
Remember me
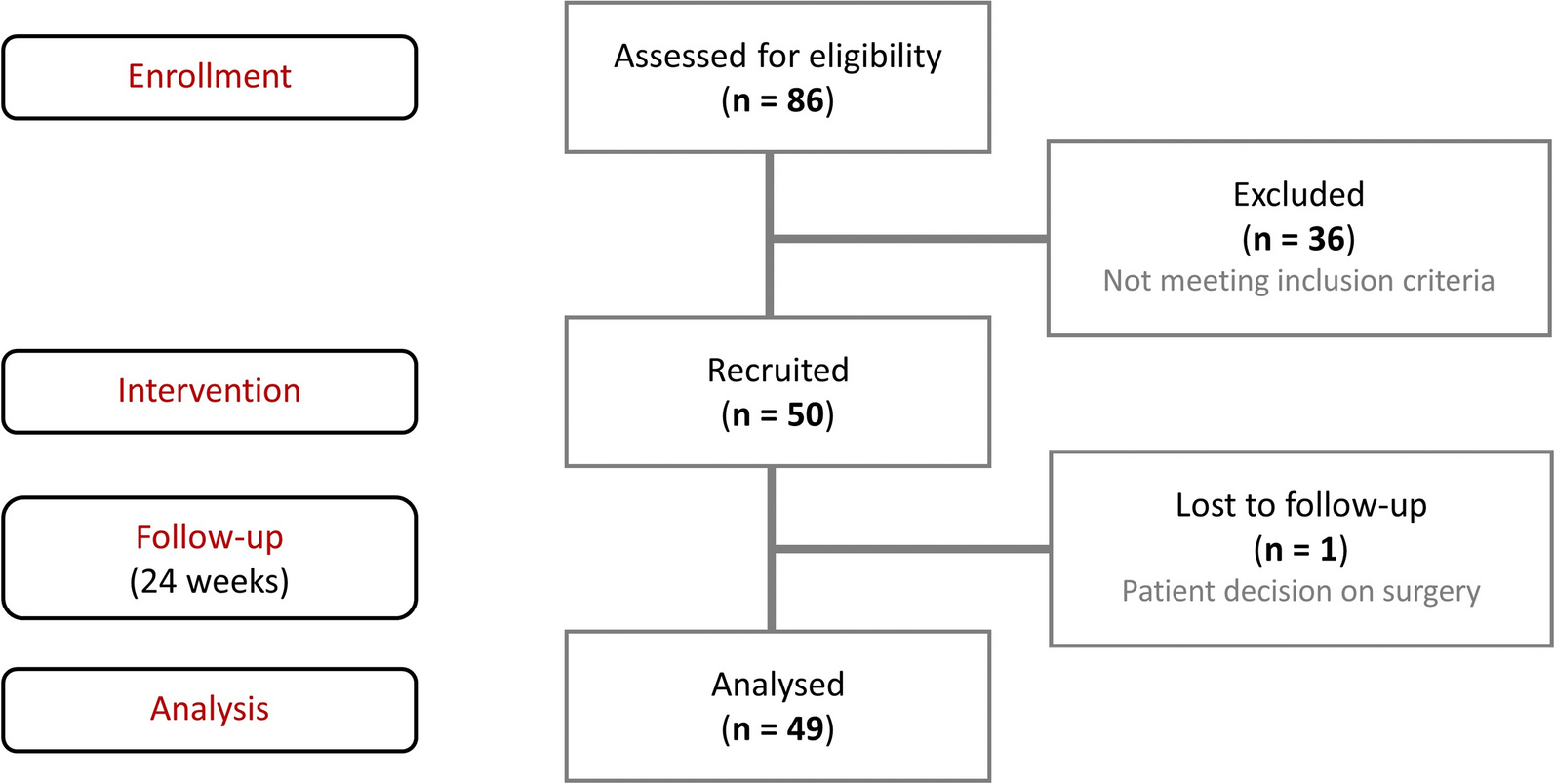
The SIRENA study enrolled 350 patients with SpA. Among them, the largest homogeneous subgroup (n = 203) was diagnosed with PsA, with the majority (91.6%) also fulfilling the CASPAR classification criteria.
A total of 171 of 203 (84.2%) patients attended the visit at 6 months, 130 (64.0%) at 12 months, 109 (53.7%) at 18 months and 120 (59.1%) at 24 months.
Baseline Demographics and Lifestyle DataThe demographic and lifestyle data are presented in Table 1. Of a total of 203 patients, 105 (51.7%) were males and 98 (48.3%) females, with a median age in both sexes equal to 52 (range: 18–82) years. Compared to males, females more frequently had a body mass index < 25 kg/m2 (p = 0.03) and were more frequently nonsmokers (p < 0.001) and non-drinkers (p = 0.002). Comorbidities were extremely frequent, with 190 of 203 (93.6%) patients with PsA reporting at least one concomitant disease. Endocrine disorders (p = 0.02), depression (p = 0.003) and fibromyalgia (p = 0.02) were more common in females than in males, whereas skin psoriasis at the time of baseline visit was more prevalent in males (90.5% vs 77.6% in females; p = 0.01). Ninety-two cases (45.3%) reported a familiar history of psoriasis, which was more frequent in females than in males (p = 0.02).
Table 1 Main demographic and lifestyle baseline characteristics of the patients with PsA observed in the SIRENA studyBaseline PsA CharacteristicsThe main PsA characteristics of the study population as a whole and split by sex are shown in Fig. 1. The vast majority of patients (95.6%) were classified as having predominantly peripheral PsA, 48.8% of whom had polyarthritis, which was significantly more common in females than in males (p = 0.01).
Fig. 1
Main baseline clinical characteristics of the patients with PsA observed in the SIRENA study. P-values for comparison of overall frequency distributions between females and males, computed using the chi-square/Fisher exact test, were 0.07 for predominant manifestations (A), 0.01 for articular involvement (B), 0.79 for new diagnosis of PsA vs confirmed diagnosis (C) and 0.34 for time from musculoskeletal symptoms to PsA diagnosis (D). Articular involvement at baseline was categorized as monoarthritis (i.e., one swollen or tender joint), oligoarthritis (i.e., 2 to 4 swollen or tender joints) or polyarthritis (i.e., ≥ 5 swollen or tender joints)
At the time of enrolment, 77.3% of patients received a new diagnosis of PsA, while in 22.7% of cases a previously established diagnosis was confirmed. The interval between the onset of the first musculoskeletal symptoms and PsA diagnosis was comparable between sexes, with 32.0% of patients (30.6% of females vs 33.3% of males) experiencing a diagnostic delay of ≥ 24 months. The median time from symptom onset to confirmed PsA diagnosis was 24.0 months overall (23.0 months in females vs 24.0 months in males).
Clinical RemissionThe main clinical outcomes, including the achievement of MDA and DAPSA remission (i.e., score ≤ 4) during follow-up, are shown in Table 2 as an overall data and split between males and females. About 15% of patients (n = 23/158) were already in MDA at the time of inclusion in the study (8.2% of females [n = 6/73] vs 20.0% of males [n = 17/85], p = 0.036). This percentage increased to 55.3% (n = 83/150) at month 6 (44.1% of females [n = 30/68] vs 64.6% of males [n = 53/82], p = 0.012), 59.8% (n = 67/112) at month 12 (43.8% of females [n = 21/48] vs 71.9% of males [n = 46/64], p = 0.003), and 75.3% (n = 73/97) at month 24 (65.9% of females [n = 27/41] vs 82.1% of males [n = 46/56], p = 0.066). After excluding patients with MDA at baseline from the calculation, the 6-month rate of MDA was 43.3% (n = 65/150) in the overall population, 38.2% (n = 26/68) in females and 47.6% (n = 39/82) in males (p = 0.06). One hundred two of 165 (61.8%) evaluable patients reached MDA at any time over the study period (56.8% of females [n = 46/81] vs 66.7% of males [n = 56/84], p = 0.19), with a median time to reach MDA of 10.0 months overall, 13.0 months in females and 7.0 months in males (p from log-rank test = 0.031). The percentage of patients with DAPSA remission increased from 6.5% at baseline (2.7% of females [n = 2/74] vs 9.4% of males [n = 9/96], p = 0.08), to 36.3% at month 6 (32.1% of females [n = 17/53] vs 39.4% of males [n = 28/71], p = 0.40) and to 50.0% at month 24 (47.4% of females [n = 18/38] vs 52.3% of males [n = 23/44], p = 0.66).
Table 2 MDA and DAPSA remission outcomes over the study period, overall and according to sexOther Clinical Outcomes and PROsAs described in Table 3, the comparative analysis of baseline values of disease activity measures after stratification by sex showed a significantly higher burden of articular disease in females than in males in terms of TJC68 (mean count: 9.3 vs 5.3, respectively; p < 0.01), VAS PhGA (mean 51.9 vs 41.7, respectively; p < 0.01), VAS Physician assessment for joints (mean 47.9 vs 40.4, respectively; p < 0.05), DAS28 (mean 4.0 vs 3.4, respectively; p < 0.01) and DAPSA score (mean 26.0 vs 18.7, respectively; p < 0.01). A similar pattern was also observed for the baseline PROs, with significantly less favourable values in females than in males for VAS PtGA (p < 0.01), HAQ-DI (p < 0.01), VAS Pain (p < 0.01), VAS Sleep (p < 0.01), BASFI (p < 0.01) and BASDAI (p < 0.01).
Table 3 Clinical outcomes, PROs and laboratory findings—mean (SD)—over the study period, overall and according to sexFor several clinical outcomes and PROs, including SJC66, TJC68, VAS PhGA, VAS Physician assessment for joints, VAS Physician assessment for skin, HAQ-DI and VAS PtGA, a significant clinical improvement was reported at all follow-up visits in females, males and overall population (all p-values were < 0.01). For most clinical indexes, a somewhat stronger burden of disease emerged in females throughout the follow-up period, although only in a few cases were the differences between sexes statistically significant (i.e., for VAS PhGA, VAS Physician Sssessment for joints and DAPSA score at month 6 and for nail psoriasis at month 24). Significant differences in mean PRO scores between sexes were reported at all visits for VAS PtGA, and at all visits except at month 24 for HAQ-DI, always showing a worse disease status in females.
Treatment Pattern During the Observational PeriodAt the baseline visit, 177/203 (87.2%) patients were prescribed systemic therapy, mainly in treatment with conventional synthetic (49.3%) or biological (24.6%) DMARDs (Table 4). Data at 6 months showed that 90.6% of the patients reaching this timepoint were still in treatment with DMARDs, with an increased proportion of patients receiving a bDMARD (61/155, 39.4%). Eighty-one (81/203, 39.9%) patients started a bDMARD during the study. Median time to switch from a non-biological to a biological DMARD was 6.8 months, longer in females than in males (mean 10.4 vs 6.2 months, respectively; p = 0.003). On the other hand, median time to switch from a biological to another biological DMARD was 10.0 months, similar in females (mean 10.3 months) and males (mean 10.0 months).
Table 4 Treatment choice during the observational study periodaFactors Influencing MDA AchievementResults from logistic regression analysis on predictors of achieving 6-month MDA are shown in Fig. 2. In univariate analyses (Panel A), factors positively associated with MDA achievement at 6 months included age (OR = 1.03, 95% CI 1.00–1.05, per 1 year increase), new versus pre-existent PsA diagnosis (OR = 2.62, 95% CI 1.05–6.54), pattern of joint involvement (OR = 2.67, 95% CI 0.78–9.09, for monoarthritis and OR = 2.19, 95% CI 1.00–4.80, for oligoarthritis vs polyarthritis) and baseline DAPSA score (≤ 14 vs > 28, OR = 4.93, 95% CI 1.67–14.56). However, factors inversely associated with MDA achievement at 6 months included female sex (OR = 0.51, 95% CI 0.26–1.02), BSA < 3% (OR = 0.44, 95% CI 0.19–1.03), TJC68 (OR = 0.96, 95% CI 0.92–1.01, for 1 point increase) and HAQ-DI score (OR = 0.53, 95% CI 0.28–0.99, for 1 point increase). In the multivariate analysis (Panel B), which included all the aforementioned covariates, mutually adjusted, none of the factors emerged as a significant independent predictor of MDA achievement at month 6.
Fig. 2
Predictors of reaching MDA at 6 months in univariate (A) and multivariate (B) analyses. BSA body surface area, CI confidence interval, HAQ-DI Health Assessment Questionnaire Disability Index, DAPSA Disease Activity Index for Psoriatic Arthritis, MDA minimal disease activity, OR odds ratio, TJC tender joints count. Joint involvement was categorized as monoarticular (i.e., one swollen or tender joint), oligoarticular (i.e., 2–4 swollen or tender joints) or polyarticular (i.e., ≥ 5 swollen or tender joints)
Comments (0)