
Remember me




Total hip arthroplasty (THA) is one of the most successful procedures performed today, with one of the highest levels of postoperative patient satisfaction among various surgical procedures. The rate of primary THA is rapidly increasing with studies projecting growth to 635,000 surgeries by 2030, a greater growth than projections for total knee arthroplasty. As implant survivorship continues to improve and more patients become candidates for surgery, it is important to scrutinize the risk of adverse events in patients with common musculoskeletal pathologies, such as scoliosis.
Scoliosis is a coronal plane deformity of the spine that classically manifests in pediatric and adolescent patients, though undiagnosed scoliosis can have a substantial effect on function and quality of life in adults. Moreover, this untreated scoliosis may manifest later in life as degenerative scoliosis. Although the complex interplay between pathologies of the hip and spine has been heavily studied, these studies almost exclusively comment on spinopelvic imbalance in the sagittal plane. Unfortunately, parameters such as pelvic tilt, pelvic incidence, and sacral slope do not fully consider the three-dimensional orientation of the pelvis, especially in the context of scoliosis. Recent biomechanical data suggest that sacropelvic parameters were correlated to the lumbar lordosis in a scoliotic spine which can affect postural balance.1 It is unclear whether coronal plane imbalances, such as those seen in patients with scoliosis, affect outcomes, specifically dislocation risk, after primary THA. Furthermore, there is a growing body of evidence suggesting that scoliosis is a three-dimensional deformity.2 In fact, the Scoliosis Research Society reported that idiopathic scoliosis is a rotational or torsional deformity for which predominantly coronal plane measurements such as plain radiographs and Cobb angles may be too elementary to comprehensively evaluate.3
There is a paucity of literature on the effect of scoliosis, in the absence of a fusion procedure, on outcomes after THA. The authors hypothesize that the biomechanical alterations to normal spinopelvic parameters increase risk of medical and, importantly, arthroplasty-related complications after THA. These findings will have important ramifications for how these patients are evaluated both in the preoperative and perioperative periods after THA to reduce the risk of adverse events.
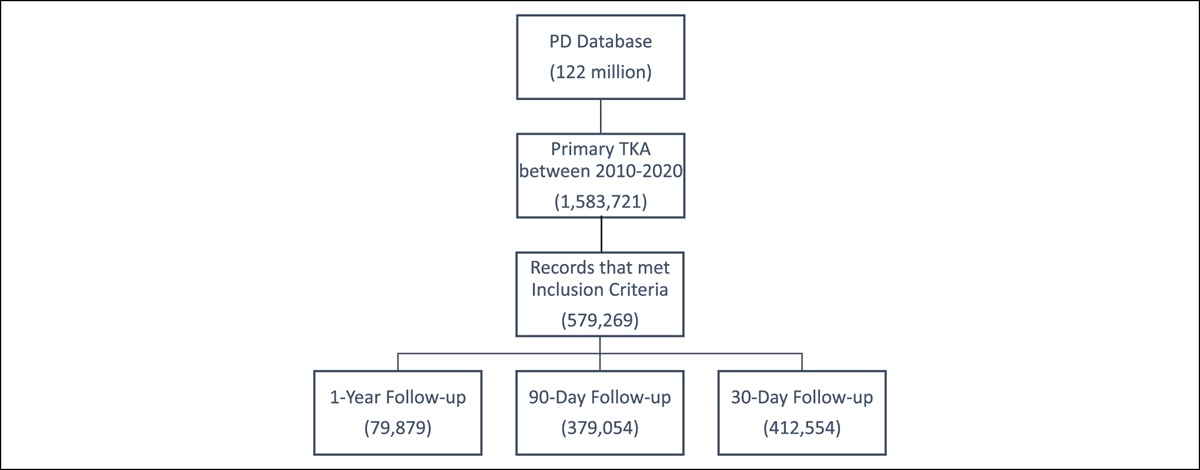
MethodsThis was a retrospective cohort study performed using the commercially available Mariner database via PearlDiver (PearlDiver) patient records database. Mariner is a large, anonymized insurance data set for 121 million patients in the United States. Patient records from 2010 to the second quarter of 2019 were searched using International Classification of Diseases (ICD) and Current Procedural Terminology codes. All queried data were deidentified in accordance with the Health Insurance Portability and Accountability Act. Therefore, this study was deemed exempt from our institution's review board process.
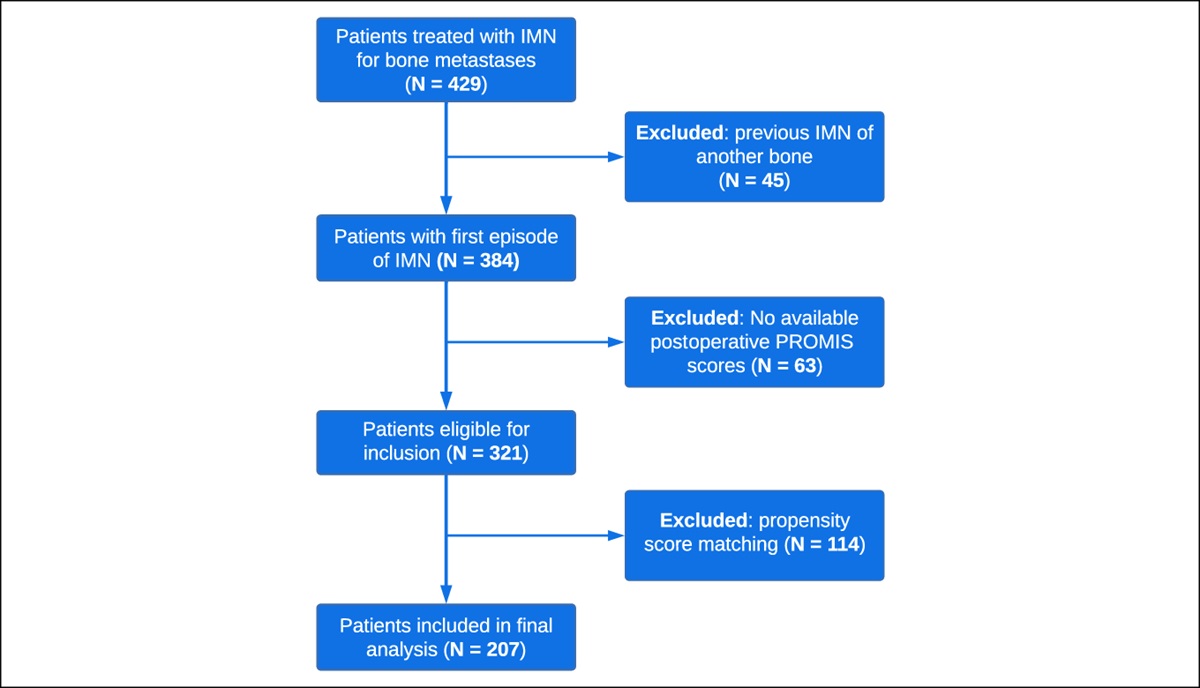
Patients with a preoperative diagnosis of infantile, pediatric, or adolescent scoliosis who underwent primary, elective THA with at least 90 days of postoperative follow-up in the database were identified using Current Procedural Terminology, ICD-9 and ICD-10 coding (Table 1). Possible confounding variables that were evaluated were age, sex, and preoperative diagnoses of uncomplicated diabetes, chronic kidney disease, obesity, ischemic heart disease, and tobacco abuse using ICD-9/10 coding. Patients with a preoperative diagnosis of scoliosis were matched using propensity scoring with patients without a preoperative diagnosis of scoliosis based on the aforementioned demographic and comorbid variables. All patients who underwent any fusion for scoliosis were excluded from this study to avoid fusion, a known risk factor for adverse events after THA, as a confounding variable.
Table 1 - International Classification of Disease-9 and 10 Codes for Scoliosis Codes Scoliosis ICD-9-D-73730, ICD-9-D-73732, ICD-9-D-73734, ICD-9-D-73739, ICD-9-D-73743, ICD-10-D-M419, ICD-10-D-M4186, ICD-10-D-M4120, ICD-10-D-M4185, ICD-10-D-M4126, ICD-10-D-M4184, ICD-10-D-M4125, ICD-10-D-M41125, ICD-10-D-M4124, ICD-10-D-M41124, ICD-10-D-M4180, ICD-10-D-M41129, ICD-10-D-M41115, ICD-10-D-M41126, ICD-10-D-M4150, ICD-10-D-M4134, ICD-10-D-M4156, ICD-10-D-M4187, ICD-10-D-M4145, ICD-10-D-M41114, ICD-10-D-M4140, ICD-10-D-M4135, ICD-10-D-M4182, ICD-10-D-M41119, ICD-10-D-M4127, ICD-10-D-M4155, ICD-10-D-M4144, ICD-10-D-M41116, ICD-10-D-M4146, ICD-10-D-M4130, ICD-10-D-M4123, ICD-10-D-M4122, ICD-10-D-M4183, ICD-10-D-M41127, ICD-10-D-M41123, ICD-10-D-M4157 Lumbar fusion CPT-22558, CPT-22585, CPT-22853, CPT-22845, CPT-22846, CPT-22847, CPT-22630, CPT-22632, CPT-22633, CPT-22634, CPT-22612, CPT-22614, CPT-22840, CPT-22842, CPT-22843, CPT-22844The main healthcare utilization outcomes evaluated were 90-day incidence of readmission, emergency department (ED) visit, reimbursement, and length of stay. The main surgery-related outcomes evaluated were 1-year incidence of diagnosis of periprosthetic joint infection (PJI), periprosthetic fracture, prosthetic dislocation, aseptic loosening, and broken implant.
The main medical complications that were evaluated were 90-day incidence of pulmonary embolism, deep vein thrombosis, myocardial infarction, cerebrovascular accident, need for transfusion, pneumonia, sepsis, acute hemorrhagic anemia, acute renal failure, and urinary tract infection.
In the totality, 21,992 patients with a preoperative history of scoliosis before THA who were matched in propensity scoring methodology in a ratio of 1:10 based on age, sex, and various medical comorbidities including coronary artery disease, uncomplicated diabetes mellitus, obesity, tobacco abuse, chronic pulmonary disease, liver disease, peripheral vascular disease, renal disease, and cancer to a control cohort.
Adjusted odds ratio (ORs) and 95% confidence intervals (CIs) were calculated for each variable independently using R (University of Auckland, New Zealand). Comparisons of continuous variables, including reimbursement and length of stay, were performed using Student t-test in R. A P-value less than 0.05 was used to ascribe statistical significance.
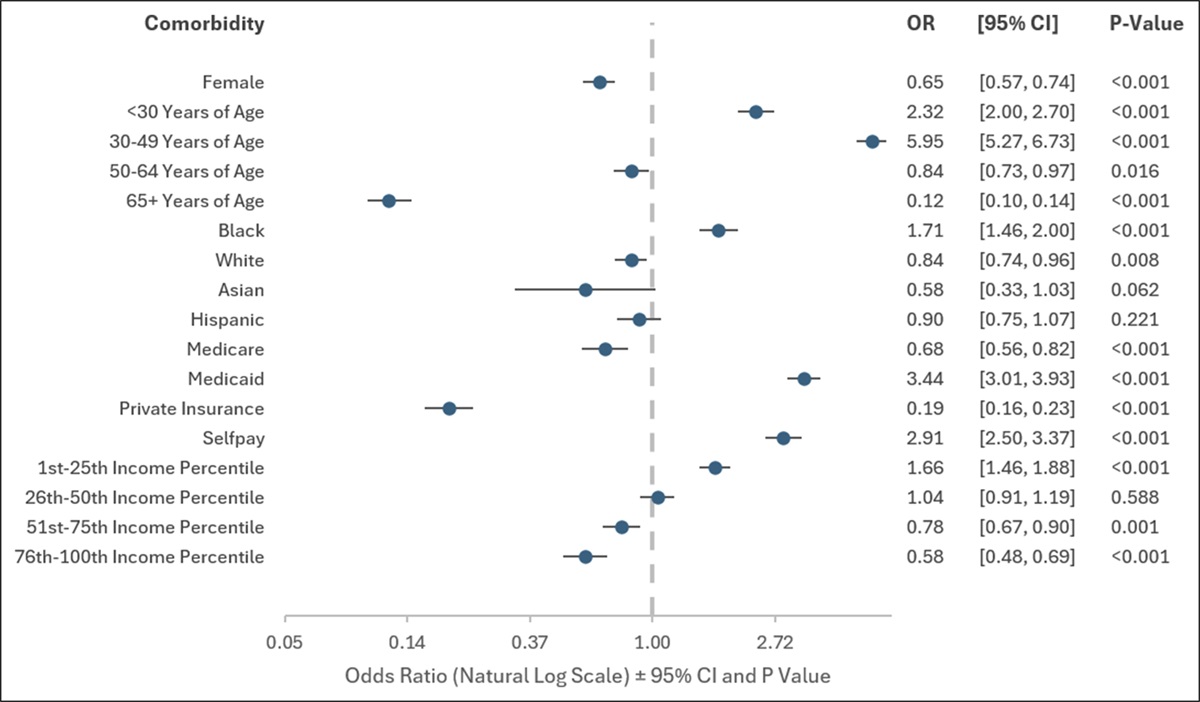
ResultsA total of 552,567 patients underwent primary THA from 2010 to 2019 were identified with at least 90 days of postoperative follow-up, and 78,107 patients were identified with scoliosis and no preoperative history of spinal fusion who underwent primary THA. In total, 21, 992 patients with scoliosis without fusion were matched in propensity scoring to 219,920 patients without a diagnosis of scoliosis before THA (Table 2). The scoliosis cohort was associated with a significantly higher 90-day incidence of pulmonary embolism (OR, 1.96; 95% CI, 1.26 to 1.82; P < 0.001), deep vein thrombosis (OR, 1.49; 95% CI, 1.30 to 1.70; P < 0.001), transfusion (OR, 1.13; 95% CI, 1.05 to 1.21; P < 0.001), pneumonia (OR, 1.37; 95% CI, 1.20 to 1.57; P < 0.001), cerebrovascular accident (OR, 1.26; 95% CI, 1.01 to 1.56; P = 0.045), myocardial infarction (OR, 1.38; 95% CI, 1.09 to 1.75; P = 0.008), sepsis (OR, 1.59; 95% CI, 1.36 to 1.85; P < 0.001), acute posthemorrhagic anemia (OR, 1.21; 95% CI, 1.10 to 1.34; P = 0.0002), and urinary tract infection (OR, 1.10; 95% CI, 1.04 to 1.16; P = 0.0012) compared with a control cohort (Table 3).
Table 2 - Patient Demographics and Comorbidities After Propensity Score Matching Total Hip Arthroplasty Scoliosis Control P Age 60-64 12.2 12.2 1 65-69 18.8 16.7 0.597 70-74 27.5 29.1 0.259 75-79 20.6 27.7 0.538 80-84 5.0 5.7 0.631 Male 57.625 42.8 0.571 Obesity 50.170 54.550 0.325 ETOH 3.891 3.619 0.385 Chronic kidney disease 11.985 11.971 0.979 Chronic pulmonary disease 33.098 34.213 0.152 Congestive heart failure 10.203 10.135 0.891 Coronary artery disease 28.200 28.404 0.783 Depression 32.159 34.676 0.562 Diabetes mellitus 43.246 45.245 0.227 HTN 79.254 81.281 0.582 PVD 16.7 17.7 0.679 Renal disease 12.7 12.5 0.728 Renal failure 9.4 9.3 0.884 Tobacco use 28.309 29.982 0.255ETOH = alcohol use disorder, HTN = hypertension, PVD = peripheral vascular disease
ARF = acute renal failure, CI = confidence interval, DVT = deep vein thrombosis, MI = myocardial infarction, OR = odds ratio, PE = pulmonary embolism, THA = total hip arthroplasty, UTI = urinary tract infection
Bold indicates statistical significance (p < 0.05)
Patients with scoliosis were also at increased 1-year risk of revision THA (OR, 1.31; 95% CI, 1.17 to 1.47; P < 0.001), PJI (OR, 1.16; 95% CI, 1.04 to 1.30; P = 0.0089), aseptic loosening (OR, 1.39; 95% CI, 1.21 to 1.60; P < 0.001), and dislocation (OR, 1.58; 95% CI, 1.47 to 1.70; P < 0.001) (Table 4). There was no notable difference between scoliosis and nonscoliotic patients for incidence of periprosthetic fracture and osteolysis.
Table 4 - One-Year Surgery-Related Complications After Total Hip Arthroplasty in Scoliosis and Control Cohorts Complication Scoliosis Control Statistical Analysis N % N % OR 95% CI P Revision 341 1.57 2,610 1.20 1.3113 1.1704-1.4693 <0.001 PJI 355 1.64 3,069 1.42 1.1593 1.0377-1.2951 0.0089 Periprosthetic fracture 202 0.93 1,914 0.88 1.0559 0.9128-1.2215 0.4643 Osteolysis 18 0.082 145 0.066 1.2416 0.7606-2.0267 0.3868 Loosening 222 1.02 1,602 0.73 1.3897 1.2069-1.6002 <0.001 Dislocation 809 3.82 5,187 2.42 1.581 1.4662-1.7049 <0.001PJI = periprosthetic joint infection, CI = confidence interval, OR = odds ratio, THA = total hip arthroplasty
Bold indicates statistical significance (p < 0.05)
The scoliosis cohort was associated with a significantly higher 90-day incidence of ED visit (OR, 1.26; 95% CI, 1.21 to 1.31; P < 0.001), readmission (OR, 1.78; 95% CI, 1.44 to 2.20; P < 0.001), and 1-year cost of care ($13,834.44 ± 14,293.27 versus $10,864.78 ± 17,283.90) (Table 5).
Table 5 - 90-Day Hospital Utilization After Total Hip Arthroplasty in Scoliosis and Control Cohorts Complication Scoliosis Control Statistical Analysis N % N % OR 95% CI P ED visit 3,290 17.60 26,920 13.95 1.2612 1.2127-1.3116 <0.001 Readmission 102 0.47 575 0.26 1.7775 1.4393-2.1952 <0.001 Reimbursement $13,834.44 ± 14,293.27 — $10,864.78 ± 17,283.90 — — — <0.001ED = emergency department, CI = confidence interval, OR = odds ratio
Bold indicates statistical significance (p < 0.05)
Scoliosis is a common spinal abnormality that classically manifests in the pediatric population as an abnormal curvature of the spine in the coronal plane. Although sagittal plane deformities have been heavily studied in the context of complications after THA, coronal plane deformities of the spine, such as scoliosis, have not been previously studied. Our findings suggest that even in the absence of a spinal fusion, patients with scoliosis were at increased risk of several medical complications, surgery-related complications, and healthcare utilization. These findings have important ramifications for the arthroplasty surgeon in the preoperative and perioperative periods when counseling patients with a history of scoliosis.
Patients with scoliosis were at increased risk of several 90-day medical complications, despite controlling for confounding variables such as comorbidities and demographics. Although there are no studies that examine the effect of scoliosis on orthopaedic procedures, a study that evaluated the incidence of medical complications after scoliotic corrective surgery found that infectious, neurologic, and cardiopulmonary complications were the most likely to occur.4 An increased risk of venous thromboembolism has been linked to scoliosis, according to other studies.5 Risk factors for increased rates of thromboembolism included worse sagittal deformity. It is also possible that patients with scoliosis are less likely to be adequately mobilized in the postoperative period after THA, although this is purely speculative and requires further prospective studies to validate. Scoliosis has also been linked to increased risk of cardiac and pulmonary complications, possibly due to decreased tidal volume and thoracic capacity of scoliotic patients.6
Scoliosis was also a risk factor for an increased risk of several surgery-related complications after THA, namely revision, PJI, aseptic loosening, and dislocation. A previous study has linked poor bone health to patients with idiopathic scoliosis, noting that these at-risk patients had lower bone mineral density at central skeletal sites such as the femoral neck and the lumbar spine, which may provide an explanation for an increased risk of aseptic loosening and revision in a scoliotic cohort of patients.7 Scoliosis is also associated with an increased risk of periprosthetic infection which may stem from poor nutrition in this cohort of patients.8,9 In addition, the literature on spine surgery and perispinal implant infections have demonstrated that scoliosis is an independent risk factor for perispinal implant infection, although it is unclear why this relationship exists. Nevertheless, future research is necessary to better characterize this important relationship between scoliosis and PJI.
A history of scoliosis was associated with an increased risk of dislocation after THA, a finding that is interesting especially when excluding patients who underwent fusion for scoliosis. Spinal fusion has long been considered a risk factor for increased risk of dislocation after THA because of a decrease in lumbo-pelvic motion and loss of normal pelvic tilt when standing and sitting.10 It is interesting that a predominantly coronal plane deformity, such as scoliosis, is still associated with an increased risk of dislocation even in the absence of fusion. A study that evaluated patients who underwent THA before lumbar fusion found that even the presence of lumbar spinal stenosis can negatively affect the longevity of arthroplasty implants.11 One etiology for an increased risk of dislocation in scoliotic patients may stem from increased stiffness and decreased range of motion in the coronal, axial, and sagittal planes. A study that evaluated 87 patients with adolescent idiopathic scoliosis determined that clinical range of motion tests in all three planes were decreased compared with a control cohort, although these analyzed movements were just of the spine.12 This increased stiffness may increase the risk of dislocation after THA. In addition, as pelvic incidence increases as a patient ages, worsening of a scoliotic curve has been associated with an additional increase in pelvic incidence, mainly due to an increase in sacral slope and maintained or slightly decreased pelvic tilt. This change to spinopelvic parameters may also increase risk of dislocation. Other studies have determined that a more progressed scoliotic curve is associated with changes to pelvic tilt to reduce energy expenditure and maintain an upright spine.13 This compensatory change in pelvic tilt likely limits anteversion out of a safe zone of acetabular anteversion, increasing the risk of dislocation. In addition, during any hip arthroplasty procedure, there is always a degree of unpredictability with positioning of the pelvis in space—this unpredictability is magnified with a scoliotic curve in the lateral decubitus position which may explain these findings. These findings are very important for the arthroplasty surgeon to consider, both in the preoperative period when counseling patients with scoliosis and in the immediate postoperative period when protecting their activity to avoid early dislocation.
Patients with a history of scoliosis were also associated with increased healthcare utilization after THA compared with control subjects. Unfortunately, there are no studies that have examined scoliosis as a risk factor for increased healthcare utilization after orthopaedic procedures. However, this finding is fairly unsurprising in light of the increased risk of medical and surgery-related complications of this at-risk cohort compared with control subjects. A previous study on patients who underwent posterior spinal fusion for scoliosis found that 9.7% of patients returned to the ED in the postoperative period for, mostly, an outpatient medical issue.14 In another study of patients with adolescent scoliosis who underwent spinal fusion, 1.6% of patients underwent early readmission and 3.3% underwent late readmission.15
This study does have its limitations. First, the use of any large-scale administrative insurance database is contingent on the accurate entry and coding of diagnoses, comorbidities, and procedures within the data. However, recent studies suggest that the incidence of inaccuracy in large databases is lower than 1%.16,17 Furthermore, ICD-9 and 10 diagnosis codes do not reflect the severity of scoliosis or each patient's radiographic Cobb angle, and therefore, we cannot comment directly on the severity of scoliosis and how it affects postoperative medical and arthroplasty-related complications. The Mariner data set does not include specific coding for mortality data, and therefore, that data were notably absent from our analysis. Finally, although we excluded spinal fusion, we did not stratify patients based on other modalities of treatment including conservative modalities which may influence our findings.
References 1. Mac-Thiong JM, Labelle H, Charlebois M, Huot MP, de Guise JA: Sagittal plane analysis of the spine and pelvis in adolescent idiopathic scoliosis according to the coronal curve type. Spine (Phila Pa 1976) 2003;28:1404-1409. 2. Labelle H, Aubin CE, Jackson R, Lenke L, Newton P, Parent S: Seeing the spine in 3D: How will it change what we do? J Pediatr Orthop 2011;31:S37-S45. 3. Stokes IA: Three-dimensional terminology of spinal deformity. A report presented to the scoliosis research society by the scoliosis research society working group on 3-D terminology of spinal deformity. Spine (Phila Pa 1976) 1994;19:236-248. 4. Zhang XN, Sun XY, Hai Y, Meng XL, Wang YS: Incidence and risk factors for multiple medical complications in adult degenerative scoliosis long-level fusion. J Clin Neurosci 2018;54:14-19. 5. Kim HJ, Iyer S, Diebo BG, et al.: Clinically significant thromboembolic disease in adult spinal deformity surgery: Incidence and risk factors in 737 patients. Glob Spine J 2018;8:224-230. 6. Godfrey S: Respiratory and cardiovascular consequences of scoliosis. RES 1970;27(suppl 1):67-70. 7. Diarbakerli E, Savvides P, Wihlborg A, Abbott A, Bergström I, Gerdhem P: Bone health in adolescents with idiopathic scoliosis. Bone Joint J 2020;102-B:268-272. 8. Aleissa S, Parsons D, Grant J, Harder J, Howard J: Deep wound infection following pediatric scoliosis surgery: Incidence and analysis of risk factors. Can J Surg 2011;54:263-269. 9. Jevsevar DS, Karlin LI: The relationship between preoperative nutritional status and complications after an operation for scoliosis in patients who have cerebral palsy. J Bone Joint Surg Am 1993;75:880-884. 10. Buckland AJ, Puvanesarajah V, Vigdorchik J, et al.: Dislocation of a primary total hip arthroplasty is more common in patients with a lumbar spinal fusion. Bone Joint J 2017;99-B:585-591. 11. Di Martino A, Bordini B, Geraci G, et al.: Impact of previous lumbar spine surgery on total hip arthroplasty and vice versa: How long should we be concerned about mechanical failure? Eur Spine J 2023;32:2949-2958. 12. Eyvazov K, Samartzis D, Cheung JPY: The association of lumbar curve magnitude and spinal range of motion in adolescent idiopathic scoliosis: A cross-sectional study. BMC Musculoskelet Disord 2017;18:51. 13. Guo J, Liu Z, Lv F, et al.: Pelvic tilt and trunk inclination: New predictive factors in curve progression during the Milwaukee bracing for adolescent idiopathic scoliosis. Eur Spine J 2012;21:2050-2058. 14. Harris AB, Marrache M, Puvanesarajah V, et al.: Emergency department visits after posterior spinal fusion for adolescent idiopathic scoliosis. J Pediatr Orthop 2020;40:e629-e633. 15. Patel A, Pahys JM, Samdani AF, et al.: Early and late hospital readmissions in adolescent idiopathic scoliosis. Spine Deform 2021;9:1041-1048. 16. Khan NF, Harrison SE, Rose PW: Validity of diagnostic coding within the general practice research database: A systematic review. Br J Gen Pract 2010;60:e128-e136. 17. Burns EM, Rigby E, Mamidanna R, et al.: Systematic review of discharge coding accuracy. J Public Health (Oxf) 2012;34:138-148.
Comments (0)