
Remember me




Total hip arthroplasty (THA) is among the most common and successful surgical procedures worldwide, and the incidence is expected to only increase in the coming years.1,2 Outpatient arthroplasty with same-day discharge (SDD) has grown in popularity in the past decade, largely attributable to both increasing payor pressure to minimize cost and improve outcomes and improving surgical techniques, perioperative pain control, and rapid rehabilitation protocols, making such an endeavor feasible.3–5 As such, rates of SDD have been increasing exponentially, and it is estimated that by 2026, over half of all patients undergoing total joint arthroplasty (TJA) will be discharged home the same day.4 Following trends elsewhere in orthopaedics, in addition to standard hospital-based outpatient centers (HBCs), freestanding ambulatory surgery centers (ASCs) have been an increasingly popular site of care to defray cost, improve surgical efficiency, and improve patient outcomes. With the recent addition of THA to the Centers for Medicare and Medicaid Services ASC-approved list, the utilization of ASC for TJA is only expected to grow.
Numerous previous studies have demonstrated the feasibility and safety of SDD in both a HBC and ASC after TJA.4,6–14 As arthroplasty shifts from a fee-for-service to value-based reimbursement model, maximizing understanding of both cost savings and patient satisfaction, by means of patient-reported outcome measures, will be critical to continue to provide the highest value care for patients. However, there remains a paucity of literature regarding patient-reported outcomes after outpatient TJA in the ASC setting, particularly comparing HBCs and ASCs. As such, the goal of this study was to compare patient-reported outcomes at 1 year after SDD after THA performed at either an HBC or an ASC while controlling for patient comorbidities.
MethodsAfter obtaining institutional review board approval, patients undergoing primary THA by one of 10 surgeons with SDD from a single HBC and a single ASC between December 2020 and 2021 were identified. The ASC is a stand-alone center, located adjacent to the hospital campus, and all included surgeons perform primary THA at both locations. Postoperative analgesia protocols varied based on surgeon; however, these were consistent between surgical settings for each included surgeon. Perioperative protocols were similar in both settings, with spinal anesthesia as the predominant modality used at the discretion of the anesthesia provider. Setting for THA as well as suitability for SDD was determined at the discretion of the operating surgeon. Absolute exclusion criteria for surgery in the ASC setting included American Society of Anesthesiologists (ASA) ≥3 and baseline mobility limitations precluding SDD. All patients undergoing THA at either the HBC or ASC were given the option preoperatively to enroll in a digital care platform through which patient-reported outcomes can be collected (Force Therapeutics).
Patients were included in the study if they underwent THA with SDD from either the HBC or ASC and were enrolled in the digital care platform. Patients undergoing THA by a direct anterior and posterolateral approach were included. Demographic information and patient comorbidities were collected. Ninety-day complications including readmission, revision surgery, and presentation to the emergency department (ED) were collected. Patients were also asked to self-report complications through the digital care platform, and surgeons were asked to report complications through an internal system. Patient-reported outcomes, including Hip Osteoarthritis Outcome Score (HOOS JR) and Veterans RAND 12-Item Health Survey (VR-12) score, were collected preoperatively and at 3, 6, and 12 months postoperatively. Procedural satisfaction using a 5-point Likert scale was collected at 1 year postoperatively.
Patients were matched in a 1:1 ratio by age and ASA. Chi-squared analysis was conducted to compare categorical variables, and a Wilcoxon rank-sum test was conducted for continuous variables. Linear regression models were conducted considering age, sex, ASA, and presence of diabetes, coronary artery disease, anxiety/depression, and obstructive sleep apnea (OSA). A P value of 0.05 was used as the threshold for statistical significance. With 170 patients per group, power analysis demonstrated an ability to detect a six-point difference in HOOS JR scores, with 80% power and alpha of 0.05.
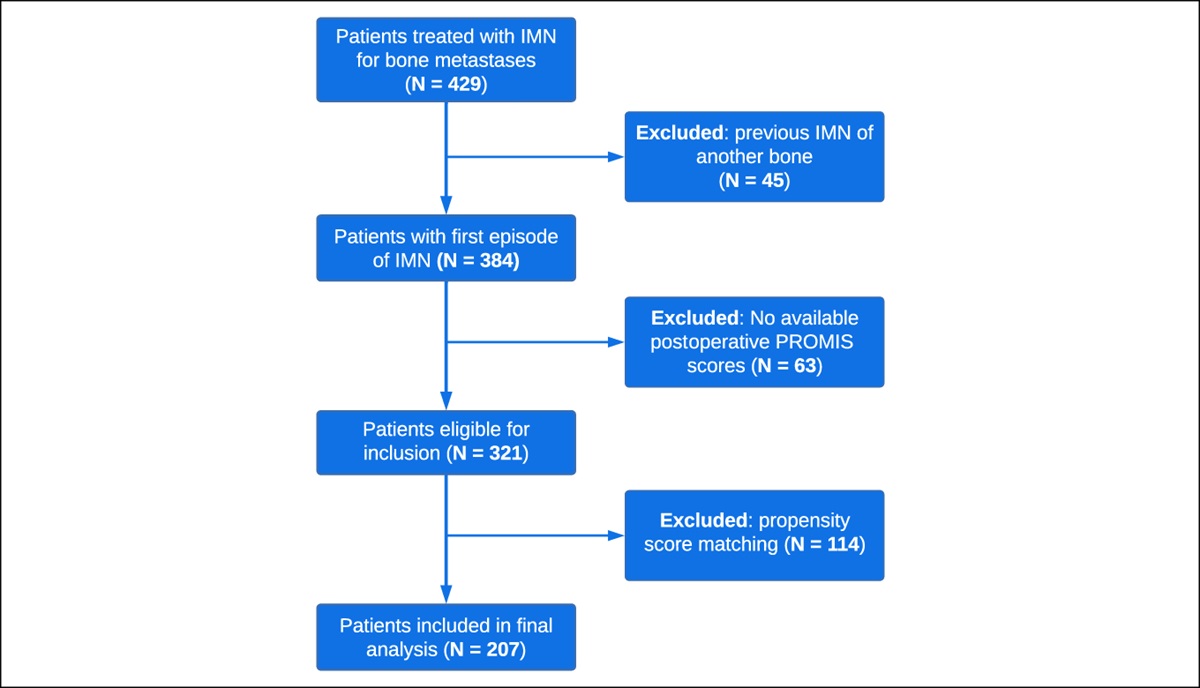
ResultsA total of 1,185 patients meeting inclusion criteria were identified, 170 of which were in the ASC setting. Patient characteristics and preoperative comorbidities are summarized in Table 1. Patients in the HBC group were significantly older (mean age 65.8 versus 58.8, P < 0.001) with more comorbidities (23.3% ASA 3 versus 7.1%, P < 0.001). After matching in a 1:1 ratio by age and ASA, each group had 170 patients. Mean age in the HSC and ASC groups was 59.1 ± 7.6 and 59.0 ± 8.1 years, respectively. Each cohort comprised ASA 1 (4.7%), 2 (88.2%), and 3 (7.1%) (Table 1). The HBC group had a significantly higher proportion of patients with preexisting diabetes (P < 0.001), OSA (P = 0.045), and chronic steroid use (P < 0.001).
Table 1 - Patient Characteristics Factor N Age (SD) ASA DM CAD CHF CKD RA Chronic Steroids OSA COPD Depression/Anxiety Full cohort 1 2 3 HBC 1015 65.8 (9.27) 11 766 237 646 111 17 50 21 133 16 41 212 ASC 170 58.8 (8.07) 8 150 12 9 8 1 2 1 0 198 1 30 P <0.001 <0.001 <0.001 0.046 0.5541 0.0732 0.3865 <0.001 0.0113 0.0648 0.8625 Matched cohort 1 2 3 HBC 170 59.1 (7.6) 8 150 12 103 11 3 6 1 20 31 3 39 ASC 170 59.0 (8.1) 8 150 12 10 8 1 3 2 0 18 1 37 P 1.00 <0.001 0.4787 0.3144 0.3108 0.5620 <0.001 0.0447 0.3144 0.7946ASC = ambulatory surgery center, CAD = coronary artery disease, CHF = congestive heart failure, CKD = chronic kidney disease, COPD = chronic obstructive pulmonary disease, DM = diabetes mellitus, HBC = hospital-based center, OSA = obstructive sleep apnea, RA = rheumatoid arthritis
A total of 26 90-day complications were found in the full HBC cohort, including three venous thromboembolic events, three infections, three periprosthetic fractures, six dislocations, two hematomas, one acute myocardial infarction, two episodes of cardiac arrhythmia, one pneumonia, and five “other.” After 1:1 matching, there were five 90-day complications, four in the HBC group (one periprosthetic fracture, one deep vein thrombosis, two infections) and one in the ASC group (one mechanical fall resulting in an ED visit with no associated injuries). No significant difference was observed in complication rates between groups before (P = 0.247) or after matching (P = 0.371).
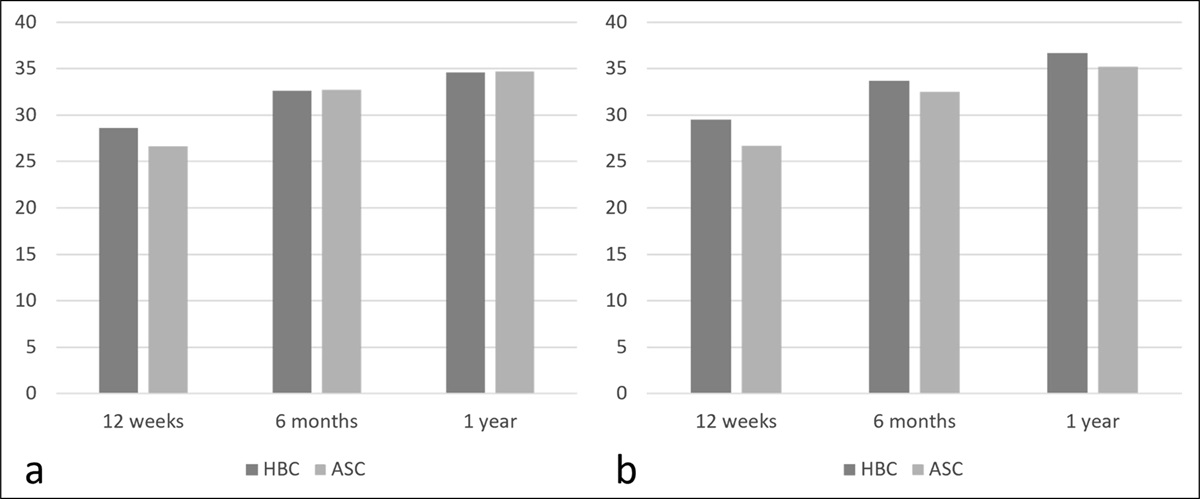
HOOS JR scores increased at each postoperative time point in both groups. Table 2 presents HOOS JR scores at all time points, and Figure 1 displays change in preoperative HOOS JR scores at all postoperative time points. Before matching, HOOS JR scores were significantly higher in the ASC group preoperatively (P = 0.0228), at 6 months (P = 0.0085), and at 1 year (P = 0.0269). However, there was no notable difference in change in HOOS JR scores from preoperative to any postoperative time point. After 1:1 matching, the preoperative HOOS JR score was lower in the HBC group (P = 0.046), with no significant difference in HOOS JR scores between groups at any postoperative time point and no significant difference in change in HOOS JR scores between groups at any postoperative time point.
Table 2 - HOOS JR Scores by Groups Preoperatively and at Time Points 12 wk, 6 mo, and 1 yr Postoperatively Factor HBC (SD) ASC (SD) P Full cohort Preoperative 52.5 (13.3) 54.7 (12.3) 0.0228 12 wk 81.6 (13.9) 82.0 (17.1) 0.6813 6 mo 85.1 (13.5) 88.1 (17.1) 0.0085 1 yr 87.3 (18.1) 89.7 (15.5) 0.0269 Matched cohort Preoperative 52.0 (12.1) 54.7 (12.1) 0.046 12 wk 81.4 (14.0) 82.0 (11.9) 0.848 6 mo 86.1 (13.5) 88.1 (12.0) 0.264 1 yr 88.9 (12.1) 89.8 (12.2) 0.403ASC = ambulatory surgery center, HBC = hospital-based center
 Figure 1:
Figure 1: Graphs demonstrating change in preoperative Hip Osteoarthritis Outcome Score JR scores at 12 weeks, 6 months, and 1 year postoperatively in the (A) full cohort and (B) matched cohort. ASC = ambulatory surgery center, HBC = hospital-based center
VR-12 Physical Component Score (PCS) and Mental Component Score (MCS) are presented in Table 3. In the unmatched groups, PCS was markedly higher in the ASC group at all time points and the MCS was markedly higher preoperatively and at 6 months. After matching, the HBC group had a significantly lower PCS preoperatively (P = 0.002) and at 12 weeks (P = 0.037). No notable difference was observed in PCS between matched groups at any other time points, and there was no notable difference in MCS at any time points.
Table 3 - VR-12 PCS and MCS of the Matched Cohort Preoperatively and at 12 wk, 6 mo, and 1 yr Postoperatively Factor HBC ASC P Preoperative PCS 31.6 (9.0) 35.0 (9.6) 0.002 MCS 52.2 (10.4) 54.1 (9.5) 0.144 12 wk PCS 44.0 (9.0) 46.3 (8.1) 0.037 MCS 55.8 (8.7) 56.9 (6.8) 0.611 6 mo PCS 48.6 (8.2) 50.5 (6.9) 0.061 MCS 55.0 (8.3) 56.5 (6.8) 0.144 1 yr PCS 49.2 (8.4) 50.8 (7.2) 0.133 MCS 56.0 (7.4) 56.4 (6.2) 0.987ASC = ambulatory surgery center, HBC = hospital-based center, MCS = Mental Component Score, PCS = Physical Component Score
Patient satisfaction was evaluated at 3 months and 1 year. This is given in Table 4. Before matching, patients in the ASC group had markedly higher procedural satisfaction at 3 months (P < 0.001). No significant difference was observed at 1 year (P = 0.4184). No notable difference was observed between matched groups in the proportion of patients reporting they are satisfied or very satisfied (4 or 5) versus patients reporting they are very unsatisfied, unsatisfied, or neutral (1, 2, or 3) (94% satisfied in the HSC group versus 93% satisfied in the ASC group, P = 0.706).
Table 4 - Satisfaction Scores of the Matched Cohort at 12 wk and 1 yr Postoperatively Factor HBC (%) ASC (%) P 12 wk 1 2 (1.4) 0 (0) 0.159 2 1 (0.7) 0 (0) 0.320 3 6 (4.1) 3 (2.1) 0.320 4 19 (13.1) 18 (12.6) 0.896 5 117 (80.7) 122 (85.3) 0.296 1 yr 1 3 (2.2) 1 (0.7) 0.290 2 5 (3.7) 0 (0) 0.021 3 0 (0) 9 (6.3) 0.003 4 18 (13.3) 26 (18.3) 0.257 5 109 (80.7) 106 (74.7) 0.224ASC = ambulatory surgery center, HBC = hospital-based center
The linear regression model demonstrated a notable association of preoperative anxiety/depression with a lower preoperative HOOS (P = 0.0388). No other factors were associated with the preoperative HOOS. Age was the only notable predictor of the 1-year postoperative HOOS and change in HOOS, with age older than 65 associated with less increase and a lower 1-year postoperative HOOS.
DiscussionOutpatient THA has the potential to result in substantial cost savings, with one previous study finding a nearly $7,000 cost decrease for patients undergoing outpatient compared with inpatient THA.3 The utilization of ASCs has the potential to further decrease costs, with a reported saving of over $12,000 when compared with inpatient THA.15 Additional benefits of SDD after THA include faster time to mobilization and improved patient satisfaction and patient-reported outcomes when compared with inpatient THA.7–9,11,13 In this study, we found THA in the ASC setting to be noninferior to HBCs with regard to patient-reported HOOS JR, VR-12, and VAS satisfaction scores at 1 year, as well as noninferior with regard to 90-day postoperative complications, return to ED, readmission, and revision surgery.
Previous studies have demonstrated the safety and feasibility of outpatient THA, with a large meta-analysis finding lower complication and readmission rates in outpatient compared with inpatient THA.6 This decreased complication rate is likely related to patient selection, with only baseline healthier patients being offered outpatient THA. In a database study comparing 90-day complication rates between inpatient and outpatient THA when controlling for patient comorbidities, Debbi et al4 found no notable difference in postoperative complications. In addition, outpatient THA has been shown not to increase healthcare utilization postoperatively, with no increase in calls to the office, acute office visits, ED visits, readmissions, or revision surgeries.7,16
Data comparing complication rates between HBC and ASC settings for THA are more limited. Wodowski et al15 directly compared rates of adverse events in THA in the HBC versus ASC settings, with equivalent rates between groups. The complication rate in this study, which is comparable to those reported previously for both outpatient and inpatient THA, reaffirms the safety of outpatient THA in the ASC setting.3,7,11,12,17
The matched groups in our study had improvements in patient-reported outcomes from preoperative to postoperative time points, without notable difference between groups at any postoperative time point, demonstrating the noninferiority of outpatient THA in the ASC setting regarding patient-reported outcomes. Matching by age and ASA helped to control for preoperative patient factors that may have influenced PROs because previous research has demonstrated that older age and higher ASA are associated with worse PROs after THA.18,19 There remained some baseline differences between groups, with a greater number of patients in the HBC group with diabetes and coronary artery disease. However, the linear regression model did not demonstrate that either of these factors was predictive of HOOS JR scores preoperatively or postoperatively at any time point.
Despite the favorable outcomes in this study, careful patient selection remains crucial in determining patients appropriate for outpatient THA in the ASC setting.20 Previous studies have found that inability to clear physical therapy and patient preference are the most common reasons for failed SDD. The inability to clear physical therapy is associated with preoperative mobility, smoking status, and comorbidities.21–23 The increased logistical difficulties associated with inpatient admission after failed SDD from an ASC make it even more imperative that comorbidities, preoperative functional status, patient motivation, and patient preference are all taken into account when considering patients for SDD and highlight the importance of shared decision making.
Limitations of this study are related to the retrospective nature and relatively limited sample size and duration of follow-up. However, as noted in the Methods section, the sample size was appropriate to capture clinically significant differences in patient reported outcome measures. A 1-year time point for patient-reported outcomes was selected because this was thought to be sufficient to capture major differences in patient satisfaction as related to the site of care. Determination of postoperative complications relied on self-reporting by patients and surgeons if they did not present to the study institution with a complication, which could have resulted in incomplete reporting of complications. In addition, the inclusion of only patients enrolled in the digital care platform with complete PRO data does introduce response bias. However, this is expected to affect both matched groups equally. The use of the digital care platform for PRO collection is relatively new at our institution, and larger studies with longer term follow-up will be possible in the future because a greater number of patients are enrolled.
ConclusionsOverall, in this retrospective matched cohort study, there were equivalent 90-day complication rates and 1-year PROs in patients undergoing outpatient THA at either an HBC or an ASC, suggesting noninferiority of THA in the ASC setting for appropriately selected patients. Based on this study, surgeons can be further assured that with appropriate patient selection, THA at ASC maintains excellent patient satisfaction while minimizing complication rates.
References 1. Sloan M, Premkumar A, Sheth NP: Projected volume of primary total joint arthroplasty in the U.S., 2014 to 2030. J Bone Joint Surg Am 2018;100:1455-1460. 2. Learmonth ID, Young C, Rorabeck C: The operation of the century: Total hip replacement. Lancet 2007;370:1508-1519. 3. Aynardi M, Post Z, Ong A, Orozco F, Sukin DC: Outpatient surgery as a means of cost reduction in total hip arthroplasty: A case-control study. HSS J 2014;10:252-255. 4. Debbi EM, Mosich GM, Bendich I, Kapadia M, Ast MP, Westrich GH: Same-day discharge total hip and knee arthroplasty: Trends, complications, and readmission rates. J Arthroplasty 2022;37:444-448.e1. 5. Rozell JC, Ast MP, Jiranek WA, Kim RH, Della Valle CJ: Outpatient total joint arthroplasty: The new reality. J Arthroplasty 2021;36(7S):S33-S39. 6. Bordoni V, Marelli N, Previtali D, Gaffurini P, Filardo G, Candrian C: Outpatient total hip arthroplasty does not increase complications and readmissions: A meta-analysis. Hip Int 2022;32:326-333. 7. Goyal N, Chen AF, Padgett SE, et al.: Otto Aufranc Award: A multicenter, randomized study of outpatient versus inpatient total hip arthroplasty. Clin Orthop Relat Res 2017;475:364-372. 8. Kelly MP, Calkins TE, Culvern C, Kogan M, Della Valle CJ: Inpatient versus outpatient hip and knee arthroplasty: Which has higher patient satisfaction? J Arthroplasty 2018;33:3402-3406. 9. Pollock M, Somerville L, Firth A, Lanting B: Outpatient total hip arthroplasty, total knee arthroplasty, and unicompartmental knee arthroplasty: A systematic review of the literature. JBJS Rev 2016;4:e4. 10. Reddy NC, Prentice HA, Paxton EW, Hinman AD, Lin AG, Navarro RA: Association between same-day discharge total joint arthroplasty and risk of 90-day adverse events in patients with ASA classification of ≥3. J Bone Joint Surg Am 2021;103:2032-2044. 11. Rosinsky PJ, Chen SL, Yelton MJ, et al.: Outpatient vs. inpatient hip arthroplasty: A matched case-control study on a 90-day complication rate and 2-year patient-reported outcomes. J Orthop Surg Res 2020;15:367. 12. Schmidt AM, Garval M, Gromov K, et al.: Feasibility, safety, and patient-reported outcomes 90 days after same-day total knee arthroplasty: A matched cohort study. Acta Orthop 2022;93:509-518. 13. Shapira J, Chen SL, Rosinsky PJ, Maldonado DR, Lall AC, Domb BG: Outcomes of outpatient total hip arthroplasty: A systematic review. Hip Int 2021;31:4-11. 14. Weiser MC, Kim KY, Anoushiravani AA, Iorio R, Davidovitch RI: Outpatient total hip arthroplasty has minimal short-term complications with the use of institutional protocols. J Arthroplasty 2018;33:3502-3507. 15. Wodowski AJ, Throckmorton TW, Mihalko WM, Toy PC: Anterior supine intermuscular total hip arthroplasty at an ambulatory surgery center versus hospitalization: Cost and adverse events. Orthop Clin North Am 2021;52:209-214. 16. Husted CE, Husted H, Nielsen CS, Mikkelsen M, Troelsen A, Gromov K: No increase in postoperative contacts with the healthcare system following outpatient total hip and knee arthroplasty. Acta Orthop 2021;92:557-561. 17. Courtney PM, Boniello AJ, Berger RA: Complications following outpatient total joint arthroplasty: An analysis of a national database. J Arthroplasty 2017;32:1426-1430. 18. Lungu E, Maftoon S, Vendittoli PA, Desmeules F: A systematic review of preoperative determinants of patient-reported pain and physical function up to 2 years following primary unilateral total hip arthroplasty. Orthop Traumatol Surg Res 2016;102:397-403. 19. Sniderman J, Stark RB, Schwartz CE, Imam H, Finkelstein JA, Nousiainen MT: Patient factors that matter in predicting hip arthroplasty outcomes: A machine-learning approach. J Arthroplasty 2021;36:2024-2032. 20. Meneghini RM, Ziemba-Davis M, Ishmael MK, Kuzma AL, Caccavallo P: Safe selection of outpatient joint arthroplasty patients with medical risk stratification: The “outpatient arthroplasty risk assessment score”. J Arthroplasty 2017;32:2325-2331. 21. Fraser JF, Danoff JR, Manrique J, Reynolds MJ, Hozack WJ: Identifying reasons for failed same-day discharge following primary total hip arthroplasty. J Arthroplasty 2018;33:3624-3628. 22. Kim KY, Anoushiravani AA, Elbuluk A, Chen K, Davidovitch R, Schwarzkopf R: Primary total hip arthroplasty with same-day discharge: Who failed and why. Orthopedics 2018;41:35-42. 23. Rodriguez S, Shen TS, Lebrun DG, Della Valle AG, Ast MP, Rodriguez JA: Ambulatory total hip arthroplasty: Causes for failure to launch and associated risk factors. Bone Jt Open 2022;3:684-691.
Comments (0)