In this study, we sought to explore whether the choice of perspective affects the results of EQ-5D-Y-3L valuation tasks using both the OPUF tool and a DCE. With both methods, differences were identified between the perspectives, but the extent of these differences varied.
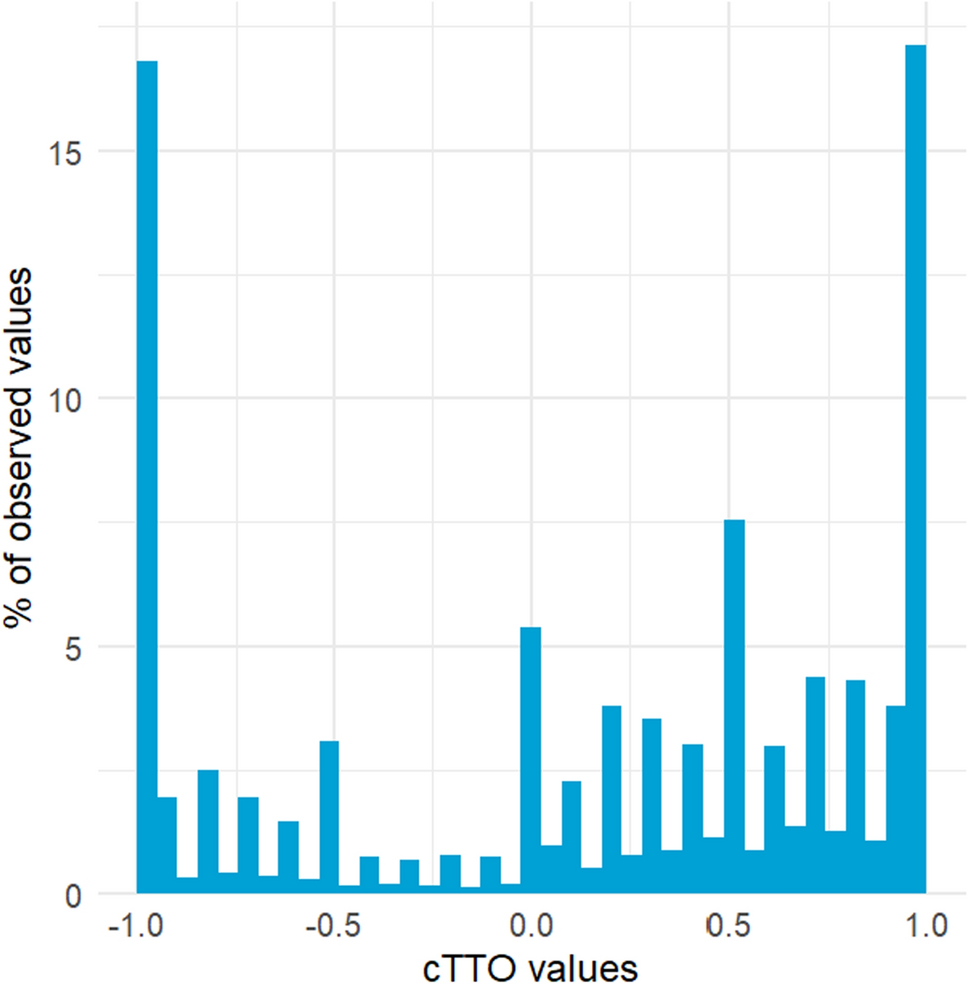
In the component of the OPUF tool that explored the RI of the five dimensions, ‘looking after myself’ was consistently less important, and ‘pain or discomfort’ was consistently more important, for children than for adults. Other dimensions had similar levels of importance both within and between perspectives. In terms of the scale of the value sets produced, the child perspective value sets were narrower (with higher values for 33333) because a smaller proportion of respondents considered 33333 to be worse than dead when considering a child perspective (31.8% for the adult self-perspective was the highest, whereas the lowest was 17.7% for the 10-year-old child perspective). In relation to scale, there were some differences within the different child and adult arms. Although 33333 was considered worse than dead by a similar proportion for the 4-year-old and 10-year-old child perspectives (18.6% and 17.7%, respectively), 25% of respondents taking the perspective of a child of unspecified age considered 33333 to be worse than dead. Furthermore, a greater proportion of respondents in the adult self-perspective arm considered 33333 to be worse than dead than in the other adult arm (31.8% vs. 25.4%).
The DCE only provided RI results, but these were considerably more varied than those from the OPUF tool, both within and between dimensions. Similar to the OPUF results, ‘looking after myself’ was consistently less important and ‘pain or discomfort’ was consistently more important in the child perspectives than in the adult perspectives (though to a far greater extent in terms of RI scores). There were also further differences, such as ‘worried, sad or unhappy’ being less important for adults and ‘looking after myself’ being less important under a 4-year-old child perspective than under the other child perspectives.
The OPUF-derived EQ-5D-Y-3L value sets suggest that adult respondents valued child health states somewhat higher when they imagined children experiencing these health states as opposed to another adult or themselves. This is the first study to explore differences by perspective using OPUF, but past studies using cTTO have found similar results [23, 25, 26]. Given that the OPUF anchoring-VAS task was based on a direct choice (between 33333 and dead) followed by a rating scale, our results cannot be explained in the same way as those from the literature (i.e., that adult respondents are less willing to trade-off life-years on behalf of children than they are for adults). Our results suggest that adults are also relatively hesitant to state that, for a child, being dead is better than being in 33333 (the first part of the task), pointing towards death aversion in this context. However, it is also worth noting that the value sets were still relatively narrow in the adult perspectives in our study, compared with value sets for adult instruments (e.g., EQ-5D-3L or EQ-5D-5L). It is unclear whether this is driven by the method (e.g., the direct nature of the first anchoring-VAS question, and/or the lack of a temporal component) or whether 33333 on the EQ-5D-Y-3L is genuinely viewed as being better than dead by most adults when considering an adult perspective. Although this is typically not the case for 33333 in EQ-5D-3L value sets, or 55555 in EQ-5D-5L value sets, the significant differences in language between these instruments and the EQ-5D-Y-3L may partly explain these differences. For example, ‘anxiety/depression’ in the EQ-5D-3L/EQ-5D-5L is labelled as ‘worried, sad or unhappy’ in the EQ-5D-Y-3L, which may create less concern.
In our study, the RI of three of the EQ-5D-Y-3L dimensions (‘looking after myself’, ‘pain or discomfort’, and ‘worried, sad or unhappy’) appeared to depend on whether a child or adult perspective was taken, irrespective of the method used. The ‘looking after myself’ differences may be explained by the fact that children are already relatively dependent on their parents/guardians, so changes relating to self-care are less important than for independent adults. The ‘pain or discomfort’ differences may be because people have a stronger aversion to imagining pain or discomfort being experienced by children than by themselves, and perhaps also because they perceive adults as having a greater tolerance of pain and discomfort. The ‘worried, sad or unhappy’ differences may also be explained by people having a stronger aversion to imagining children feeling this way. It may also be the case that, although this wording may feel appropriate in the child perspectives, it may seem less severe (than anxiety/depression, for example) when adults are considering this dimension for themselves or other adults. Regardless of the reasons for these differences, the consistency in our results suggests that the choice between an adult or a child perspective may affect the RI of different dimensions of health in valuation studies. Researchers should consider this, in addition to the expected impact on the scale of the value sets, and the consequences for the generation of QALYs and, ultimately, reimbursement decisions [18].
The DCE results in our study go one step further and suggest that ‘looking after myself’ is perceived, by adults, to be less important for younger children than for older children. This may be because younger children are relatively more dependent on their parents/guardians than older children. Although this is not directly supported by the OPUF results, it is worth noting that the variation in the RI of the dimensions in the OPUF task was far more limited overall, perhaps due to its nature (a single swing-weighting exercise vs. a series of 15 forced-choice tasks).
Our RI results are in direct contrast to those of Ramos-Goni et al. [22], who found no substantial differences in DCE results between a range of different perspectives, which included an adult self-perspective as well as four different child perspectives: ages 5–7 years, 8–10 years, 11–13 years, and 14–15 years. An important difference between our study and theirs, which may have had an impact, is that all respondents in their study completed DCE tasks with every perspective. In contrast, in our study, different respondents completed the task with each perspective. On one hand, our respondents only had to focus on a single perspective throughout, which may have enabled them to more consistently and carefully consider the impact of the health states on the proxy or themselves. On the other hand, the nature of multi-arm studies such as ours means we cannot rule out that the differences between perspectives were driven by differences in underlying preferences between the samples. This is a limitation of our study. That said, the demographic characteristics in each of our samples, and particularly the 4-year-old and 10-year-old child arms, were remarkably similar. Furthermore, it is worth acknowledging that a recent cognitive debriefing study that used the OPUF tool—albeit in the context of valuing a different instrument (EQ-HWB-9)—revealed some concerns about the method, suggesting that interviewer-led data collection may be preferred to ensure data quality [34]. Given that our study used online self-completion, this is a further limitation of our study.
Stakeholder engagement is an increasingly important aspect of valuation studies, particularly when the instrument being valued is for children or adolescents [21, 35, 36]. Our study highlights that the choice of perspective, among other important considerations, such as whose preferences to elicit (e.g., adults vs. children and/or adolescents) and which elicitation technique to use (e.g., DCE vs. best–worst scaling), is also an important consideration. Furthermore, should stakeholders and researchers opt to collect data using multiple perspectives, it is likely that the resulting value sets will have different characteristics, which may create dilemmas when ultimately deciding upon which value set to use in practice (for which no definitive criteria currently exist). As such, it is advisable for research teams to seek a consensus view with stakeholders on the choice of perspective before embarking on their valuation study. It is also worth noting that deciding on a perspective may be particularly challenging if studies aim to elicit both adult and adolescent preferences [21], given that the former are likely to take a child proxy perspective, whereas it is not clear whether it would be feasible for the latter to also do so, given the complexity of valuation tasks [37,38,39].




Comments (0)