
Remember me




Carpal tunnel syndrome (CTS) is a common upper extremity entrapment neuropathy and is estimated to affect 3.8% of the general population.1 While conservative management with splinting and/or steroid injection is typically considered,2,3 patients with ongoing symptoms may be considered for carpal tunnel release (CTR) with median nerve decompression4 by open (open carpal tunnel release [OCTR]) or endoscopic (endoscopic carpal tunnel release [ECTR]) approaches.
The standard approach for CTS is OCTR, which has been associated with very favorable outcomes.3,567 Roughly three decades ago, ECTR was introduced and can be performed by single-portal or two-portal methods.8,9 Although ECTR and OCTR are generally considered safe procedures, neurovascular and other surgical complications can occur.10 Previous research has demonstrated that ECTR can lead to comparable outcomes compared with OCTR.
While outcomes after both ECTR and OCTR have been compared, the relative utilization of these two techniques is not fully clear, especially in more recent years. One older 2004-2014 study examined trends in OCTR versus ECTR use from California, Florida, and New Jersey and found the following: the incidence of ECTR was increasing, those undergoing OCTR were associated with greater comorbidity burden, and ECTR was found to be markedly more costly.11 Another older 2005-2014 study used a national database and found that the incidence of both ECTR and OCTR was increasing over their study period.12
This study was designed to follow up on previous trend analysis of the endoscopic technique relative to OCTRs using a large, national, multi-insurance, administrative database. The study also aimed to assess predictive factors for utilization of each of the approaches, overall reimbursement, and concomitant procedures performed on the same day as CTR. We hypothesized increasing utilization of ECTR relative to OCTR over the years of study.
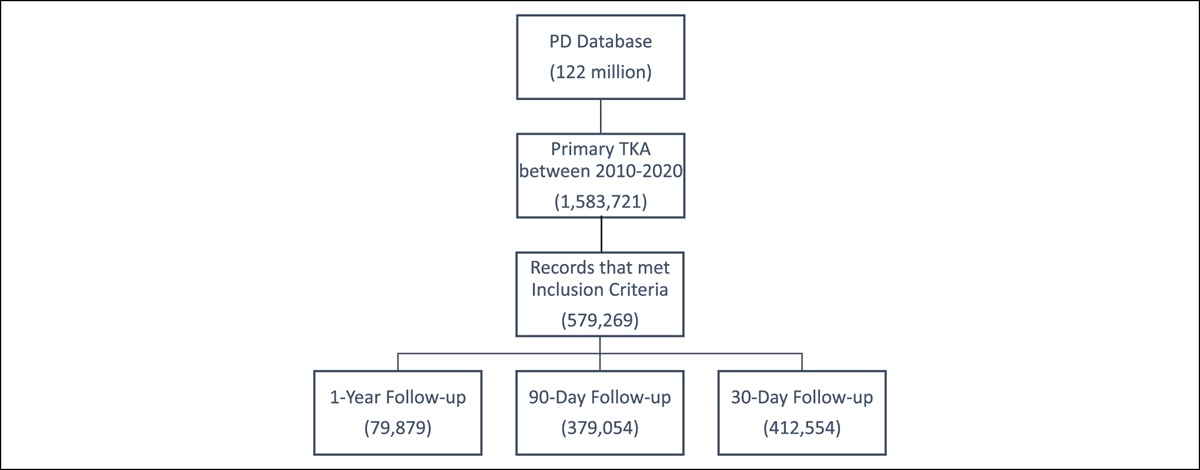
Methods Database and CohortData analyzed in this retrospective cohort study were abstracted from the 2010-2021 PearlDiver M151Ortho data set. This is a large, Health Insurance Portability and Accountability Act–compliant administrative database containing information of nearly 151 million patients in the United States. Our institutional review board designated studies using this data set exemption from review.
Patients for this study were identified using Current Procedural Terminology (CPT) coding. ECTR was identified with CPT-29848 while OCTR was identified with CPT-64721. Patients who had any diagnosis related to trauma, neoplasm, or infection on the day of CTR were excluded from the study cohort based on the presence of pertinent ICD diagnosis codes on the same day as ECTR or OCTR.
In addition to tracking the year that each surgery type was performed, several patient demographic factors were extracted. These included age, sex, Elixhauser Comorbidity Index (ECI, a standardized patient comorbidity index generated using longitudinal International Classifications of Disease codes), region of the country where the surgery was performed (Northeast, Midwest, South, and West), and insurance plan (commercial, Medicaid, Medicare).
Subsequent Surgeries and Overall ReimbursementsThe average day-of-surgery and overall 90-day reimbursements for ECTR and OCTR procedures were determined. This included all reimbursements over the indicated period—defined as total reimbursement paid by patients' insurance provider. Institutional-level costs associated with ECTR and OCTR could not be determined using the PearlDiver data set.
Concomitant procedures performed on the same day as ECTR and OCTR were determined by extracting all additional procedural codes billed for on the same day as CTR. Codes were then manually grouped into procedure categories, including cubital tunnel release, trigger finger release, intercarpal or carpometacarpal (CMC) arthroplasty, ganglion cyst excision, extensor tendon sheath release, tendon transfer/repair/realignment, and distal radius/distal ulna arthroplasty. The number of patients who had these procedures performed on the same day as CTR was then determined.
Data AnalysisThe yearly utilization of ECTR relative to OCTR was tracked from 2010 to April 30, 2021. The projected total number of ECTRs performed by the end of 2021 was estimated using the number of ECTRs performed from January 1 through April 30, 2021. A Z-test for two proportions was used to statistically evaluate the proportional utilization of ECTR between years.
Univariate analysis was conducted to compare demographic factors of ECTR and OCTR patients identified. The Welch Student t-test was used to evaluate differences in age and ECI between the two groups while the Pearson chi-square test was used to evaluate for differences in patient sex, insurance plan, and region of the country where the surgery was performed.
Multivariate logistic regression analysis was conducted to identify independent predictors of having ECTR performed as opposed to OCTR. With this, odds ratios (ORs) and 90% confidence intervals (95% CIs) were determined for each demographic factor analyzed and compared with their respective referent categories.
All statistical analyses were conducted within the built-in PearlDiver statistics package. Statistical significance was reached at P < 0.01. Prim9 (GraphPad Software) and Microsoft Excel (Microsoft Corporation) were used to create all figures.
Results Study CohortA total of 261,315 ECTR and 1,133,998 OCTR patients were initially identified in the data set; however, after application of inclusion/exclusion criteria, 258,345 ECTR and 1,015,526 OCTR patients were identified. In total, 441,023 ECTR procedures and 1,767,820 OCTR procedures were identified over the study interval, of which 258,345 (58.6%) and 1,015,526 (57.4%) were primary procedures, respectively. The number of each type of surgery was assessed by year. The total number of carpal tunnel releases performed annually increased from 183,260 in 2010 to a projected 198,927 in 2021, reflecting an 8.5% increase. Endoscopic cases were noted to evolve from 2010 (28,859 cases, 15.7% of all carpal tunnel releases performed in 2010) through 2021 (32,007 cases, 26.1% of all carpal tunnel releases performed in 2021) (Figures 1 and 2). This increase in ECTR was significant over the years of studies (P < 0.001).
 Figure 1:
Figure 1: Chart demonstrating the annual utilization of endoscopic carpal tunnel release (ECTR) from 2010 to 2021. For year 2021, black bar represents ECTRs performed through April 30, 2021, while the dashed bar represents the projected remaining number of ECTRs to be performed by the end of 2021.
 Figure 2:
Figure 2: Chart demonstrating the proportional utilization of single-level endoscopic carpal tunnel release (ECTR) compared with open carpal tunnel release (OCTR) from 2010 to 2021. Black bars represent ECTR while gray bars depict OCTR. Numbers above black bars reveal the percentage of procedures each year that were ECTR. The increase in proportional utilization of ECTR between 2010 (15.8%) and 2021 (25.7%) was statistically significant (P < 0.0001).
Factors Associated With Receiving Endoscopic Carpal Tunnel ReleaseDemographic factors of patients who underwent OCTR or ECTR are listed in Table 1. Compared with OCTR patients, ECTR patients were, on average, younger (average age 57.88 versus 58.01 for OCTR), more female predominant (64.5% versus 63.7%), less comorbid (average ECI 2.84 versus 3.73), and more frequently commercially insured (73.7% versus 70.9%) (P < 0.0001 for each). In addition, regional variations were observed, with the largest proportion of ECTRs being performed in the Northeast (41.1%), whereas the largest proportion of OCTRs was performed in the South (35.2%) (P < 0.001).
Table 1 - Univariate Analysis of Characteristics of Patients With Open and Endoscopic Carpal Tunnel Releases From 2010 to 2021 Factor Open Endoscopic P N 1,015,526 (79.7%) 258,345 (20.3%) Age (mean ± SD) 58.01 ± 13.6 57.88 ± 13.50 <0.0001 Sex Female 647,322 (63.7%) 166,575 (64.5%) <0.0001 Male 368,204 (36.3%) 91,770 (35.5%) ECIa (mean ± SD) 3.73 ± 3.2 2.84 ± 2.67 0-1 286,163 (28.2%) 7302 (37.8%) <0.0001 2-3 286,450 (28.2%) 5979 (31%) 4-5 198,654 (19.6%) 3243 (16.8%) >5 244,259 (24.1%) 2777 (14.4%) Region Midwest 328,999 (32.4%) 59,502 (23%) <0.0001 Northeast 194,886 (19.2%) 53,639 (20.8%) West 130,723 (12.9%) 37,661 (14.6%) South 357,133 (35.2%) 106,244 (41.1%) Insurance Commercial 719,865 (70.9%) 190,441 (73.7%) <0.0001 Medicare 204,883 (20.2%) 49,855 (19.3%) Medicaid 66,386 (6.5%) 12,309 (4.8%)aECI = Elixhauser Comorbidity Index.
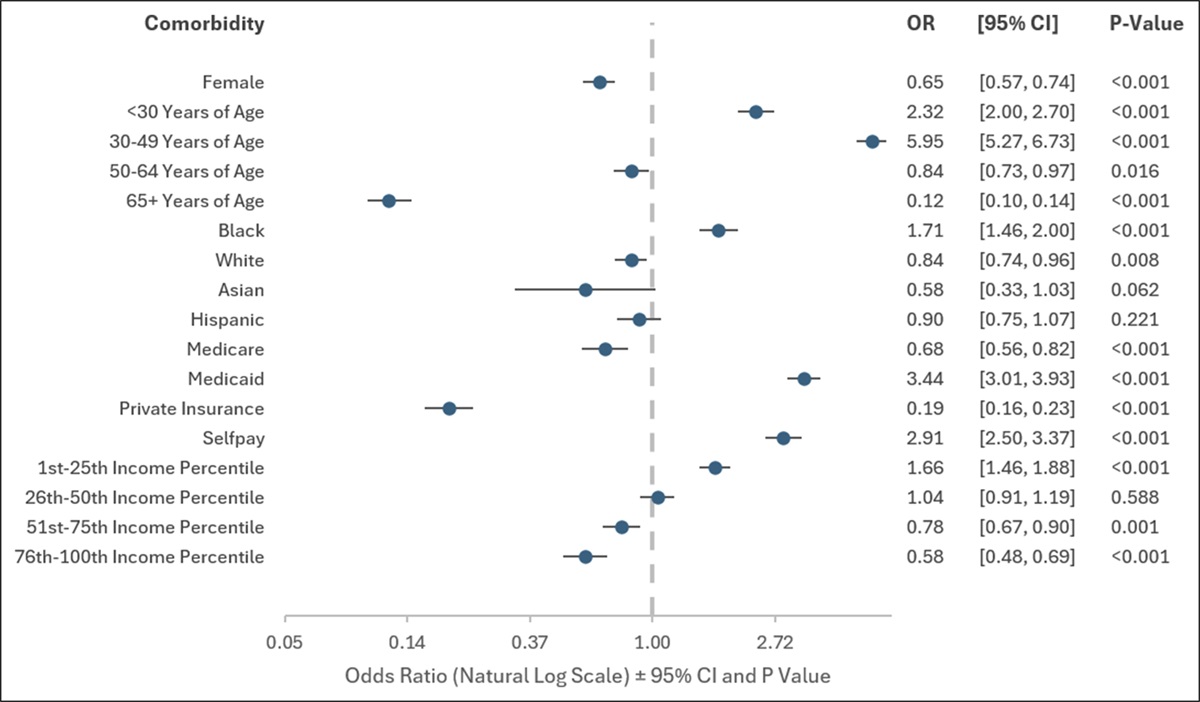
Multivariate analysis of independent predictors for having ECTR performed rather than OCTR is provided in Table 2. ECTR was more common in those who were younger (OR per decade decrease 1.01), female (OR, 1.04), and more highly comorbid (per two-point increase in ECI, OR, 1.02) or who had surgery outside the Midwestern United States (Northwest OR, 1.53; West OR, 1.62; and South OR, 1.66) (P < 0.0001 for all). By contrast, patients with Medicare or Medicaid insurance were significantly less likely to receive ECTR than OCTR when compared with those with commercial insurance (Medicare OR 0.94 and Medicaid 0.69, respectively) (P < 0.0001 for both).
Table 2 - Multivariate Analysis of Predictive Factors for Undergoing Endoscopic Carpal Tunnel Release Rather Than Open Carpal Tunnel Release N = 1,257,356 OR (95% CI) P Age (per decade decrease) 1.01 (1.00, 1.01) <0.0001 Sex Male (referent) Female 1.04 (1.03, 1.05) <0.0001 ECI (per two-point decrease) 1.02 (1.01, 1.02) <0.0001 Region Midwest (referent) Northeast 1.53 (1.53, 1.53) <0.0001 West 1.62 (1.61, 1.62) <0.0001 South 1.66 (1.64, 1.68) <0.0001 Insurance Commercial (referent) Medicare 0.94 (0.93, 0.95) <0.0001 Medicaid 0.69 (0.68, 0.70) <0.000195% CI = 95% confidence interval, ECI = Elixhauser Comorbidity Index, OR = odds ratio.
Day-of-surgery and 90-day average reimbursements for OCTR and ECTR are provided in Table 3. The average (SD) day-of-surgery reimbursement for ECTR was $1,265.38 ($1,652.47), compared with $1,122.45 ($2,903.51) for OCTR. By contrast, the overall 90-day reimbursement of ECTR was $3,114.82 ($5,418.05), and that of OCTR was $3,087.62 ($7,417.61). Two-mean T-tests revealed the day-of-surgery reimbursement for ECTR to be significantly greater than for OCTR (P < 0.0001); however, there was no significant difference in the average 90-day reimbursement between the two procedures (P = 0.0816).
Table 3 - Reimbursement of Open and Endoscopic Carpal Tunnel Releases From 2010 to 2021 Reimbursement Period Open (N = 1,004,384) Endoscopic (N = 256,205) P Day-of-surgery $1,122.45 ($2,903.51) $1,265.38 ($1,652.47) <0.0001 90 days postoperatively $3,087.62 ($7,417.61) $3,114.82 ($5,418.05) 0.0816Trends in reimbursement over time were also evaluated. The average (SD) day-of-surgery reimbursement for ECTR was $941.21 ($1,024.54) in 2010, increasing to $1,273.04 ($1,690.19) in 2020 (P < 0.0001). A similar trend was observed for OCTR, with day-of-surgery reimbursement being $838.65 ($1,501.28) in 2010 and $1,259.80 ($1,868.81) in 2020 (P < 0.0001). The average 90-day reimbursement for ECTR was $1,966.69 ($5,072.20) in 2010, increasing to $3,581.32 ($5,075.53) in 2020 (P < 0.0001), whereas the average 90-day reimbursement for OCTR was $2,018.09 ($5,583.89) in 2010, rising to $3,870.19 ($7,079.07) in 2020 (P < 0.0001).
Concomitant procedures performed on the same day as ECTR or OCTR are shown in Figure 3. Among both ECTR and OCTR patients, cubital tunnel release was the most performed additional procedure in 24,724 and 87,297 cases, respectively. This was followed by trigger finger release (21,470 ECTR, 72,864 OCTR), intercarpal or CMC arthroplasty (5,498 ECTR, 18,282 OCTR), ganglion cyst excision (4,594 ECTR, 17,092 OCTR), extensor tendon sheath release (4,724 ECTR, 12,284 OCTR), tendon transfer/repair/realignment (4,234 ECTR, 14,154 OCTR), and total wrist/distal radius/distal ulna arthroplasty (148 ECTR, 636 OCTR).
 Figure 3:
Figure 3: Chart demonstrating additional concomitant procedures performed on the same day as endoscopic carpal tunnel release (ECTR) or open carpal tunnel release (OCTR). Black bars represent the number of alterative procedures performed on the same day as ECTR while gray bars represent the number of alternative procedures performed on same day as OCTR.
DiscussionCTS affects 3.8% of the general population,1 and surgery with ECTR or OCTR may be considered if conservative measures do not provide adequate improvement.3,6,13,14 The relative utilization of ECTR versus OCTR has not been reported since 2014,12 and this study sought to assess utilization rates, predictors, and overall reimbursement in a large, national, multi-insurance cohort from 2010 through 2021.
For a very large study population of over a million carpal tunnel releases, 80.0% were by OCTR. Notably, this may represent a decline from previous years, with a previous 2005-2012 study reporting 88.1% of CTR surgeries as OCTR. Despite the growing popularity of ECTR, this finding emphasizes that most of the CTRs continue to be performed by open technique.3 Several reasons may underlie the greater use of OCTR versus ECTR, including the greater institution-level cost of endoscopic equipment, training bias for one procedure over the other, and potentially greater risk of iatrogenic nerve injury in ECTR.6
Over the years of this study, endoscopic cases increased from 15.7% of cases in 2010 to 26.1% of cases in 2021. This is put in the context of a previous study analyzing the Medicare population that reported a higher annual growth rate of ECTR (5%) compared with OCTR (0.9%) between 2005 and 2012.15 Another study also reported increasing utilization of ECTR relative to OCTR from 2003 to 2013.16 This study builds on these previous works, identifying a continuing trend toward ECTR in more recent years—particularly 2014 onward.
Multivariate analysis identified several patient factors as independent predictors of undergoing ECTR rather than OCTR, including age, sex, and comorbidity burden. Regarding patient age, both the present and past studies report that younger patients are more likely to undergo ECTR rather than OCTR.17 Regarding patient sex, previous work supports the findings of this study, with women being more likely to undergo ECTR.11 No study to date has evaluated the influence of patient comorbidity on undergoing ECTR versus OCTR. This study identified patients with lower comorbidity burdens to be independently more likely to receive ECTR rather than OCTR. Importantly, despite the statistical significance of these findings, ORs for patient-level factors as predictors for ECTR versus OCTR were quite small; thereby, the clinical significance of these findings is unclear.
By contrast, non–patient-level factors were found to greatly influence treatment modality choice. Notably, this study found geography of where the procedures were performed to be the greatest independent predictor of ECTR relative to OCTR. This aligns with a previous study showing regional differences15 and is interpreted to be differences in training because past studies have shown hand fellowship–trained surgeons to be 4.5 times more likely to perform ECTR compared with non–hand fellowship–trained surgeons.16 Past studies have explored the geographic distribution of hand fellowship–trained surgeons and training programs across the United States, finding notable variation in different regions of the country.18 Specifically, a greater density of hand fellowship–trained surgeons and fellowship programs are found in the Northeast and West compared with the South and Midwest. Such variations in hand fellowship–trained surgeon availability and the location of training programs likely influence the relative utilization of ECTR versus OCTR in different regions of the country.
This study also found Medicare and Medicaid patients to be independently less likely to undergo ECTR than commercially insured patients, a finding that has not been previously reported to our knowledge and may suggest some disparity in care. This finding may also reflect greater institution-level costs for ECTR relative to OCTR, with Medicaid and Medicare patients being directed toward less costly treatment options.11
Interestingly, day-of-surgery reimbursement for ECTR was markedly greater than that for OCTR; however, 90-day reimbursement rates between ECTR and OCTR showed no difference between the two procedures. Past studies have found ECTR to be a costlier procedure than OCTR at the institution level15,19; however, current literature also suggests that long-term institution-level costs of ECTR may be equal to or less than those of OCTR secondary to more favorable postoperative outcomes after ECTR.20 The equalization in reimbursement between ECTR and OCTR by 90 days postoperatively may reflect fewer postoperative adverse events for ECTR patients because of procedure-level factors or patient-level factors—such as ECTR patients being younger and having lower comorbidity burden as identified in this study. Furthermore, both day-of-surgery and 90-day reimbursement for ECTR and OCTR markedly increased over the duration of the study. This trend likely reflects rising healthcare costs, annual increasing relative value units for CTR, and inflation over the years.21,22 Importantly, rising reimbursement for CTR may not reflect a direct increase in payment to surgeons over the years.22
Finally, this study identified several procedures commonly performed concomitantly with CTR—the most common being cubital tunnel release, trigger finger release, and intercarpal or CMC arthroplasty. Past studies have demonstrated that additional procedures are commonly performed on the same day as CTR when multiple pathologies are present.23 Notably, there was minimal difference in the relative frequency of different alternative procedures performed between ECTR and OCTR.
This study has several limitations. As with all large administrative database studies, the accuracy of the findings is limited to the accuracy of the data coded. Furthermore, data were only available through April 30, 2021, with total ECTR utilization for 2021 calculated by extrapolation. In addition, although patient demographic factors could be analyzed, individual patient-level factors that could influence the decision to perform ECTR or OCTR could not be assessed. Furthermore, institution-level costs of ECTR and OCTR could not be assessed using the PearlDiver database. Although reimbursements of the two procedures were assessed, these may not reflect the costs incurred by individual facilities for conducting ECTR and OCTR.
Overall, using a large, national database, this study evaluated ECTR use compared with OCTR from 2010 to 2021. ECTR utilization increased from 15.8% of CTR procedures in 2010 to 25.7% in 2021. Factors predictive of undergoing ECTR rather than OCTR were defined, and reimbursements of the two procedures were not markedly different.
References 1. Atroshi I, Gummesson C, Johnsson R, Ornstein E, Ranstam J, Rosén I: Prevalence of carpal tunnel syndrome in a general population. JAMA 1999;282:153-158. 2. Bland JD: Treatment of carpal tunnel syndrome. Muscle Nerve 2007;36:167-171. 3. Petrover D, Richette P: Treatment of carpal tunnel syndrome: From ultrasonography to ultrasound guided carpal tunnel release. Joint Bone Spine 2018;85:545-552. 4. Verdugo RJ, Salinas RA, Castillo JL, Cea JG: Surgical versus non-surgical treatment for carpal tunnel syndrome. Cochrane Database Syst Rev 2008;2008:CD001552. 5. Boya H, Ozcan O, Özteki N HH: Long-term complications of open carpal tunnel release. Muscle Nerve 2008;38:1443-1446. 6. Kim PT, Lee HJ, Kim TG, Jeon IH: Current approaches for carpal tunnel syndrome. Clin Orthop Surg 2014;6:253-257. 7. Benson LS, Bare AA, Nagle DJ, Harder VS, Williams CS, Visotsky JL: Complications of endoscopic and open carpal tunnel release. Arthroscopy 2006;22:919-924.e9242, 924.e911-912. 8. Okutsu I, Ninomiya S, Takatori Y, Ugawa Y: Endoscopic management of carpal tunnel syndrome. Arthroscopy 1989;5:11-18. 9. Chow JC: Endoscopic release of the carpal ligament: A new technique for carpal tunnel syndrome. Arthroscopy 1989;5:19-24. 10. Palmer AK, Toivonen DA: Complications of endoscopic and open carpal tunnel release. J Hand Surg Am 1999;24:561-565. 11. Williamson ERC, Vasquez Montes D, Melamed E: Multistate comparison of cost, trends, and complications in open versus endoscopic carpal tunnel release. Hand (N Y) 2021;16:25-31. 12. Devana SK, Jensen AR, Yamaguchi KT, et al.: Trends and complications in open versus endoscopic carpal tunnel release in private payer and Medicare patient populations. Hand (N Y) 2019;14:455-461. 13. Hansen TB, Majeed HG: Endoscopic carpal tunnel release. Hand Clin 2014;30:47-53. 14. Li Y, Luo W, Wu G, Cui S, Zhang Z, Gu X: Open versus endoscopic carpal tunnel release: A systematic review and meta-analysis of randomized controlled trials. BMC Musculoskelet Disord 2020;21:272. 15. Law TY, Rosas S, Hubbard ZS, Chieng LO, Chim HW: Trends in open and endoscopic carpal tunnel release utilization in the Medicare patient population. J Surg Res 2017;214:9-13. 16. Smetana BS, Zhou X, Hurwitz S, Kamath GV, Patterson JM: Effects of hand fellowship training on rates of endoscopic and open carpal tunnel release. J Hand Surg Am 2016;41:e53-e58. 17. Hudson HT Jr, Moore R, Elver AA, Herrera FA: Are patient demographics and payor status associated with practice patterns in the surgical management of carpal tunnel syndrome? Hand (N Y) 2022;19:128-135. 18. Baron ED, Lutsky KF, Maltenfort M, Beredjiklian P: Geographic distribution of hand surgeons throughout the United States. J Hand Surg Am 2018;43:668-674. 19. Zhang S, Vora M, Harris AHS, Baker L, Curtin C, Kamal RN: Cost-minimization analysis of open and endoscopic carpal tunnel release. J Bone Joint Surg Am 2016;98:1970-1977. 20. Rogers MJ, Stephens AR, Yoo M, Nelson RE, Kazmers NH: Optimizing costs and outcomes for carpal tunnel release surgery: A cost-effectiveness analysis from societal and health-care system perspectives. J Bone Joint Surg 2021;103:2190-2199. 21. Eltorai AEM, Durand WM, Haglin JM, Rubin LE, Weiss APC, Daniels AH: Trends in Medicare reimbursement for orthopedic procedures: 2000 to 2016. Orthopedics 2018;41:95-102. 22. Nayar SK, Wollstein A, Sullivan BT, et al.: Are we working harder for less pay? A survey of Medicare reimbursement for hand and upper extremity surgery. Plast Reconstr Surg 2022;149:711e-719e. 23. Lilly SI, Stern PJ: Simultaneous carpal tunnel release and Dupuytren's fasciectomy. J Hand Surg Br 2010;35:754-759.
Comments (0)