Study Design and Participants
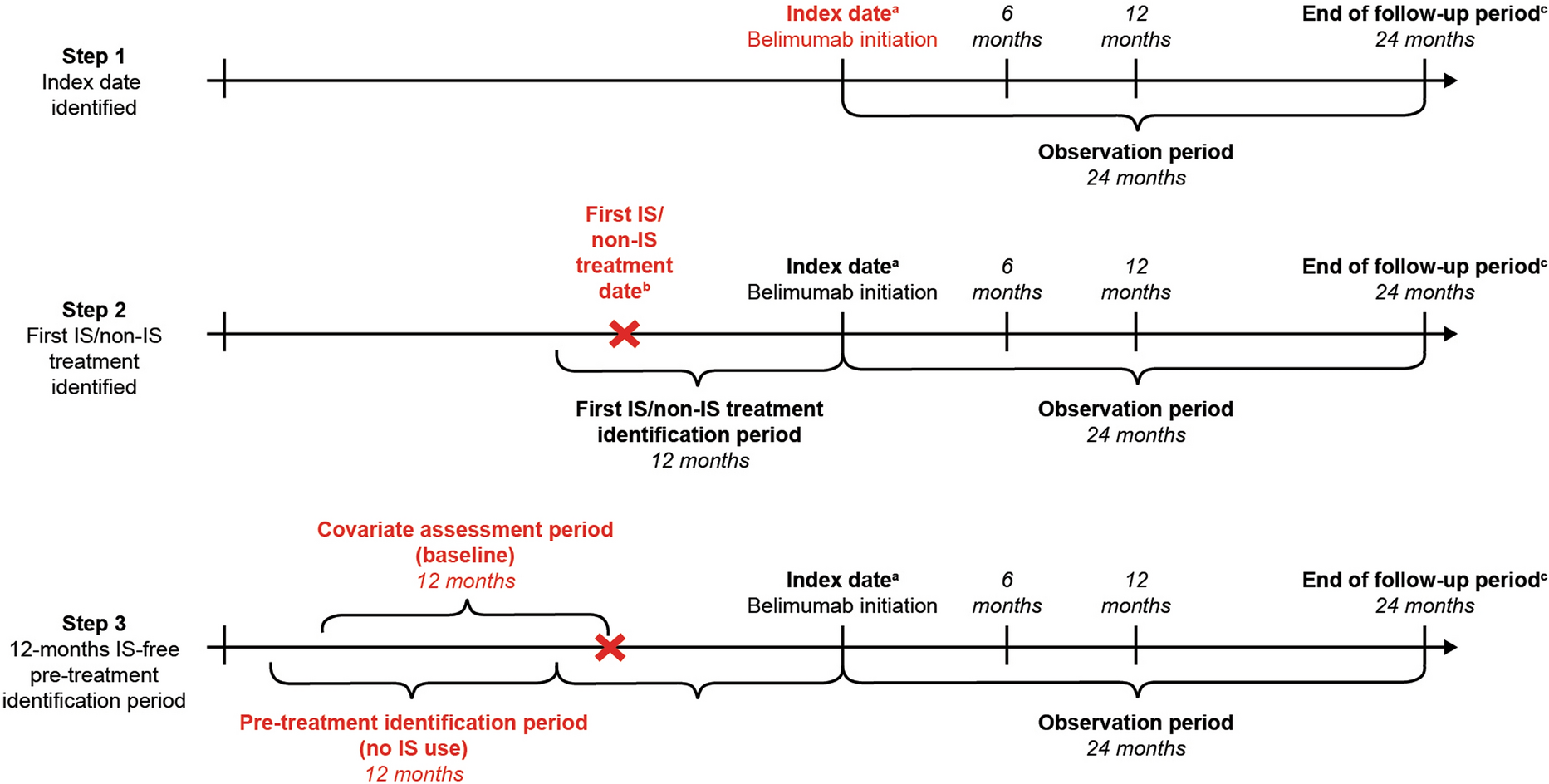
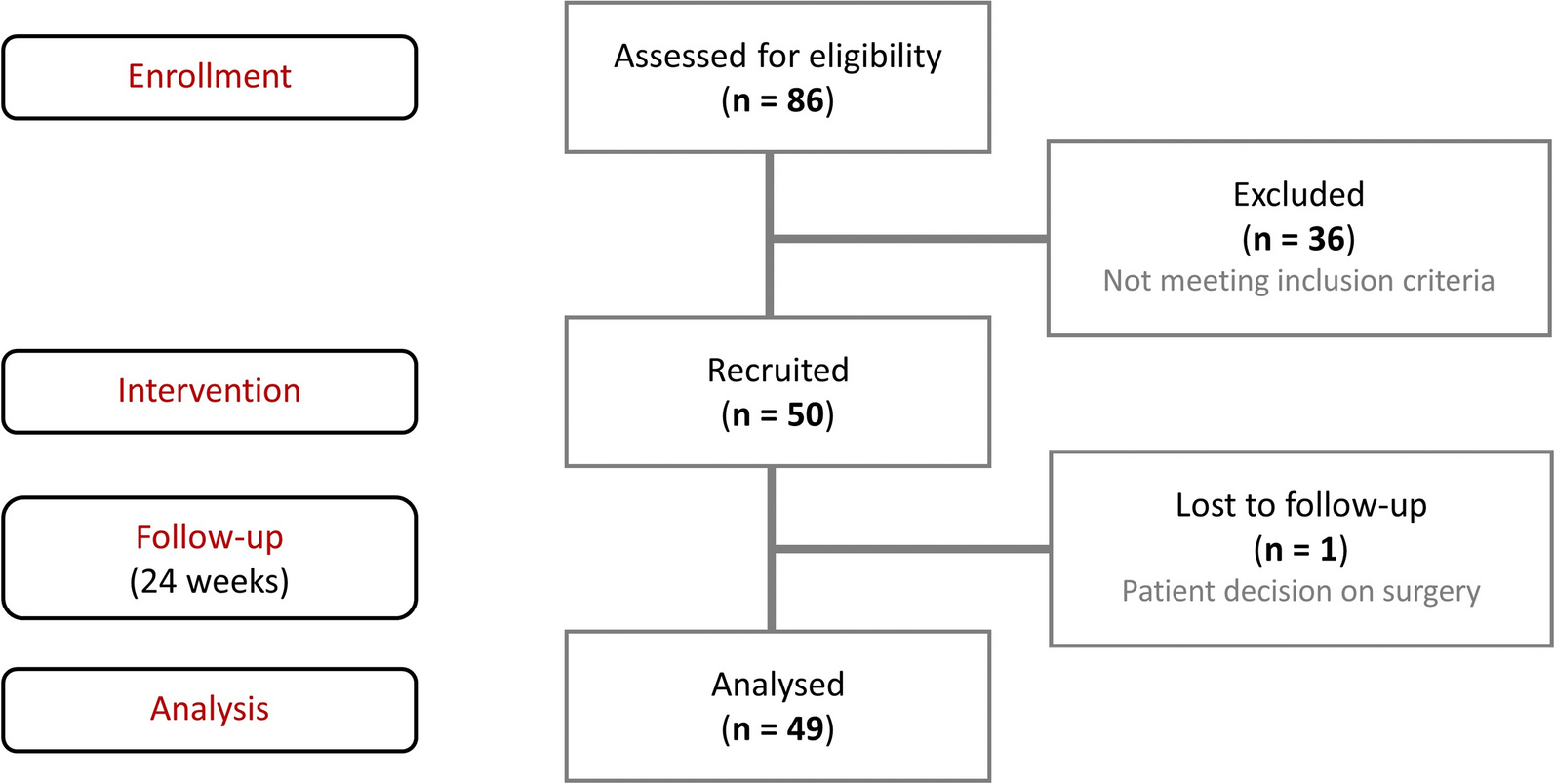
This retrospective, observational cohort study used administrative claims data, collected between January 1, 2009 and December 31, 2020, from the Merative™ MarketScan® databases, to identify patients newly diagnosed with GCA initiating glucocorticoid treatment and assess their glucocorticoid use for ≥ 1 year and up to 5 years (Supplementary Fig. S1). For patients newly diagnosed with GCA and initiating glucocorticoids (GCA + GC cohort), eligible patients were aged ≥ 50 years, had continuous enrollment with medical and pharmacy benefits for ≥ 12 month pre- and post-index date, and had ≥ 1 inpatient or ≥ 2 outpatient claims (≥ 7 days and ≤ 365 days apart) with a diagnosis code indicating GCA (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM]: 446.5; ICD-10-CM: M31.6 [GCA without concomitant polymyalgia rheumatica], M31.5 [GCA with polymyalgia rheumatica]) between January 1, 2010 and December 31, 2019. The GCA index date was the date of the earliest GCA claim. Patients with any evidence of a GCA diagnosis in the 12 months prior to index date were excluded to create an inception cohort of new-onset GCA.
Among patients with newly diagnosed GCA, those newly initiating oral glucocorticoids were identified on the basis of outpatient pharmacy claims for oral glucocorticoid treatment up to 90 days prior to and 1 year after the GCA index date. Parenteral administration of glucocorticoids was not accounted for because of inability to identify dosing. Eligible oral glucocorticoids included betamethasone, cortisone, dexamethasone, fludrocortisone, hydrocortisone, methylprednisolone, prednisolone, prednisone, triamcinolone, and deflazacort. To be included in the GCA + GC cohort, patients had to have at least 12 months’ continuous enrollment after glucocorticoid initiation and had received ≥ 30 days’, but ≤ 360 days’, supply during the 12-month post-index period. Glucocorticoid index date was defined as the date of the earliest claim for a glucocorticoid prescription. The ≤ 360 days’ supply was based on typical quantities of glucocorticoid prescribed (i.e., 30 or 90 days’ supply). Additionally, to ensure appropriate patient selection, glucocorticoid initiation was allowed up to 90 days prior to GCA index date, as it is possible that patients initiated glucocorticoid treatment while undergoing clinical evaluations to confirm GCA diagnosis; however, to be included, patients had to have a claim with a GCA-related symptom reported (Supplementary Table S1). Patients were excluded if they had oral glucocorticoid use in the 12-month pre-index period (without a GCA-related symptom) or a prescription for > 80 mg/day (prednisone equivalent dose), as this may indicate use not related to GCA.
The above eligibility criteria were based on a modified version of the patient identification algorithm published by Lee et al. [23]. Modifications included the allowance of non-rheumatology specialties, such as internal medicine or ophthalmology, and use of a time-bound steroid initiation rather than only restricting high doses of glucocorticoids to allow for variations in medical practice and patient preference. This modified approach enabled identification of patients commensurate with the primary objective of this research to characterize patients with GCA in a real-world practice context.
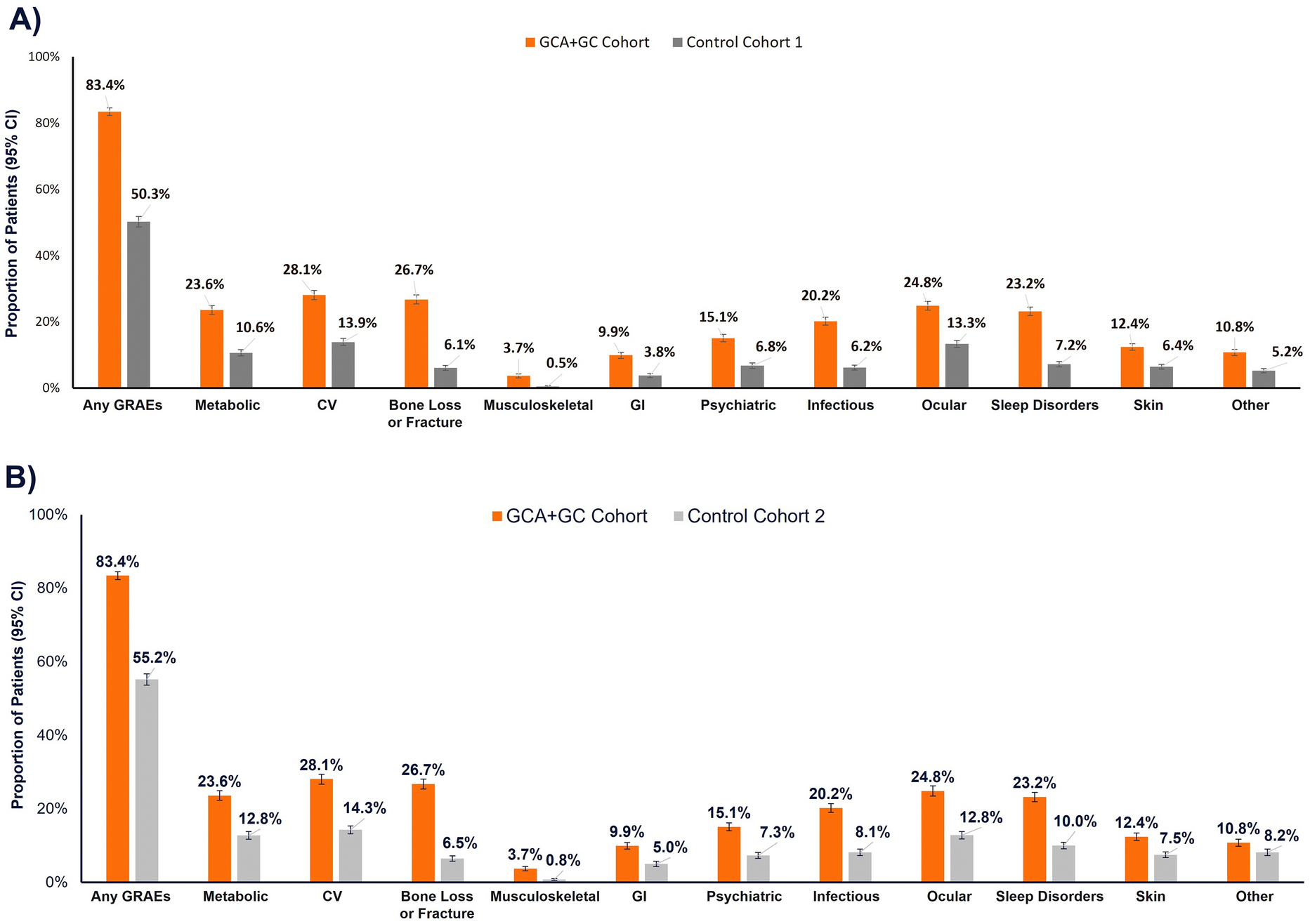
For comparison, two control cohorts were established (control cohort 1 [CC1] and control cohort 2 [CC2]), with patients aged ≥ 50 years, with ≥ 12 months continuous plan enrollment pre- and post-index date, and no evidence of a GCA diagnosis between January 1, 2009 and December 31, 2020. For CC1, patients had to have no evidence of glucocorticoid use before or after the index date. This cohort allowed ascertainment of background rates of GRAEs among a similarly aged sex- and comorbidity-matched population such that, when compared to the GCA + GC cohort, the glucocorticoid burden in incident GCA cases could be assessed independent of other potential causes (e.g., due to advanced age). For CC2, patients were randomly selected from a 5% sample of the entire database population. Selected individuals could have oral glucocorticoid use before or after the start of follow-up, allowing for comparison to a relevant elderly control population that may be receiving glucocorticoids for reasons other than GCA.
For the control populations, corresponding index dates between January 1, 2010 and December 31, 2020 were randomly assigned using a uniform distribution. Patients in the GCA + GC cohort were matched 1:1 with patients in both control groups using propensity score matching.
This analysis used a de-identified administrative claims database and thus did not require institutional review board approval nor patient consent.
Outcomes
Demographic and clinical characteristics are reported for the propensity score matched cohorts. Average daily glucocorticoid dose and cumulative glucocorticoid exposures up to 5 years were reported for the GCA + GC cohort. Assessment of GC burden was considered across a framework of 39 conditions, stratified across 11 categories (Table 1). Chronic conditions were required to be newly incident following glucocorticoid initiation (or index date for controls); if patients had a claim for a chronic condition in the 12 months prior to index date, they were not eligible post analysis for that condition but could be eligible for other conditions. All patients were eligible for the occurrence reporting of acute events. Occurrence of GRAEs was measured at baseline and is categorized by mean daily dose for over 12, 24, 36, and 60 months. Glucocorticoid dose was categorized by > 0 to ≤ 7.5 mg (“low”), > 7.5 to ≤ 20 mg (“medium”), > 20 mg to ≤ 40 mg (“high”), and > 40 mg (“very high”). Healthcare utilization, including inpatient admission, emergency department (ED) visits, and outpatient visits, services, and pharmacy prescriptions were assessed, with outcomes including proportion of patients utilizing each service, frequency of utilization, and healthcare costs (all-cause, GCA-related, and GRAE-related).
Table 1 GRAEs by categoryStatistical Analysis
Continuous measures are presented as means with standard deviations (SDs) and categorical measures are reported as counts and percentages. Propensity scores were generated using logistic regression and included age, sex, Deyo-Charlson Comorbidity Index (DCI) score, and index year. The matching algorithm used greedy nearest neighbor matching with a caliper width of 0.2 of the standard deviation (SD) of the logit of the propensity score. Distribution of propensity scores for the two cohorts was compared to determine sufficient overlap and balance. Balance of patient characteristics was compared using standardized mean difference (SMD); characteristics were considered balanced if the SMD was < 0.1.
The average daily glucocorticoid dose during the period from month 1 up to month 60 for each patient was calculated by dividing total steroid dose (in prednisone equivalents) by total number of days and was calculated among patients who filled at least one glucocorticoid pharmacy claim. Stockpiling was applied, meaning the start date of a new glucocorticoid pharmacy claim was adjusted to the day after the expiration date of the previous glucocorticoid claim if it was filled before the prior claim’s expiration date. Prescriptions that had their days’ supply extend beyond the date of censoring or the end of follow-up were truncated to assess exposure within the defined time periods.
Data were collected from inpatient medical, outpatient medical, and outpatient pharmaceutical claims data using enrollment records, service dates, ICD-9/10-CM codes, Healthcare Common Procedure Coding System codes, and/or National Drug Codes (Supplementary Table S2).
Healthcare costs were adjusted for inflation to 2020 US dollars (USD) using the Medical Care component of the Consumer Price Index and included gross covered payments for all healthcare services or products. GCA-related costs were classified as any costs associated with claims with a GCA diagnosis. Costs related to GCA and GRAEs were determined on the basis of diagnosis codes identified in claims.
Odds ratios (OR) were determined by logistic regression for each GRAE category as dependent variables, adjusted for age, sex, US region, index year, DCI score, insurance type, and baseline prevalent GRAE event (presence of any event within the same category during pre-index period, given the potential increased risk for another within-category event in post-index period [e.g., prediabetes in pre-index period, type 2 diabetes in post-index period]).

Comments (0)