
Remember me
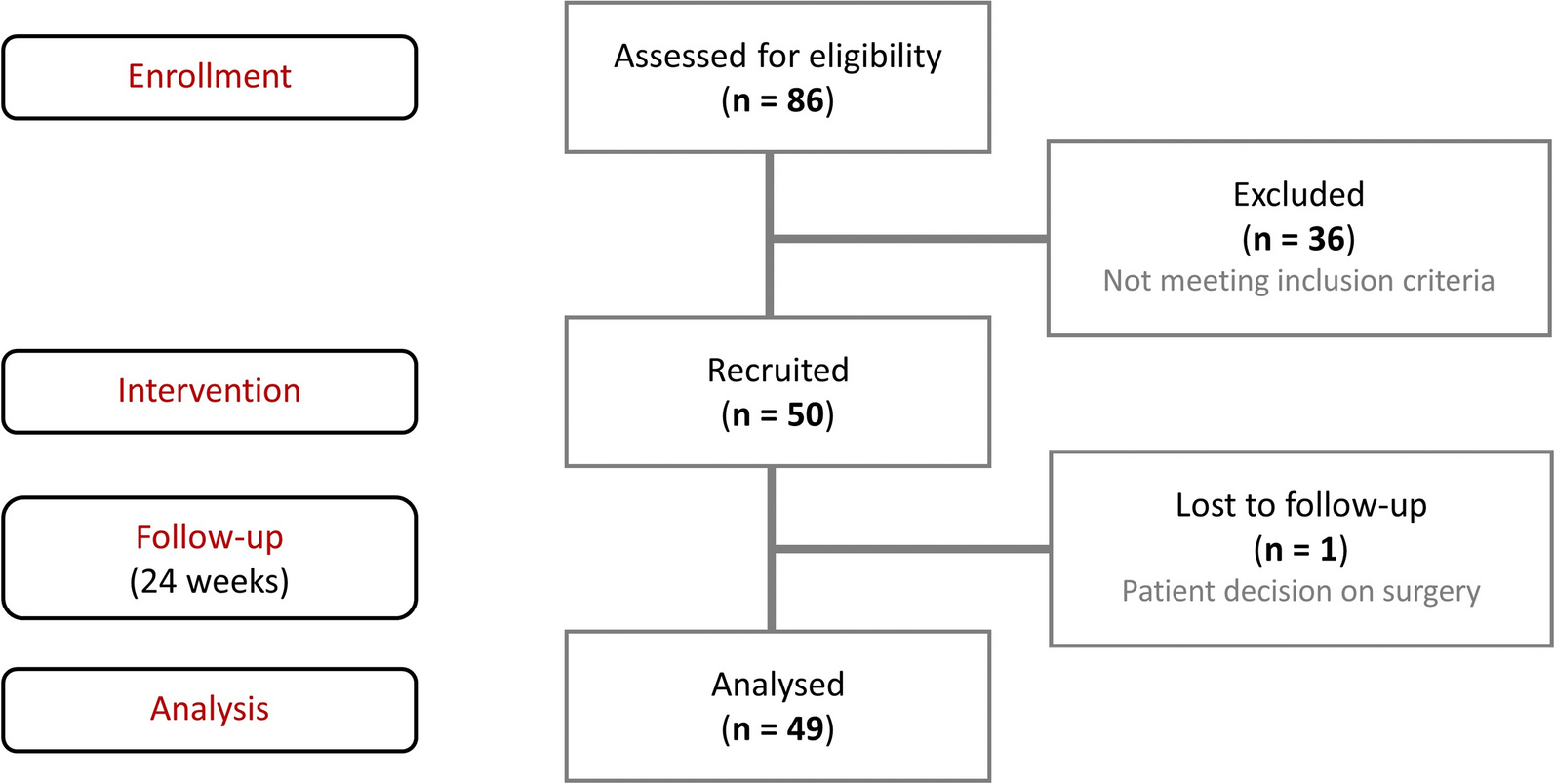
A total of 95 patients were enrolled in the ProDERM study, of whom 47 were randomized to receive IVIg and 48 were randomized to receive placebo in the first period, up to week 16. Of these, 45 patients (95.7%) in the IVIg group and 46 (95.8%) in the placebo group completed the first period. During the first period, five patients (10.4%) on placebo crossed over to IVIg and no patients on IVIg switched to placebo. In total, 69 (72.6%) patients completed the extension period.
Patient disposition was described in full previously [17]. In summary, 71 (74.7%) patients were female and the median (range) age was 52.0 years (22.0–79.0). The demographics and baseline characteristics of patients were generally balanced between the IVIg and placebo groups and are described in full in the previous publication [17].
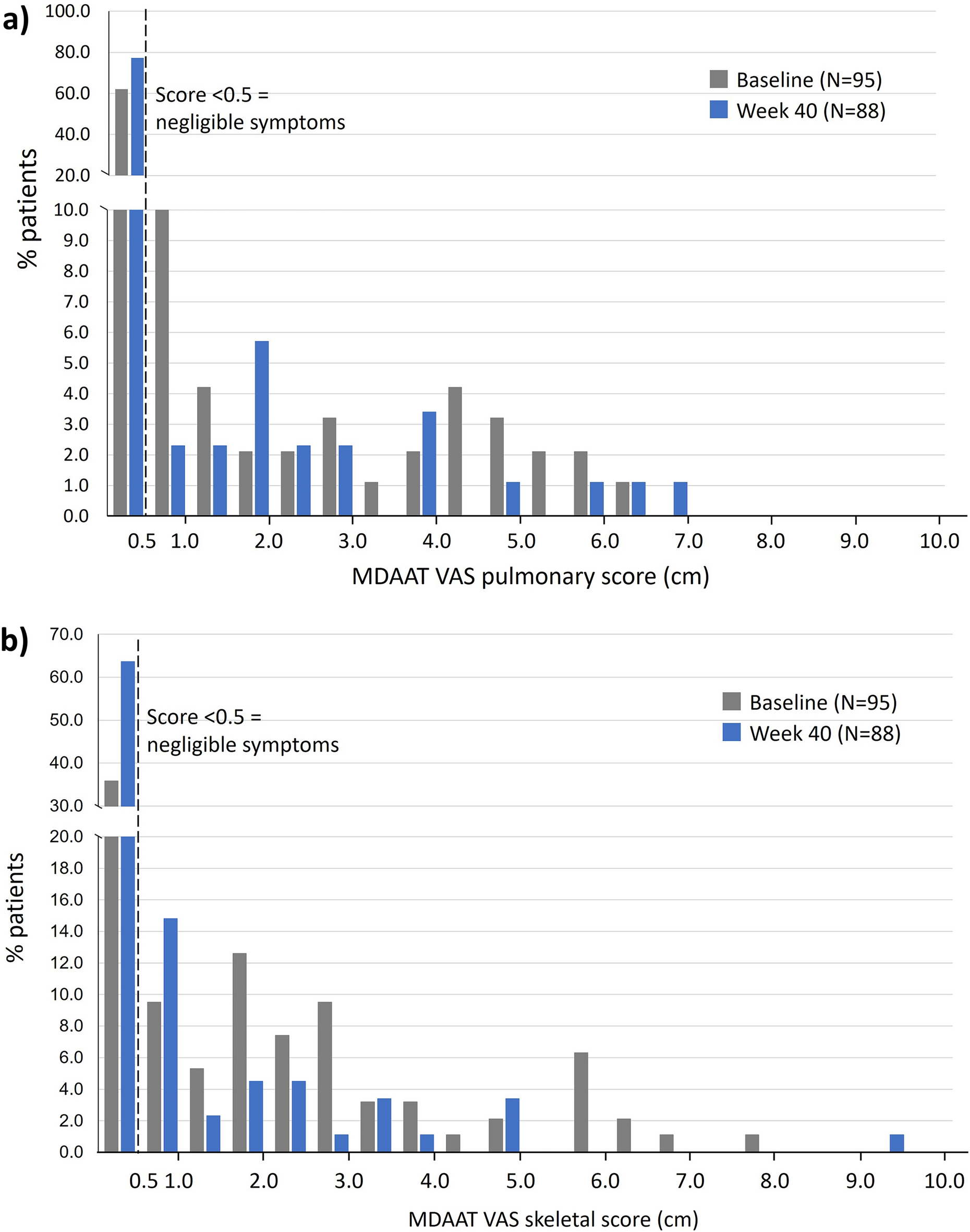
Spread of MDAAT VAS ScoresFor each of the five domains assessed using the MDAAT, the distribution of VAS scores at baseline was assessed. For the skeletal and constitutional domains, the majority of patients had symptoms at baseline (i.e., VAS > 0.5); of 95 patients, only 34 (35.8%) patients had VAS ≤ 0.5 for the skeletal domain, indicating no involvement, and 22 (23.2%) patients had VAS ≤ 0.5 for the constitutional domain (Fig. 1b, c; and Table S1 in the Supplementary Material). For the pulmonary and GI domains, more than half of the patients did not have involvement at baseline (n = 59 [62.1%] and n = 63 [66.3%], respectively) (Fig. 1a, d; and Table S1 in the Supplementary Material).
Fig. 1

MDAAT VAS score at baseline and week 40 for a pulmonary, b skeletal, c constitutional, and d gastrointestinal symptoms. MDAAT Myositis Disease Activity Assessment Tool, VAS visual analog scale
By week 40, the proportion of patients with no involvement (i.e., VAS ≤ 0.5) had increased significantly for all four domains, to the following (of 88 patients with available scores): no skeletal involvement, n = 56 (63.6%, P < 0.001); no constitutional involvement, n = 57 (64.8%; P < 0.001); no pulmonary involvement, n = 68 (77.3%, P = 0.007); and no GI involvement, n = 74 (84.1%; P < 0.001).
For the cardiovascular domain of the MDAAT, the majority of patients (80/95; 84.2%) had no involvement at baseline; this did not change significantly by week 40 (78/88 patients; 88.6%; P = 0.18) (Fig. S1a).
Mean MDAAT VAS Scores Over TimeFor patients with VAS ≥ 0.5 at baseline, a significant improvement in mean VAS score for the pulmonary, skeletal, constitutional, and GI domains was seen from baseline to week 16 for the IVIg group and from baseline to week 40 for the combined cohort (Fig. 2a–d and Table 1). From baseline to week 16 in the IVIg group, mean skeletal VAS decreased by 52.6% (1.62 cm; P < 0.001), constitutional VAS decreased by 44.4% (1.30 cm; P < 0.001), pulmonary VAS decreased by 37.7% (1.15 cm; P = 0.001), and GI VAS decreased by 49.2% (1.22 cm; P = 0.005). In contrast, no significant improvement for these domains was noted for the placebo group at week 16 except for constitutional VAS (Table 1). A significant difference was seen in the change in VAS scores through week 16 between the IVIg and placebo groups for the pulmonary and skeletal scores (both P = 0.02), but not for constitutional, GI, or cardiovascular scores (P = 0.18, P = 0.27, and P = 0.22, respectively). At week 40, following patients on placebo switching to IVIg, significant improvement was seen for the combined cohort as compared with baseline, as follows: mean pulmonary VAS decreased by 38.2% (1.08 cm), skeletal VAS decreased by 60.1% (1.75 cm), constitutional VAS decreased by 58.2% (1.70 cm), and GI VAS decreased by 51.0% (1.27 cm; P < 0.001 for all domains).
Fig. 2
Changes in MDAAT VAS scores from baseline for a pulmonary, b skeletal, c constitutional, and d gastrointestinal symptoms, in patients with baseline MDAAT VAS scores of ≥ 0.5. IVIg intravenous immunoglobulin, MDAAT Myositis Disease Activity Assessment Tool, VAS visual analog scale. Patients with MDAAT VAS score of < 0.5 at baseline were excluded from analysis
Table 1 Change in MDAAT VAS scores from baseline for patients with MDAAT VAS > 0.5, at week 16 and week 40For the cardiovascular domain (Fig. S1b), few patients had VAS ≥ 0.5 at baseline and data were not available for all patients at all timepoints, making it difficult to draw conclusions. However, from baseline to week 16 a decrease in VAS of 21.4% (0.43 cm) was observed for patients in the IVIg group, and from baseline to week 40 for the combined cohort of patients a decrease of 22.4% (0.52 cm) was seen; both decreases were of borderline significance (P = 0.06 and P = 0.05, respectively).
A similar pattern of improvement was seen when considering all patients, regardless of baseline VAS score, although the results were less pronounced for the GI and cardiovascular domains (Table S2 in the Supplementary Material).
To determine if response to IVIg was similar across all MDAAT domains in each patient or whether response varied between domains, improvement in VAS from baseline to week 40 was analyzed for the five domains described above (i.e., pulmonary, skeletal, constitutional, GI, and cardiovascular), as well as the cutaneous and extramuscular domains, which were described previously [18, 23]. For each patient, only domains in which they exhibited symptoms at baseline (i.e., had baseline VAS > 0.5) were considered, with response to IVIg classed as a decrease in VAS of > 0.5. For the 88 patients with scores available at both timepoints, overall, 52 (59.1%) showed improvement with IVIg in all domains in which they had symptoms at baseline. Five (5.7%) patients did not respond to IVIg in any affected domain that they exhibited symptoms at baseline. The remaining 32 (35.2%) patients showed improvement in some, but not all, domains.
Presence of Health Conditions Assessed by MDAAT MITAXThe presence or absence of individual health conditions associated with the pulmonary, skeletal, constitutional, GI, and cardiovascular domains was assessed by MDAAT MITAX, whereby a score of 1, 2, 3, or 4 indicated the presence of a health condition and 0 indicated its absence. At baseline, the most common health conditions present were fatigue (n = 72; 75.8%), arthralgia (n = 63; 66.3%), dysphagia (n = 38; 40.0%), arthritis (n = 35; 36.8%), dyspnea (n = 24; 25.5%), and dysphonia (n = 19; 20.0%), showing a marked systemic involvement of DM (Table S1 in the Supplementary Material).
For most health conditions, the number of patients experiencing each condition decreased numerically during the study in patients on IVIg, both to week 16 and week 40 (Fig. 3). At week 16, the proportion of patients with the following health conditions had decreased significantly from baseline in the IVIg group: arthritis (36.2 to 17.8%; P = 0.01), arthralgia (68.1 to 40.0%; P < 0.001), and fatigue (68.1 to 53.3%; P = 0.008). Also at week 16, there was a significant difference between the IVIg and placebo groups in the proportion of patients with arthritis (P = 0.04) and arthralgia (P = 0.009), and a numerical difference in the proportion of patients with fatigue, although this did not reach statistical significance (P = 0.07). By week 40, the proportion of patients with the following health conditions had decreased significantly from baseline in the combined cohort: dysphonia (20.0 to 8.1%; P = 0.04), arthralgia (66.3 to 39.8%; P < 0.001), weight loss (10.5 to 3.4%; P = 0.04), fatigue (75.8 to 50.0%; P < 0.001), and dysphagia (40.0 to 18.4%; P < 0.001). The percentage of patients with dyspnea from respiratory muscle weakness decreased numerically from baseline to week 16 in the IVIg group (25.5 to 17.8%; P = 0.25) and to week 40 in the combined cohort (25.5 to 20.9%; P = 0.69), although neither reached statistical significance.
Fig. 3
Percentage of patients with health conditions as recorded on the MDAAT MITAX scorea at baseline, week 16, and week 40. IVIg intravenous immunoglobulin, GI gastrointestinal, ILD interstitial lung disease, MDAAT Myositis Disease Activity Assessment Tool, MITAX Myositis Intention-To-Treat Activity Index. aPatients with a health condition described as 1—improving, 2—stable, 3—worsening, or 4—new, as per the MDAAT MITAX score. bSignificant difference between IVIg and placebo groups at week 16 (P < 0.05). cSignificant difference from baseline to week 16 (P < 0.05). dSignificant difference from baseline to week 40 (P < 0.05)
Severity of Health Conditions Assessed by MDAAT MITAXConsidering the change in MITAX scores on their original 5-point scale from baseline, at week 16 an improvement was seen for the following health conditions for patients in the IVIg group: dyspnea (P = 0.008), arthritis (P = 0.003), arthralgia (P < 0.001), and fatigue (P < 0.001) (Table 2; full breakdown of scores shown in Table S3 in the Supplementary Material). Improvement was also seen for arthritis (P = 0.02) and fatigue (P = 0.005) using this scaling system for patients in the placebo group at week 16. A significant difference in improvement in arthralgia was seen between the IVIg and placebo groups at week 16 (P = 0.002); numerical differences in improvement of other symptoms between the IVIg and placebo groups were seen but these did not reach statistical significance.
Table 2 Severity of health conditions as recorded on the MDAAT MITAX score at baseline versus week 16 and week 40By week 40, an improvement in the MITAX 5-point scale was seen for the following health conditions for patients in the combined cohort: dysphonia (P = 0.02), arthritis (P = 0.004), arthralgia (P < 0.001), weight loss (P = 0.01), fatigue (P < 0.001), and dysphagia (P < 0.001). For dyspnea, the changes in scores from baseline did not reach statistical significance (P = 0.17).
Comments (0)