
Remember me




Surgery is associated with physiologic insult and inflammation that patients must overcome. Complications and failure to overcome such insults may lead to potentially poor outcomes, the need for revision surgery, and an increase in the overall cost of care. The prevention of postsurgical site infections (SSIs) is an area of intense research interest. It is estimated that as many as 8% of surgeries in the United States are complicated by a postoperative infection of the surgical site.1 SSIs are the leading cause of nosocomial infections among surgical patients in the United States, accounting for 17% of all hospital-acquired infections.2 SSI can be devastating for patients and may result in hospital readmissions, increased time in intensive care units, revision surgeries, and increased mortality.3 A 2022 analysis estimated the cost of SSI to the US economy at over $3.7 billion annually.4 There are many well-established risk factors of SSI, such as age, hyperglycemia, hypoxia, and length of surgical time.1,5–7 Despite widespread attention, awareness and education campaigns, and new standards of care, the incidence of SSI remains relatively unchanged.8 An intriguing area of research in the prevention of SSI centers on the role of intraoperative temperature specifically the effect of perioperative hypothermia (PH). Two highly publicized RCTs in 1996 and 2001 ushered in a new wave of practice changes and standards of care for the management of perioperative temperature across practically every surgical field. Several studies have demonstrated that PH increased the incidence of SSI in patients undergoing abdominal surgery.9–16 However, a more recent 2019 meta-analysis concluded that there was no consistent association between PH and SSI.17 Furthermore, in the PROTECT trial, Sessler et al12 found no association between temperature status and SSI in patients undergoing noncardiac surgery. Given these conflicting results, we hope to add clarity to the current debate in the literature about the importance of intraoperative temperature management while simultaneously adding to the dearth of evidence regarding (1) the interplay between PH and established risk factors of surgical site infections, such as diabetes mellitus (DM), and (2) the incidence and importance of PH because it specifically relates to orthopaedic surgery.
The mechanism by which PH may increase the risk of infection is unknown; however, it is hypothesized that hypothermia increases the risk of infection by three synergistic mechanisms: (1) Increased risk of wound dehiscence exposes the surgical wound to contaminants; (2) decreased immune cell motility impairs the ability of leukocytes to migrate to sites of microbe seeding; and (3) decrease in the efficacy of O2-dependent killing by polymorphonuclear neutrophils results in ineffective clearance of microbes.18,19 In healthy individuals, normal core body temperature (CBT) is tightly regulated within tenths of a degree throughout the day.20 A slight drop in CBT triggers a compensatory vasoconstrictive response.21,22 A decrease in CBT by as little as 1°C activates a physiologic shivering response, which can increase the metabolic rate by a factor of five.23 However, in patients undergoing surgery, the use of anesthesia depresses the thresholds for vasoconstriction and shivering by as much as 2.5°C, inhibiting an individual's physiologic compensatory response and allowing patients' CBT to reach new nadirs.16 As a result, PH is considered common in surgical patients, but owing to its relatively recent emergence as a topic of interest, estimates of its incidence range widely. It is thought that PH affects between 20% and 90% of all surgical operations.9,13,16,20,21 The current surgical standard of care for perioperative thermoregulation is to keep patients normothermic. However, this poses a challenge in the operating room. Moreover, practice patterns for managing temperature vary from aggressive temperature management to more passive techniques. At our institution, patients are managed with temperature monitoring intraoperatively but aggressive preoperative and postoperative management is less strictly used.
It has been well documented that owing to multiple biochemical and vascular factors, DM is a strong independent risk factor of SSI, doubling some surgical patients' risk.1,5,17,19,24–30 It follows that if an association between PH and SSI exists, mechanistically, it would be more apparent in a population with a previously established increased risk of SSI, such as in patients with DM. However, there are very few published studies in this population in the field of orthopaedic surgery, suggesting a critical need in the literature for this work. As such, we sought to (1) evaluate the role of hypothermia in patients with diabetes who underwent orthopaedic surgery and (2) estimate the incidence of PH in orthopaedic surgery. We hypothesized that PH in the setting of DM will increase the risk of postoperative SSIs.
Methods Patient PopulationA retrospective chart review was conducted on all patients with DM who underwent elective orthopaedic surgery at our academic teaching institution between May 1, 2018, and April 1, 2022. This retrospective chart review was approved by our institutional review board. Inclusion criteria were as follows: all patients older than 15 years with a history of DM (type 1 or 2) or a recent HbA1c level ≥6.5% who received general anesthesia for elective orthopaedic surgeries and nonurgent fracture care of at least 60 minutes in duration. All procedures were performed at our academic teaching institution, and there were no procedures performed at a surgery center. An HbA1c level ≥6.5% was chosen because this is considered diagnostic for DM according to the American Diabetes Association. It is part of our institution's routine preoperative workup to assess the patient's glucose levels; however, several patients had no recorded glucose levels so recent HbA1c levels in the electronic health record (EHR) were captured for analysis instead. Elective and nonurgent procedural patients all underwent preoperative optimization according to AAOS guidelines and hospital protocols. Such standardization is done to minimize variances and optimize surgical outcomes. As part of this optimization, patients underwent preoperative education and were given knowledge and acute management of their glycemic status. By contrast, nonurgent surgical cases did not undergo prolonged optimization but were medically optimized in the acute setting. Nonurgent procedures included all outpatient fracture care, fractures among patients who were medically optimized, and those with osseous malignancy requiring prophylactic intervention. A minimum surgical length of 60 minutes was chosen as the minimum length of surgery for inclusion because it would allow adequate time for PH to develop.
In keeping with the methodology of previously published literature,9,10 the authors excluded patients who (1) had an altered preexisting metabolic state that may affect thermoregulation (ie, hyperthyroidism, hypothyroidism, hyperadrenalism, and hypoadrenalism) or (2) presented for surgery with a febrile illness (core temperature >37.5°C). In addition, the authors elected to exclude (3) patients who received only regional anesthetics or “monitored anesthesia care” to minimize confounding from the type of anesthesia given, (4) patients who used a skin or axillary source for their intraoperative temperature recordings, and (5) patients who were being treated for an infection. For patients who underwent multiple eligible orthopaedic procedures during the defined period, each surgery was treated as an independent event. For example, if a patient had a right total knee arthroplasty and returned 12 months later for a left total knee arthroplasty, they were considered two independent operations. A total of 236 operations were performed in 211 patients. Twenty patients underwent more than one procedure. Sixteen patients underwent two procedures, three patients had three procedures, and one patient had four procedures. The following are the orthopaedic procedures included in the final analysis: ankle arthroscopy, ankle fusion, ankle open reduction and internal fixation (ORIF), above-knee amputation, basilar joint arthroscopy, carpectomy, rotational hand flap, total hip arthroplasty, humeral intramedullary rod insertion, knee arthroscopy, total knee arthroplasty (distinction not made between primary and revision, or robotic), perilunate dislocation ligament repair, radius ORIF, ulnar ORIF, shoulder arthroscopy, total shoulder arthroplasty (distinction not made between primary and revision), shoulder mass excision, and tibial pilon ORIF. Femoral nailing, gamma nailing, and femur ORIFs were included when they were performed in the setting of nonunion surgery and osseous malignancy or in the outpatient setting.
Power AnalysisA priori power analysis was completed at the outset of the study. Based on a review of previous literature, it was estimated that the incidence of SSI in orthopaedic surgery patients experiencing PH and normothermia was 19% and 6%, respectively. Assuming an alpha of 0.05, a beta of 0.1, and power of 0.9, it was determined that a sample size of 268 patients was required.
Data CollectionThe patients' preoperative temperature, lowest intraoperative temperature, final intraoperative temperature, and temperature on transfer to the post-anesthesia care unit were collected from the EHR, intraoperative anesthesia record, and anesthesia handoff notes. These were recorded automatically by an intraoperative monitoring system. Basic demographic data relating to each patient, including age, race, ethnicity, sex, body mass index (BMI), HbA1c levels, length of surgery, and type of the anesthetic agent administered, were also recorded from the EHR. All body temperatures were recorded using an esophageal or nasopharyngeal probe thermometer. The patient's temperature was recorded at the induction of anesthesia, periodically during the intraoperative period, and at the conclusion of anesthesia. Patients with incomplete time and temperature data were excluded from the study. The length of the operation was defined as the time from the first incision to closure. These time points were obtained from intraoperative anesthesia records. All patients received general anesthesia.
The primary outcome of SSI was defined as any type of infection of the surgical wound, including deep or superficial, or infection of the prosthesis when applicable, within 90 days. All patients underwent an extensive EHR review that included postoperative notes, postoperative physical examination documentation, physical therapy notes, MyChart communications, EHR “Problem List,” and primary care provider notes for any mention of infection or findings concerning for SSI. Perioperative hypothermia was defined as a core temperature of 35.5°C or lower recorded during any part of the procedure. Despite previous studies defining hypothermia as CBT ≤36°C,31–33 we chose to use a more stringent cutoff of 35.5°C to prevent patients with low basal body temperatures from being included in the hypothermic cohort. This decision mirrored that of Simpson et al10 in their recent work.
Logistic RegressionWe created multivariable logistic regression models to estimate the effect of perioperative temperature status and glycemic control on the rate of SSI. We included variables that were notable in univariate logistic regression and known risk factors of orthopaedic SSI5,34–36 in the final multivariable models. We modeled the full study population, as well as patients who underwent perioperative normothermia and hypothermia. When assessing model discrimination, the predicted probability threshold was set to 6% because this was equal to the prevalence of SSI in the study population. We calculated the concordance statistic (c-statistic) to assess the discriminatory abilities of the models. The 95% confidence intervals for the c-statistics were determined by bootstrapping with 1,000 replicates.
Statistical AnalysisCategorical variables were compared using the chi-squared test. Continuous variables were compared using the Wilcoxon rank-sum test. Missing data within continuous variables were imputed by replacing missing values with the median of the variable. The only variable with missing data was hemoglobin A1c, which was missing for three procedures. The outputs of logistic regression models were reported as odds ratios; however, because the outcome of interest (ie, SSI) was rare in the study population, odds ratios were assumed to approximate relative risk.37 All analyses were conducted using R version 4.0.4 and RStudio (RStudio Team, 2021. RStudio: Integrated Development for R. RStudio, Public Benefit Corporation). See the Supplemental Material for access to all analysis codes. All statistical tests were two-sided, and statistical significance was set at P < 0.05.
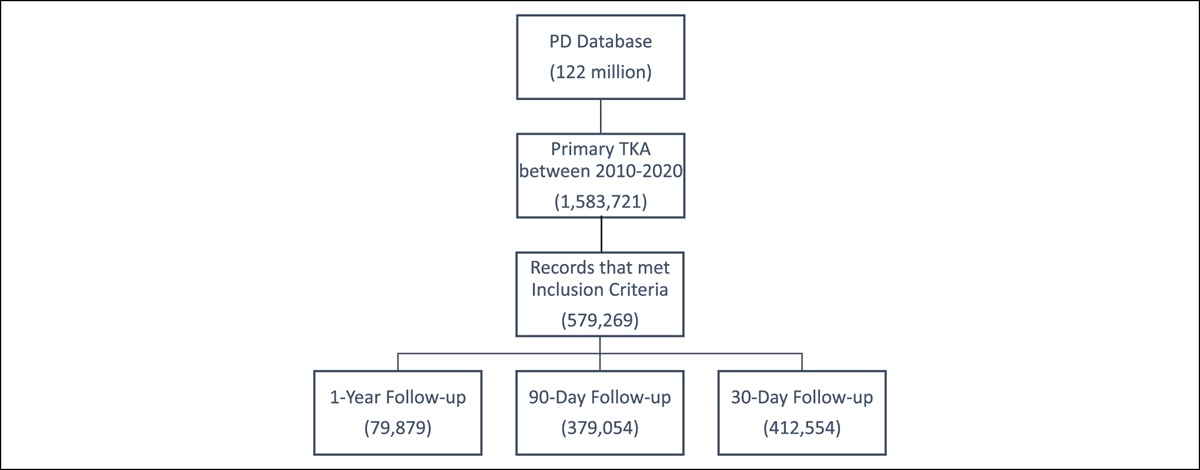
ResultsA total of 719 elective orthopaedic procedures from May 1, 2018, to April 1, 2022, were screened for inclusion. In total, 236 procedures met the inclusion criteria and were included in the analysis (Table 1). These procedures were performed by a total of 21 surgeons. Shoulder arthroscopy was the most common procedure performed, accounting for 33% (77/236), followed by total knee arthroplasty, comprising approximately 25% (60/236), and total shoulder arthroplasty, accounting for approximately 17% (40/236). These three procedure types accounted for approximately 75% of the total number of operations. Overall, the study population included 138 women (58%) and 98 men (42%). The mean age at operation was 63 years (±12.9, range 17 to 94), mean BMI was 33 (±7.0), mean HbA1c was 6.8% (±1.3), and mean surgical time was 119 minutes (±50.3, range 37 to 403 minutes).
Table 1 - Whole Study Population Characteristics Median, (interquartile range); n (%); N = 236 Patient age (yr) 64 (56, 70) Patient sex Female 138 (58%) Male 98 (42%) Temperature (°C) 35.70 (35.30, 36.10) Surgical time (minutes) 123 (92, 158) BMI (kg/m2) 33 (28, 38) Hemoglobin A1c (%) 7.00 (6.15, 7.50) Surgery type Other 59 (25%) Shoulder arthroscopy 77 (33%) Total shoulder arthroplasty 40 (17%) Total knee arthroplasty 60 (25%)Among the 236 operations, eight men (8.2%) and six women (4.3%) developed SSIs postoperatively (Table 2). These 14 cases resulted in a postoperative SSI incidence of 5.93%. Patients who developed SSI had significantly longer operation time (159 min vs. 118 min, P = 0.013). Of the 60 total knee arthroplasty operations, eight (13%) developed SSIs. Two patients who underwent shoulder arthroscopy (4%) and two patients undergoing shoulder arthroplasty (5%) developed SSIs. The type of surgery performed was not a risk factor of SSI (P = 0.068). No notable differences were observed in HbA1c, BMI, age, or sex between patients who developed SSI and those who did not develop SSI.
Table 2 - Patient Characteristics by Surgical Site Infection Status No Infection, N = 222a Surgical Site Infection, N = 14a P b Patient age (yr) 63 (55, 69) 67 (59, 72) 0.2 Patient sex 0.2 Female 132 (59%) 6 (43%) Male 90 (41%) 8 (57%) Temperature (°C) 35.70 (35.30, 36.10) 35.65 (35.42, 35.90) 0.8 Surgical time (minutes) 118 (92, 151) 159 (119, 214) 0.013 BMI (kg/m2) 33 (29, 39) 34 (31, 37) 0.7 Hemoglobin A1c (%) 6.80 (6.20, 7.50) 6.90 (6.25, 7.58) 0.6 Surgery type 0.068 Other 57 (26%) 2 (14%) Shoulder arthroscopy 75 (34%) 2 (14%) Total shoulder arthroplasty 38 (17%) 2 (14%) Total knee arthroplasty 52 (23%) 8 (57%)aMedian (interquartile range); n (%).
bWilcoxon rank-sum test; Pearson chi-squared test; Fisher exact test.
The cohort of patients who developed SSI was subdivided by temperature status (Table 3). Six of the patients who developed SSI experienced PH. Other than the lowest intraoperative temperature experienced, the two cohorts did not markedly differ. Perioperative hypothermia was not an independent risk factor of SSI in univariate logistic regression (OR = 1.04, 95% CI = 0.33 to 3.09, P-value = 0.94).
Table 3 - Patient Characteristics by Intraoperative Temperature Status Among Patients With Surgical Site Infection Normothermic, N = 8a Hypothermic, N = 6a P b Patient age (yr) 64 (58, 68) 70 (68, 74) 0.4 Patient sex >0.9 Female 3 (38%) 3 (50%) Male 5 (62%) 3 (50%) Temperature (°C) 35.90 (35.77, 36.02) 35.40 (35.32, 35.48) 0.002 Surgical time (minutes) 158 (120, 193) 162 (96, 245) >0.9 BMI (kg/m2) 35 (34, 38) 32 (28, 35) 0.3 Hemoglobin A1c (%) 6.45 (6.05, 7.32) 7.10 (6.85, 7.73) 0.2 Surgery type 0.9 Other 2 (25%) 0 (0%) Shoulder arthroscopy 1 (12%) 1 (17%) Total shoulder arthroplasty 1 (12%) 1 (17%) Total knee arthroplasty 4 (50%) 4 (67%)aMedian (interquartile range); n (%).
bWilcoxon rank-sum test; Fisher exact test.
In total, 99 patients (42%) experienced PH, of which 63 (64%) were female. The incidence of PH was not significantly different between men and women (37% vs 46%, P = 0.2) (Table 4). Incidence of PH was significantly different by surgery type (P < 0.001). While sex, race, ethnicity, and BMI did not differ between patients who experienced PH and patients who remained normothermic, patients in the hypothermic cohort were, on average, 4 years older (62 years vs. 66 years, P = 0.009) and had a lower preoperative hemoglobin A1c (6.9% vs. 6.5%, P < 0.001). Body mass index did not markedly differ between the two groups. Surgical time was not significantly different between groups (P = 0.3).
Table 4 - Patient Characteristics by Intraoperative Temperature Status Normothermic, N = 137a Hypothermic, N = 99a P b Surgical site infection 8 (5.8%) 6 (6.1%) >0.9 Patient age (yr) 62 (53, 68) 66 (58, 70) 0.009 Patient sex 0.2 Female 75 (55%) 63 (64%) Male 62 (45%) 36 (36%) Temperature (°C) 36.00 (35.80, 36.20) 35.20 (34.90, 35.40) <0.001 Surgical time (minutes) 120 (95, 157) 115 (90, 149) 0.3 BMI (kg/m2) 34 (30, 39) 32 (28, 38) 0.15 Hemoglobin A1c (%) 6.90 (6.40, 7.70) 6.50 (6.00, 7.10) <0.001 Surgery type <0.001 Other 44 (32%) 15 (15%) Shoulder arthroscopy 45 (33%) 32 (32%) Total shoulder arthroplasty 26 (19%) 14 (14%) Total knee arthroplasty 22 (16%) 38 (38%)an (%); median (interquartile range).
bPearson chi-squared test; Wilcoxon rank-sum test.
The normothermic and hypothermic cohorts were further divided according to SSI status (Table 5). Within the normothermic cohort, the subcohort that developed SSI had significantly longer surgical time compared with the infection-free subcohort (158 minutes vs. 119 minutes, P = 0.032). Within the hypothermic cohort, the subcohort of patients who went on to develop SSI had an average HbA1c that was 0.7% higher than the infection-free subcohort (P = 0.032). A univariate regression analysis among the 102 patients who experienced PH demonstrated that higher values of HbA1c were associated with increased risk of SSI (OR = 2.39, 95% CI: 1.12 to 5.32, P-value = 0.022).
Table 5 - Patient Characteristics by Intraoperative Temperature Status and Surgical Site Infection Status Normothermic Hypothermic No infection, N = 129a Surgical site infection, N = 81 P b No infection, N = 931 Surgical site infection, N = 61 P b Patient age (yr) 62 (53, 68) 64 (58, 68) 0.4 65 (58, 70) 70 (68, 74) 0.3 Patient sex 0.5 0.7 Female 72 (56%) 3 (38%) 60 (65%) 3 (50%) Male 57 (44%) 5 (62%) 33 (35%) 3 (50%) Temperature (°C) 36.00 (35.80, 36.20) 35.90 (35.77, 36.02) 0.5 35.20 (34.90, 35.40) 35.40 (35.32, 35.48) 0.029 Surgical time (minutes) 119 (93, 152) 158 (120, 193) 0.032 115 (91, 140) 162 (96, 245) 0.2 BMI (kg/m2) 34 (30, 39) 35 (34, 38) 0.6 32 (28, 38) 32 (28, 35) >0.9 Hemoglobin A1c (%) 7.00 (6.50, 7.70) 6.45 (6.05, 7.32) 0.3 6.40 (6.00, 7.00) 7.10 (6.85, 7.73) 0.032 Surgery type 0.095 0.5 Other 42 (33%) 2 (25%) 15 (16%) 0 (0%) Shoulder arthroscopy 44 (34%) 1 (12%) 31 (33%) 1 (17%) Total shoulder arthroplasty 25 (19%) 1 (12%) 13 (14%) 1 (17%) Total knee arthroplasty 18 (14%) 4 (50%) 34 (37%) 4 (67%)aMedian (interquartile range); n (%).
bWilcoxon rank-sum test; Fisher exact test.
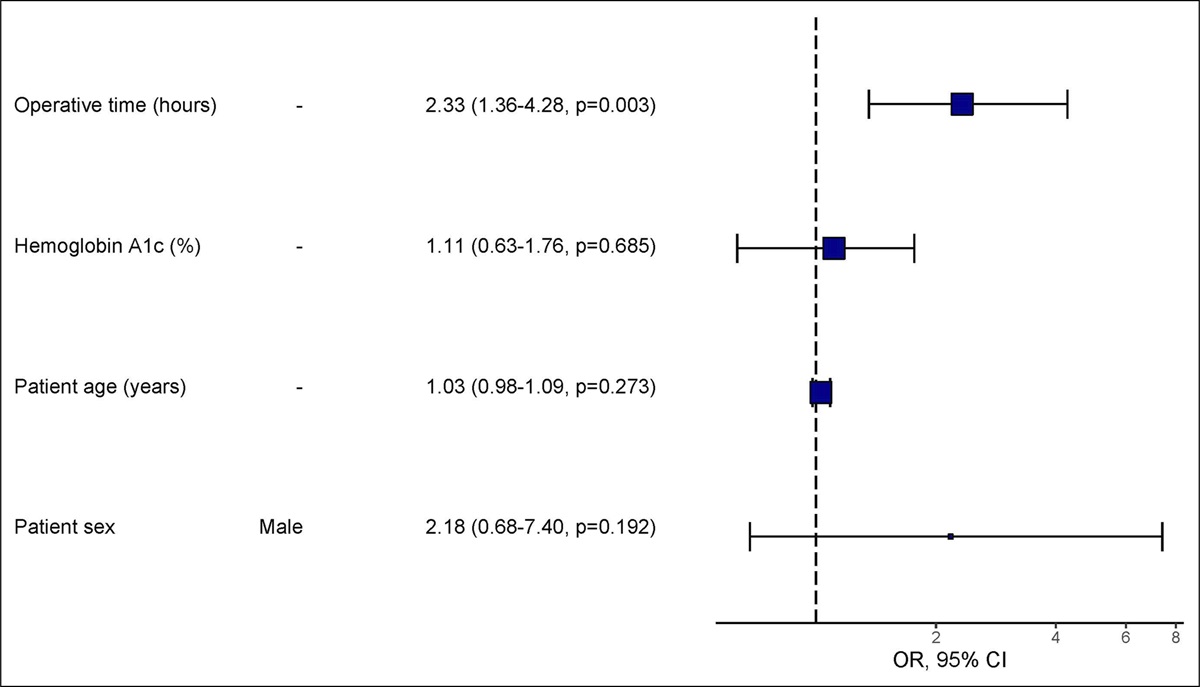
Univariate logistic regression models were created to identify variables that were independent predictors of SSI risk (Table 6). Surgical time was associated with increased risk of SSI (OR 2.45, 95% CI: 1.46 to 4.38, P = 0.001). A multivariable logistic regression model was constructed to predict the risk of SSI among the full study population. Surgical time was included as a predictor in the multivariable model because it was an independent risk factor of SSI in our population. Other known risk factors of SSI, including hemoglobin A1c, age, and sex, were also included as predictors. This model had good discriminatory ability (c-statistic 0.74, 95% CI: 0.61 to 0.89) and good predictive accuracy (sensitivity 64%, specificity 73%). Surgical time remained an independent risk factor of SSI in the multivariable model (Figure 1). Multivariable models were also constructed for patients who experienced PH (Figure 2) and those who did not experience PH. These models also demonstrated good discriminatory ability (hypothermic cohort c-statistic 0.82 [95% CI: 0.71 to 1.0], normothermic cohort c-statistic 0.77 [95% CI: 0.66 to 0.96]).
Table 6 - Univariate Logistic Regression for Predictors of Surgical Site Infections Characteristic OR 95% CI P Hemoglobin A1c (%) 1.04 0.66, 1.51 0.83 Patient age (yr) 1.03 0.99, 1.09 0.18 Temperature (°C) 1.35 0.59, 3.34 0.50 Intraoperative temperature < 35.5 C 1.04 0.33, 3.09 0.94 BMI (kg/m2) 1.02 0.94, 1.10 0.65 Surgical time (hours) 2.45 1.46, 4.38 0.001 Surgery type Other — — Shoulder arthroscopy 0.76 0.09, 6.49 0.79 Total shoulder arthroplasty 1.50 0.17, 12.9 0.69 Total knee arthroplasty 4.38 1.04, 29.9 0.069 Patient sex Female — — Male 1.96 0.66, 6.12 0.23OR = odds ratio, CI = confidence interval
 Figure 1:
Figure 1: Forest plot showing the results of a multivariable logistic regression model for surgical site infection (SSI). Surgical time was associated with significantly increased risk of SSI.
 Figure 2:
Figure 2: Forest plot showing the results of a multivariable logistic regression model for surgical site infection (SSI) among patients who experienced perioperative hypothermia (PH). In this cohort, surgical time and hemoglobin A1c were associated with significantly increased risk of SSI.
DiscussionRisk factors of SSI are of keen interest to the surgical community because they affect up to 8% of surgical operations in the United States, resulting in poor patient outcomes and over $3.7 billion annually of unnecessary and potentially preventable costs. The primary aim of our work was to evaluate the role of hypothermia in the development of SSI among patients with diabetes undergoing orthopaedic surgery. We hypothesized that PH would increase the odds of developing SSIs among patients with DM. Our findings demonstrate that PH may not be an independent risk factor of SSI in high-risk patients; however, it appears to be an additive risk factor in the setting of poor glycemic control and potentially in the setting of other known risk factors. This is a novel finding and differs from previous literature that either endorses PH as an independent risk factor of SSI or contradicts report that finds no association between PH and SSI.
Perioperative hypothermia is an intriguing frontier in surgical research because the medical community searches for interventions to aid in decreasing the rate of postoperative surgical site infections. The exact role of PH in the development of SSI has been increasingly debated. Some evidence points to normothermia as a critical component in limiting SSIs,9,13,15 whereas others suggest that it has little-to-no effect on the development of SSI.
Comments (0)