
Remember me




Patients self-discharging against medical advice (AMA) occurs when patients refuse continued care.1 Roughly 1% to 2% of hospitalized patients leave AMA.1,2 Patients who leave AMA have a higher risk of hospital readmission, morbidity, and mortality than discharged patients.2 Previous studies have identified that younger, male, and low socioeconomic status (SES) patients are more likely to leave AMA.2,3 Patients who leave AMA represent a public health and financial concern because they are more likely to experience adverse outcomes and to use additional healthcare resources in the future.4
The upper extremity (UE) function is critical in patients' quality of life.5 A study by de Putter et al6 found that patients with UE arm injuries had lower health-related quality of life (HRQoL) factors such as mobility and self-care. In addition, they also found that the HRQoL for hospitalized UE patients was far below that of the general population. In a retrospective cohort study by MacDermid et al7 of 266,324 patients with UE fractures in Ontario, 7.6% of the fractures were associated with hospital admission. Many UE orthopaedic injuries require hospitalization, including trauma-related UE amputations, mangled UEs, and multiple UE fractures.7–9 However, the factors that contribute to higher rates of UE orthopaedic patients leaving AMA have not been well categorized.
Many studies have been done to further understand the factors associated with patients who leave AMA in a general hospital setting. Our goal was to investigate this specific population because there are limited studies that have analyzed the demographics and risk factors of UE orthopaedic patients who leave AMA to our knowledge. 4 It is important to understand these factors because UE orthopaedic patients who leave AMA tend to have decreased HRQoL and cause economic burden to healthcare systems. It is our hope that by understanding the factors contributing to higher rates of patients leaving AMA, we can develop solutions to improve patient adherence to medical advice. We hypothesize that hospitalized UE orthopaedic patients will have similar demographics and risk factors of those in a general hospital setting that leave AMA. We hypothesize that younger patients, male, of racial minority groups, have lower SES, and lack health insurance, are more likely to leave AMA.
MethodsWe conducted a retrospective analysis of the Healthcare Cost and Utilization Project database, sourced from federal, state, and industry levels from community and academic hospitals between 2011 and 2020. We specifically reviewed UE trauma assessing CPT codes S42 (fracture of shoulder and upper arm), S52 (fracture of forearm), and S62 (fracture at wrist and hand level). This database is generated each year by randomly sampling 20% of all included patient data. Variables that include age, sex, household income by quartile, concurrent diagnoses, insurance payer type, rural or urban practice setting, length of stay, recovery time, days from admission to the procedure, and the total charge for a visit were collected.
We compared the relationship between the collected variables and rates of leaving AMA. Multiple logistic regression models that were created from the variables found to have a notable relationship. Independent sample t-tests were conducted for normally distributed data, and the Wilcoxon rank-sum test was used for nonnormally distributed data. Categorical variables were analyzed with the Chi-square with Kendall tau or Fischer exact test. Residuals were assessed for normal distribution where appropriate, and no multicollinearity was observed. Categorical data are reported as n (%), and continuous data are reported as mean (standard deviation). The standard error is reported when appropriate.
ResultsWe identified 262,912 patients who satisfied the inclusion criteria. 261,739 (99.55%) were discharged without leaving AMA, while 1,173 (0.45%) left AMA. 91.98% of all patients received care in an urban setting, while 8.02% received care in a rural setting.
Demographic FactorsThe mean age of all patients in this study was 62.46 years. Patients who left AMA were significantly younger than patients who did not leave AMA (43.69 versus 62.55, P < 0.001). Men were more likely than women to leave AMA (69.05% versus 30.95%, P < 0.001), and Black patients were more likely to leave AMA than the general population (P < 0.001). Patients from the lowest income quartile were the most likely to leave AMA (OR, 1.657, P < 0.001), and patients from the highest income quartile were the least likely to leave AMA (OR, 0.579, P < 0.001). Household income levels indicated that most patients who left AMA tend to come from the lowest income quartile (0 to 25th percentile, n = 443, 40.27%) compared with the highest income percentiles (75th to 100th percentile, n = 143, 13%). Patients on Medicaid (38.61% versus 7.81%, P < 0.001) or who had no insurance (2.14% versus 0.34%, P < 0.001) were more likely to leave AMA than the rest of the population. Patients with private insurance (25.30% versus 10.96%, P < 0.001) or with Medicare (56.47% versus 20.72%, P < 0.001) were more likely to have normal discharge than the general population. This information is summarized in Table 1.
Table 1 - Demographic Factors Associated With Leaving AMA Factor No AMA AMA Total P Total number, N (%) 261,739 (99.55) 1,173 (0.45) 262,912 Demographics Age Mean (SD) 62.545 (18.198) 43.687 (16.374) 62.461 (18.234) <0.001 Age category <30 21,570 (8.24) 258 (21.99) 21,828 (8.30) <0.001 30-54 26,327 (10.06) 513 (43.73) 26,840 (10.21) 55-64 63,802 (24.38) 257 (21.91) 64,059 (24.37) ≥65 149,983 (57.31) 145 (12.36) 150,128 (57.11) Sex Female 140,148 (53.57) 363 (30.95) 140,511 (53.47) <0.001 Male 121,460 (46.43) 810 (69.05) 122,270 (46.53) Race Asian or pacific islander 2,853 (1.15) 12 (1.06) 2,865 (1.15) <0.001 Black 16,856 (6.78) 199 (17.55) 17,055 (6.83) Hispanic 19,763 (7.95) 152 (13.40) 19,915 (7.98) Other 6,988 (2.81) 39 (3.44) 7,027 (2.81) White 202,086 (81.31) 732 (64.55) 202,818 (81.23) Household income by zip code 0 to 25th percentile 64,228 (24.97) 443 (40.27) 64,671 (25.04) <0.001 26th to 50th percentile 69,238 (26.92) 295 (26.82) 69,533 (26.92) 51st to 75th percentile 67,592 (26.28) 219 (19.91) 67,811 (26.25) 76th to 100th percentile 56,139 (21.83) 143 (13.00) 56,282 (21.79) Rural/urban Rural 20,938 (8.04) 37 (3.32) 20,975 (8.02) <0.001 Urban 239,578 (91.96) 1,079 (96.68) 240,657 (91.98) Payer Medicaid 20,401 (7.81) 451 (38.61) 20,852 (7.94) <0.001 Medicare 147,601 (56.47) 242 (20.72) 147,843 (56.32) No charge 886 (0.34) 25 (2.14) 911 (0.35) Other 15,978 (6.11) 56 (4.79) 16,034 (6.11) Private insurance 66,126 (25.30) 128 (10.96) 66,254 (25.24) Self-pay 10,366 (3.97) 266 (22.77) 10,632 (4.05)AMA = Against Medical Advice
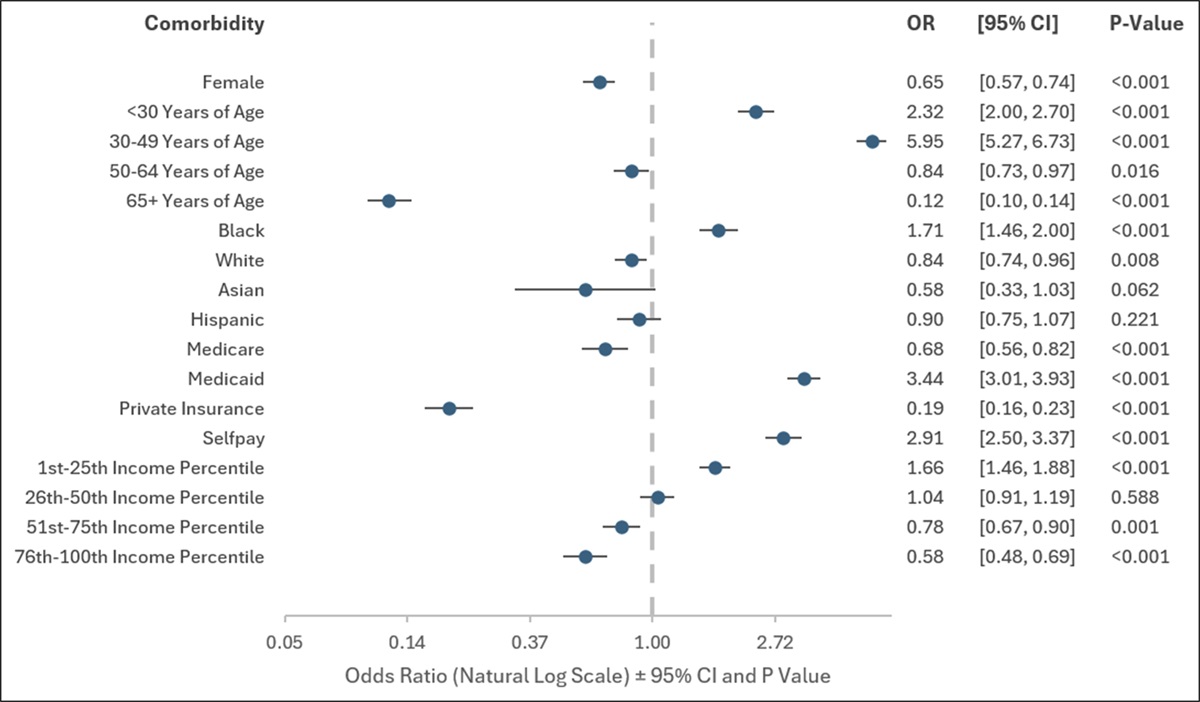
Female patients were 0.647 times as likely as male patients to leave AMA (P < 0.001). In addition, patients younger than 30 years were 2.324 times more likely to leave AMA (P < 0.001), and patients aged between 30 and 49 years were 5.953 times more likely to leave AMA (P < 0.001). However, patients aged between 50 and 64 years were 0.841 times less likely to leave AMA (P < 0.016), and patients aged older than 65 years were 0.117 times less likely to leave AMA (P < 0.001). Black patients were 1.708 times more likely to leave AMA compared with patients of different racial backgrounds (P < 0.001), while White patients were 0.840 times less likely to leave AMA (P < 0.001). Although our study shows that Asian (OR, 0.580, P < 0.062) and Hispanic (OR, 0.896, P < 0.221) patients were less likely to leave AMA, the data were not statistically significant. Patients with Medicaid were 3.436 times more likely to leave AMA than patients with other type of insurance (P < 0.001), and patients with private health insurance were 0.191 times less likely to leave AMA (P < 0.001). Patients in the bottom quartile of income were 1.657 times more likely to leave AMA than other patients (P < 0.001), and patients in the top quartile of income were 0.579 times less likely to leave AMA compared with non-AMA patients (P < 0.001). These data are presented in Figure 1.
 Figure 1:
Figure 1: Graph showing odds ratios of each demographic factor and patients leaving AMA.
Hospital Course VariablesPatients who left AMA had longer average days from admission to procedure (0.896 versus 0.383 days, P < 0.001), longer lengths of stays at the hospital (3.626 versus 2.363 days, P < 0.001), and longer recovery times (2.733 versus 1.977 days, P < 0.001) than patients who did not leave AMA. In addition, patients who left AMA had a lower total charge of hospital stay compared with non-AMA patients ($57,627.24 versus $65,993.79, P < 0.001). These data are presented in Table 2.
Table 2 - Hospital Course Factors Associated With Leaving AMA Hospital Course Variables No AMA AMA Total P Days from admission to procedure (d) Mean (SD) 0.382 (1.343) 0.896 (1.556) 0.384 (1.345) <0.001 Length of stay (d) Mean (SD) 2.363 (2.573) 3.626 (4.447) 2.369 (2.586) <0.001 Time recovery (d) Mean (SD) 1.977 (2.162) 2.733 (3.780) 1.980 (2.172) <0.001 Total charge ($) Mean (SD) 65,993.791 (48,122.789) 57,627.242 (54,622.040) 65,956.363 (48,156.934) <0.001 Discharge disposition Adverse discharge 34,984 (13.37) 1,173 (100.00) 36,157 (13.75) <0.001 Home discharge with care 42,145 (16.10) 42,145 (16.03) Routine discharge 184,610 (70.53) 184,610 (70.22)AMA = Against Medical Advice
Our retrospective analysis of 262,912 patients found that in UE adult orthopaedic patients, 0.45% left AMA. Patients more likely to leave AMA were male, younger than 50 years, Black, on Medicaid, and came from zip codes with a median income in the bottom quartile.
It has been established in the literature that Black and male patients leave AMA more frequently across many fields of medicine. Moy et al10 retrospectively reviewed 241,911 patients in a general hospital setting and found that African American patients were 1.78 times more likely than White patients to leave AMA, a finding replicated in our study. They also found that men and patients with either state or no insurance were more likely to leave AMA.10 Some of this effect may be explained by SES factors.11 African Americans are less likely to have health insurance than the general population, and one in four surveys reported problems paying medical bills.12 However, our study found that when controlling for sex, age, insurance status, and income, Black patients were still more likely to leave AMA than patients from other racial backgrounds after UE orthopaedic injuries. Although these SES factors may explain some of these differences, other variables are likely mediating this effect.
Another potential reason Black patients may leave AMA more frequently than the rest of the population is a lower level of trust in healthcare providers, leading to lower patient satisfaction.13 Patient trust has been associated with higher patient satisfaction and treatment adherence.13,14 Strong interpersonal communication between patients and clinicians is essential to bring high-quality care.13,15 African Americans and other minority patients have been found to receive poorer interpersonal communication, which can lead to greater physician verbal dominance, shorter visits, and less patient-centeredness compared with White patients.13 Effective communication and empathy are linked to increased patient satisfaction, better adherence to treatment, and improved health outcomes.15 Addressing these issues may be done through perspective-taking, a technique that improves a patient's ability to communicate their perspective to a doctor through directed questions. This intervention has been demonstrated to improve short-term communication and trust with patients. It can potentially improve treatment adherence and patient satisfaction and reduce the rate of Black patients leaving AMA.16 However, additional studies must be done to understand better what interventions can be instated to improve trust in medical professionals and to determine what other factors may contribute to Black patients leaving AMA more frequently than their counterparts.
Several studies have investigated the factors contributing to patients leaving AMA after trauma. Haines et al17 found that after trauma, African American and uninsured patients were more likely to leave AMA than other patients in their retrospective study of 1,770,570 patients from the National Trauma Bank, which collects data from the United States, Puerto Rico, and Canada. Kraut et al18 conducted a retrospective review of 1,916,104 Canadian patients from the Manitoba Centre for Health Policy and found that patients who left AMA were more likely to be male, of low SES, have a history of drug abuse, and have a history of HIV/AIDS. One potential reason for patients leaving AMA is the cost of health care. Our study found that patients in the lowest household income quartile were more likely to leave AMA after an UE orthopaedic injury. In addition, our study found that patients without health insurance are more likely to leave AMA than patients with health insurance. Although safety nets such as universal health care may seem to address this issue, evidence suggests that this is not an ideal solution. Kraut et al18 followed a trauma population with universal health care provided by the government. Their population had a higher rate of patients leaving AMA than the population in our study (1.4% versus 0.45%). Haines et al17 also followed a cohort that included Canadian patients, and they also found that patients left more frequently than we did in our study (1.11% versus 0.45%). Despite these differences in rates of patients leaving AMA, our study specifically examines UE orthopaedic patients. By contrast, Kraut et al. and Haines et al. examined general trauma patients at acute care facilities.17,18 Additional studies must be conducted to determine why lacking health insurance leads to higher rates of patients leaving AMA.
Our study additionally found that patients who left AMA had a markedly longer time between procedure and admission. Although intuitive that patients who are in the hospital for longer before their procedure are more likely to leave AMA, this has not been previously investigated in the literature. From our experience, this relationship may be partially explained by patients feeling like their care is not progressing, but this has not been investigated in the literature. Additional studies must be conducted to determine what potential causes of this relationship may be. A potential explanation of lower rates of patients leaving AMA in our study compared with other trauma patients could be that UE patients tend to have lower lengths of stay (mean of 4.6 days for men and 6.6 days for women) compared with other trauma patients (mean of 9.4 days).
This is one of the first studies done to assess the demographics and risk factors that contribute to higher rates of adult hospitalized UE orthopaedic patients leaving AMA. We wanted to study UE orthopaedic patients because of the importance in the functionality of the UE's in maintaining one's quality of life. We hope that future healthcare policies can be developed that contribute to decreasing rates of leaving AMA in UE orthopaedic patients. In addition, we also believe that improving AMA rates can lead to cost savings to healthcare systems.
This study is limited by its retrospective design. Limitations to our study include confounding variables, incomplete data, recall bias, no randomization, no blinding, and potential restrictions to important patient information. However, the retrospective nature of this study enabled us to analyze a large number of patients to find relationships between variables that might not otherwise have been identified. In addition, this study is only conducted in patients within the United States who underwent treatment for UE orthopaedic injuries. Therefore, the factors that may influence these patients to leave may differ from other patient groups. However, for orthopaedic surgeons who frequently see UE injuries, it is critical to identify and address any factors that may lead to patients leaving AMA and increasing the likelihood that they have adverse outcomes. Furthermore, this study did not analyze patient substance use or provide detailed information about the clinical course. However, given the identified relationship between substance use and patient outcomes, this may explain some of our identified relationships.
ConclusionIn our retrospective analysis of the Healthcare Cost and Utilization Project database, we found that patients who are male, Black, younger than 49 years, have Medicaid, or are in the lowest income quartile are more likely to leave AMA after treatment for an UE orthopaedic injury than their counterparts. Therefore, surgeons must be aware of these risk factors to mitigate rates of leaving AMA. Some interventions that can increase patient adherence to medical advice include improving communication with patients and improving access to insurance. However, additional studies must be conducted to understand best practices and policies to increase patient adherence to medical advice. Additional studies must be conducted to understand why these factors are associated with higher rates of patients leaving AMA.
References 1. Spooner KK, Salemi JL, Salihu HM, Zoorob RJ: Discharge against medical advice in the United States, 2002-2011. Mayo Clin Proc 2017;92:525-535. 2. Holmes EG, Cooley BS, Fleisch SB, Rosenstein DL: Against medical advice discharge: A narrative review and recommendations for a systematic approach. Am J Med 2021;134:721-726. 3. Southern WN, Nahvi S, Arnsten JH: Increased risk of mortality and readmission among patients discharged against medical advice. Am J Med 2012;125:594-602. 4. Menendez ME, van Dijk CN, Ring D: Who leaves the hospital against medical advice in the orthopaedic setting? Clin Orthop 2015;473:1140-1149. 5. Van Lieshout ECC, van de Port IG, Dijkhuizen RM, Visser-Meily JMA: Does upper limb strength play a prominent role in health-related quality of life in stroke patients discharged from inpatient rehabilitation? Top Stroke Rehabil 2020;27:525-533. 6. de Putter CE, Selles RW, Haagsma JA, et al.: Health-related quality of life after upper extremity injuries and predictors for suboptimal outcome. Injury 2014;45:1752-1758. 7. MacDermid JC, McClure JA, Richard L, Faber KJ, Jaglal S: Fracture profiles of a 4-year cohort of 266,324 first incident upper extremity fractures from population health data in Ontario. BMC Musculoskelet Disord 2021;22:996. 8. Inkellis E, Low EE, Langhammer C, Morshed S: Incidence and characterization of major upper-extremity amputations in the national trauma data bank. JB JS Open Access 2018;3:e0038. 9. Bumbasirevic M, Stevanovic M, Lesic A, Atkinson HDE: Current management of the mangled upper extremity. Int Orthop 2012;36:2189-2195. 10. Moy E, Bartman BA: Race and hospital discharge against medical advice. J Natl Med Assoc 1996;88:658-660. 11. Franks P, Meldrum S, Fiscella K: Discharges against medical advice: Are race/ethnicity predictors? J Gen Intern Med 2006;21:955-960. 12. Becker G, Newsom E: Socioeconomic status and dissatisfaction with health care among chronically ill African Americans. Am J Public Health 2003;93:742. 13. Martin KD, Roter DL, Beach MC, Carson KA, Cooper LA: Physician communication behaviors and trust among black and white patients with hypertension. Med Care 2013;51:151-157. 14. Goldman LE, Vittinghoff E, Dudley RA: Quality of care in hospitals with a high percent of Medicaid patients. Med Care 2007;45:579-583. 15. Blatt B, LeLacheur SF, Galinsky AD, Simmens SJ, Greenberg L: Does perspective-taking increase patient satisfaction in medical encounters? Acad Med 2010;85:1445-1452. 16. Kong L, Chen Y, Wang L, Wang K, Liu C, Gan Y: Effect of perspective-taking on trust between doctors and patients: A randomized controlled trial. J Clin Psychol Med Settings 2023;30:708-715. 17. Haines K, Freeman J, Vastaas C, et al.: “I'm leaving”: Factors that impact against medical advice disposition post-trauma. J Emerg Med 2020;58:691-697. 18. Kraut A, Fransoo R, Olafson K, Ramsey CD, Yogendran M, Garland A: A population-based analysis of leaving the hospital against medical advice: Incidence and associated variables. BMC Health Serv Res 2013;13:415.
Comments (0)