In this large, real-world retrospective cohort study of patients with SLE initiating belimumab, we used IPTW to create similar cohorts of patients with or without prior IS use and address potential confounding. We found that prescribing belimumab as part of standard treatment, without prior use of IS, was associated with earlier and higher rates of OGC discontinuation as well as fewer SLE flares, compared with patients initiating belimumab after IS therapy. The odds of all-cause emergency department visits were higher among patients without prior IS use compared with those with prior IS use in the 12 months following belimumab initiation, but there were no differences in SLE-related HCRU.
The 2023 EULAR recommendations for the management of SLE emphasise the need for rapid OGC tapering (≤ 5 mg/day prednisone-equivalent) and discontinuation to aid the prevention of organ damage and other OGC-related adverse events linked to cumulative use, such as increased risk of infections and mortality [10, 11, 28]. These recommendations further highlight that prior treatment failure with conventional IS should not be mandatory to initiate treatment with biologics, such as belimumab, in patients not responding to hydroxychloroquine treatment (with or without glucocorticoid use) [5].
Here we demonstrated that patients who initiated belimumab without IS use in their SLE treatment sequence discontinued OGC therapy approximately 2 months earlier than patients who initiated belimumab following prior use of IS. The non-IS cohort also had a 30% higher rate of OGC discontinuation immediately after initiating belimumab relative to the IS cohort, though this effect attenuated over time. While no significant difference in OGC dose reduction to the recommended dose of < 5 mg/day for patients on ≥ 10 mg/day was observed in this study, findings of this study largely align with a previous report, showing that belimumab initiation without prior IS use was also associated with earlier OGC discontinuation and/or dose reduction to < 5 mg/day [21]. Considering the dose-dependent toxicity and adverse events associated with long-term steroid use [10], withdrawing OGC sooner implies greater health benefits for patients [29, 30], such as reduced risk of organ damage, infections and mortality [11, 28]. Taken together, these OGC findings suggest that initiation of belimumab in patients who have not received IS therapy may help achieve EULAR’s recommendations to taper or discontinue OGC therapy and reduce OGC-related adverse events associated with long-term use.
Earlier OGC withdrawal also signifies greater control of patients’ symptoms owing to the reduced need for OGC use. In line with this, we found that patients initiating belimumab without prior IS use had lower overall rates of SLE flares. Interestingly, we observed a reduction in moderate flares and an increase in mild flares, indicating that flares experienced by patients in the non-IS cohort were of a lower magnitude, lending support to the hypothesis that use of belimumab as standard treatment could help achieve better disease control than conventional IS by either preventing a flare or reducing the severity of a flare. These findings align with similar observational studies that assessed non-claims data sources with other clinical measures available, including disease activity and risk of new organ damage [20, 21], as well as with preliminary findings from a cohort of patients with early SLE, where those who had not received IS prior to belimumab treatment also experienced fewer flares than patients who had received prior IS [31]. Of note, our previous descriptive study reported lower rates for flares of all severities for the cohort initiating belimumab without prior use of IS [21]. However, our previous study did not account for variation in patient baseline characteristics, and the baseline period was anchored on 24 months prior to belimumab initiation rather than the 12 months prior to the initial clinical decision to start IS [21]. By contrast, the current study used more rigorous IPTW to account for baseline characteristics measured in the 12 months prior to initiation of non-IS/IS treatment, although it should be noted that IPTW excluded race and ethnicity, and clinical biomarkers because of lack of data in the Komodo dataset, which may have contributed to residual confounding. Furthermore, it is crucial to recognize that the definition of SLE flare used in this study may not fully reflect clinical reality. Flares were classified using a claims algorithm based on specific medications, prescription fills, types of hospital admissions, and associated diagnoses, and it varied substantially from flare definitions used in clinical trials, and from what is perceived as a flare in the clinic. In short, published clinical studies frequently rely on the Safety of Estrogen in Lupus Erythematosus National Assessment—Systemic Lupus Erythematosus Disease Activity Index (SELENA-SLEDAI) Flare Index (SFI) flare [32], while clinicians generally perceive a “flare” as relapse following treatment response. Nevertheless, the flare algorithm utilized in this study [25] has been validated to recognize SLE severity (mild, moderate and severe) when SLEDAI is not available [33], and has been successfully incorporated into a number of published studies utilizing various databases for research [34,35,36].
A previous HCRU analysis of belimumab initiation prior to IS use focused on all-cause HCRU by SLE severity [21], finding all cause-HCRU to be generally similar across cohorts, irrespective of disease severity or IS treatment prior to belimumab [21]. The present study conducted separate analyses of all-cause HCRU and those in relation specifically to SLE. We found increased likelihood of all-cause emergency department visits in the non-IS versus IS cohort, but similar likelihood of SLE-related emergency department visits and all-cause and SLE-related inpatient stays between both cohorts. Further studies are required to understand the emergency department visit result in relation to all causes, particularly the relationship between pre-existing comorbidities and HCRU. In the current study, follow-up time was not considered in the HCRU analysis, but was included in the model for flares. Therefore, a future analysis of HCRU, which incorporates the timing of emergency visits and inpatient stays, may demonstrate a similar benefit for those using belimumab without prior IS to those with prior IS use. Additionally, a more in-depth assessment should consider the specific diagnosis codes associated with emergency department visits to improve our understanding of HCRU in relation to belimumab and IS use.
There are many possible drivers for the positive outcomes of this real-world study, including more rapid tapering of OGC and reduced rates of SLE flares in patients without IS use prior to starting belimumab matched using IPTW to a cohort of prior IS users. One potential driver is the tolerability and more targeted immunosuppression of belimumab [19, 37,38,39], resulting in reduced disease activity and OGC use [40, 41]. Although the efficacy and safety of belimumab have been extensively studied, further investigation of treatment sequence and optimal timing of biologics, particularly in patients with new onset SLE randomised to initial treatment with belimumab or an alternative therapeutic regimen, is required. Indeed, belimumab efficacy and safety in patients with early SLE with/without prior IS use will be investigated in an ongoing clinical trial (BeEARLY, GSK Study 219240, NCT06411249), enabling analysis of belimumab’s impact on relevant disease activity endpoints [42, 43].
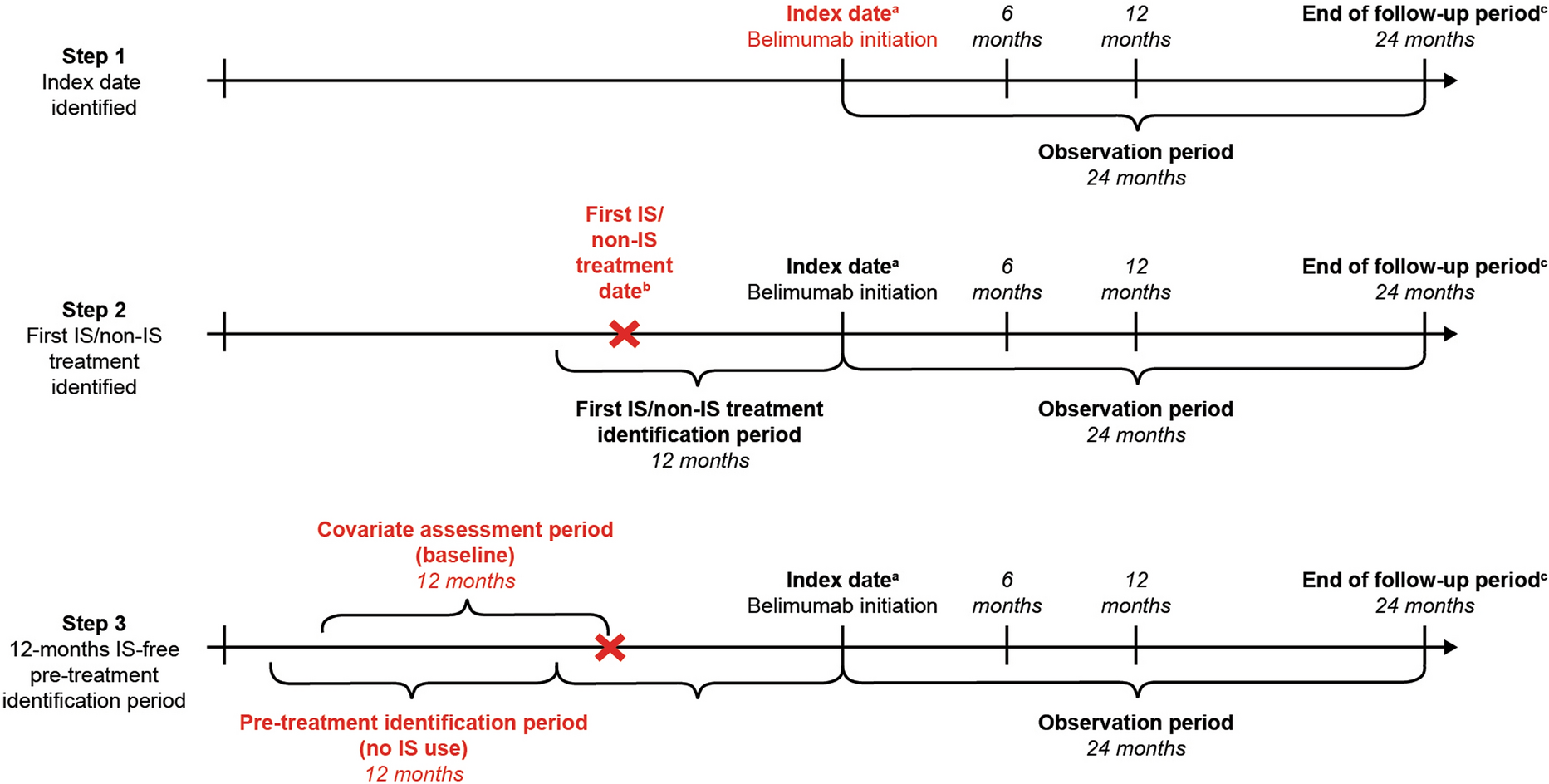
One of the strengths of the current real-world study lies in the large population that was well balanced between cohorts. The patient sample was obtained from a national, multi-payer, USA-based claims database, which offers extensive geographic and demographic representation and can be expected to be reflective of many patients in clinical practice. Although the study imposed certain eligibility criteria, the findings described here are generally applicable to the US adult population with SLE treated with belimumab. Furthermore, the rigorous study design led to more conservative results than those presented in our previous study [21]. First, application of IPTW (which included a range of patients’ demographic and clinical characteristics) and doubly robust estimation reduced confounding bias. Second, anchoring of the covariate assessment period at the start of IS/non-IS treatment prior to belimumab, rather than at belimumab initiation, ensured that the captured covariates allowed adjustment for channelling bias by capturing covariates that would have been considered by the clinicians when deciding the appropriate treatment. As such, the covariate assessment period was reflective of the clinicians’ decision-making period (e.g. deciding whether to prescribe IS or belimumab), which was an essential part of the study design that allowed the assessment of the treatment pathway. Lastly, non-belimumab biologics were included to ensure that all non-belimumab treatments were considered; however, only a small proportion of patients in the non-IS cohort received them.
Certain limitations to this study should be considered when interpreting the findings. Claims data used in this study lack information on clinical biomarkers and disease activity (e.g. for calculation of SELENA-SLEDAI) [44], as these measures are not routinely assessed by physicians in standard clinical practice and, consequently, administrative claims. This may have introduced some bias through measurement error when using claims-based proxies for SLE flares and disease severity, but the presence of a comparator cohort reduced the magnitude of the bias as both cohorts would have been impacted to a similar extent. Data on drug use, medical records and HCRU were limited to those provided through claims only; as such, the actual numbers may not be fully reflected, particularly for patients who may have had co-insurance or supplemental insurance coverage. Together with non-claims drug use or treatment non-adherence, those may have potentially contributed to data missingness or misclassification. It should also be noted that although OGC dose alone was not included in cohort weighting, it is a component of SLE severity and flares, which were both included in IPTW. Patients discontinuing belimumab or initiating alternative treatment during the observation period were not censored. As the average time on belimumab was approximately 11 months, follow-up data beyond 24 months was excluded from this study as it may have been attributable to factors other than belimumab. Lastly, potential residual confounding from unobservable and unmeasured characteristics, such as race, ethnicity or clinical biomarkers (e.g. SELENA-SLEDAI), could have influenced treatment decisions and although the study design incorporated IPTW and doubly robust statistical estimators to ensure both cohorts had comparable characteristics anchored on the baseline period, some confounding may still be present.

Comments (0)