In the present study, which included over 500 patients with obstructive sleep apnea (OSA), we found that none of the polysomnographic parameters indicative of OSA severity, such as the apnea-hypopnea index (AHI), oxygen desaturation index (ODI), mean saturation, minimal saturation, time with SpO2 < 90% were significantly associated with lactate levels in OSA patients who were treated with metformin for type 2 diabetes. Similarly, we did not find significant associations between lactate levels and patient age, sex, or degree of obesity. We confirmed, however, that in the subgroup of patients with diabetes, metformin use affects lactate levels. To the best of our knowledge, no prior studies have investigated lactate levels in patients with OSA and concurrent type 2 diabetes treated with metformin. We found no published data on factors influencing lactate levels in such patients. However, metabolomic studies in individuals with OSA and even single snorers suggest that sleep-related breathing disorders may affect lactate levels [14].
Data from the presented study support the hypothesis that intermittent hypoxia, typical of OSA, may not be sufficient to activate anaerobic respiration, which would result in substantial lactate production. It is well established that lactate accumulation is more closely related to the magnitude of oxygen debt incurred in response to hypoxia rather than to the severity of hypoxia itself [15]. Thus, it may seem that intermittent hypoxia in OSA does not lead to significant oxygen debt, and intermittent reoxygenation allows for sufficient compensation of homeostasis to maintain oxygen metabolism.
Our findings differ from those reported by Ucar et al. [6], who suggested that lactate may serve as a marker of hypoxia in patients with sleep-related breathing disorders. However, importantly, in their study, lactate levels in patients with OSA were not significantly different from those in healthy controls. Furthermore, their cohort included individuals with underlying conditions that cause hypoventilation and hypoxia, such as neuromuscular diseases, chest deformities, and chronic obstructive pulmonary disease (COPD), which were not present in our study population. This suggests that the overlap of chronic and intermittent hypoxia (as in the Ucar et al. study) may activate different pathomechanisms than intermittent hypoxia alone (as in our group). This interpretation is supported by evidence indicating that there are several important differences in how intermittent and chronic hypoxia affect cell behavior [16]. These include a number of phenomena connected inter alia to the activation and degradation of hypoxia-inducible factor 1-alpha (HIF-1α) [17].
Furthermore, both our findings and those of Ucar et al. highlight the clinical importance of identifying patients with sleep-related hypoventilation and chronic hypoxia. Hira et al. reported that nocturnal lactate levels increase in patients with OSA [18]. In our study, however, the lactate level was measured at a single time point, precluding analysis of its changes over time. The maximum lactate level observed in our cohort was 3.8 mmol/L, which does not exceed levels typically considered elevated [5]. We are aware that our study assessed lactate concentrations but did not directly evaluate the risk of acute lactic acidosis. Nevertheless, it was reported that lactate levels exceeding 4 mmol/L may be associated with poor clinical outcomes, whereas severe hyperlactatemia with accompanying acidosis is typically defined by lactate levels above 5 mmol/L [19, 20]. Given these thresholds, the risk of lactic acidosis in OSA patients treated with metformin appears negligible.
A further independent finding from our study is the identification of active smoking as a factor associated with elevated lactate levels in patients treated with metformin. Three mechanisms may contribute to this phenomenon. Smoking may influence lactate metabolism through increased lactate dehydrogenase (LDH) activity [21], elevated carbon monoxide levels [22,23,24], and when cyanide present in tobacco smoke is absorbed into the blood [25, 26]. Additionally, apart from the chemical reactions, the inhalation of hot gases alone has been shown to increase lactate levels [27].
Collectively, these observations support our conclusion that metformin use in patients with sleep-disordered breathing and type 2 diabetes is safe in terms of potential disturbances in the lactate metabolism. However, this finding is limited to situations in which hypoxia/hypoventilation is not additionally observed during sleep. Active smoking appears to contribute to hyperlactatemia in patients treated with metformin, providing further rationale for targeted smoking cessation efforts in this patient population. This finding is clinically relevant because, despite the recent expansion of therapeutic options, metformin continues to be the first-line treatment for type 2 diabetes [28]. Given the growing prevalence of obesity and OSA, the cooccurrence of OSA and type 2 diabetes is expected to increase, further highlighting the importance of safe metformin use in this patient population [29].
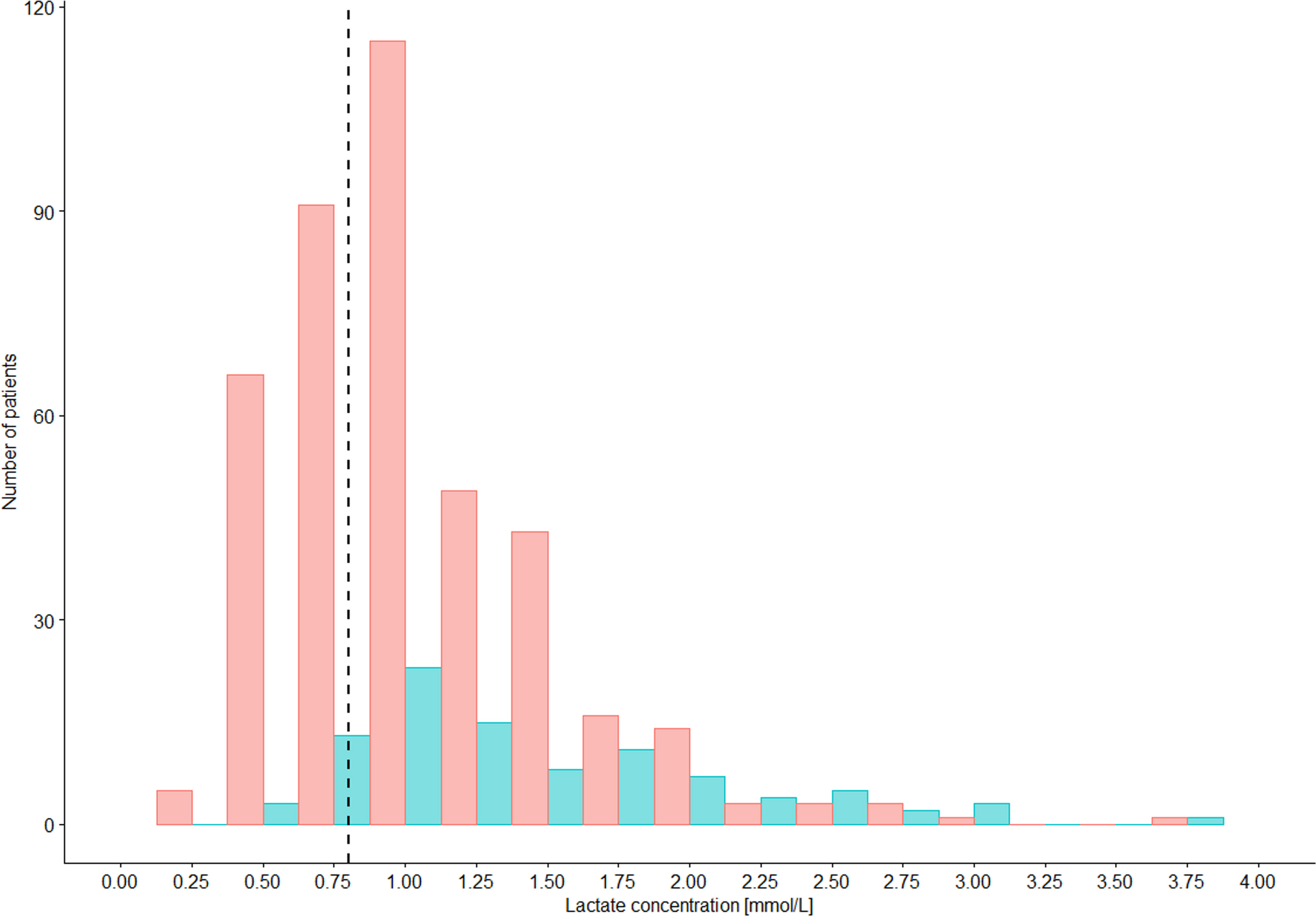
Our study did not include patients treated with continuous positive airway pressure (CPAP), and we did not analyze the effects of CPAP on lactate levels. Interestingly, the literature on this subject shows contradictory results. Lin et al. reported a reduction in serum lactate following CPAP therapy [29], whereas Cooper et al. found no such effect [30]. Caution is warranted when comparing these studies with ours, as differences in lactate measurement methodologies and reference ranges limit direct comparisons. For example, Ucar et al. defined normal lactate level as 0.5–2.0 mmol/L [6], whereas in our study, the threshold value was > 0.8 mmol/L.
We should mention that our study has some limitations. First, the absence of a healthy control group limits our ability to draw definitive conclusions about lactate levels in relation to the diagnosis of OSA. Second, lactate was assessed at a single time point, which prevents analysis of temporal changes or nocturnal dynamics in patients treated with metformin.



Comments (0)