNFi to receive either bimekizumab 160 mg every 4 weeks or placebo. By week 16, 43% of those on bimekizumab reached the American College of Rheumatology 50% Improvement (ACR50), in comparison with 7% in the placebo (adjusted OR 11.1, P < 0.0001). Among patients with at least 3% body surface area affected by psoriasis, 69% on bimekizumab achieved Psoriasis Area and Severity Index 90 (PASI 90), versus 7% on placebo (adjusted OR 30.2, P < 0.0001). Treatment-emergent adverse events (TEAEs) were reported in 40% of the bimekizumab group and 33% of the placebo, with no new safety concerns or deaths [80].
While the panel recognized the high cost of IL-17i and their potential to reduce equity, they concluded that bimekizumab is acceptable, feasible, and likely to improve health equity. Larger studies are warranted to provide clearer evidence for effectiveness and safety.
The panel suggested either TNFi therapy, IL-17i, or JAKi for adults with active axSpA, based on their established effectiveness and safety. The decision should be guided by the safety profile, coexisting comorbidities, extra-musculoskeletal manifestations, patient preference, risk–benefit ratio, and cost considerations.
The strong recommendation for TNFi, JAKi, or IL-17i was supported by high-quality evidence from multiple RCTs demonstrating the efficacy of each drug class compared with the placebo and considering that the overall benefits of them outweigh the potential risks [82,83,84,85,86,86]. However, the low certainty evidence originated from the cited network meta-analyses, which compared the efficacy of TNFi with JAKi and IL-17i (secukinumab, ixekizumab) with bimekizumab alone, in the absence of direct head-to-head comparisons, to answer the relevant PICO questions.
Recommendation 7: For adults with active axSpA, we suggest using any TNFis (conditional recommendation, low evidence).
Rationale
Our recommendation is based on a recent meta-analysis, including 48 articles comparing the different treatment options in patients with AS. The study indicated that TNFi had consistent and significant benefits across multiple clinical outcomes compared to placebo. A significant improvement in disease activity was observed in ASAS 20 (RR 2.2, 95% CI 2.0–2.5; low certainty, Table S11), ASAS 40 (RR 3.1, 95% CI 2.4–4.2; low certainty, Table S11), ASAS 5/6 (RR 5.4, 95% CI 3.9–7.7; low certainty, Table S11), and BASDAI 50 (RR 3.2, 95% CI 2.6–4.0; low certainty, Table S11). In addition, TNFi treatment resulted in an MD of − 1.4 (95% CI − 1.6 to − 1.2; low certainty, Table S11) in BASFI. However, a slight risk of adverse events among patients treated with TNFi was detected (RR 1.2, 95% CI 1.1–1.3; low certainty, Table S11) [74].
However, in previous studies, etanercept did not demonstrate clear efficacy in treating uveitis and has been linked with a high risk of uveitis flares [87]. When comparing the efficacy of anti-TNFα antibodies such as adalimumab and infliximab with a soluble TNF receptor molecule such as etanercept in patients with AS, etanercept treatment triggered new-onset uveitis cases more than adalimumab after a short-term period (26.4% vs. 6.3%; P = 0.024) [88]. In addition, another study found that patients with AS who received monoclonal TNFi reported infrequent new onset and flare of IBD events, as well as infliximab largely prevented IBD activity. In comparison, those who received etanercept reported a high frequency of new-onset and flares of IBD [89]. Thus, the panel suggests using monoclonal TNFi and avoiding etanercept for cases with concomitant uveitis or IBD.
The guideline panel issued a conditional recommendation, noting that head-to-head trials comparing

Comments (0)