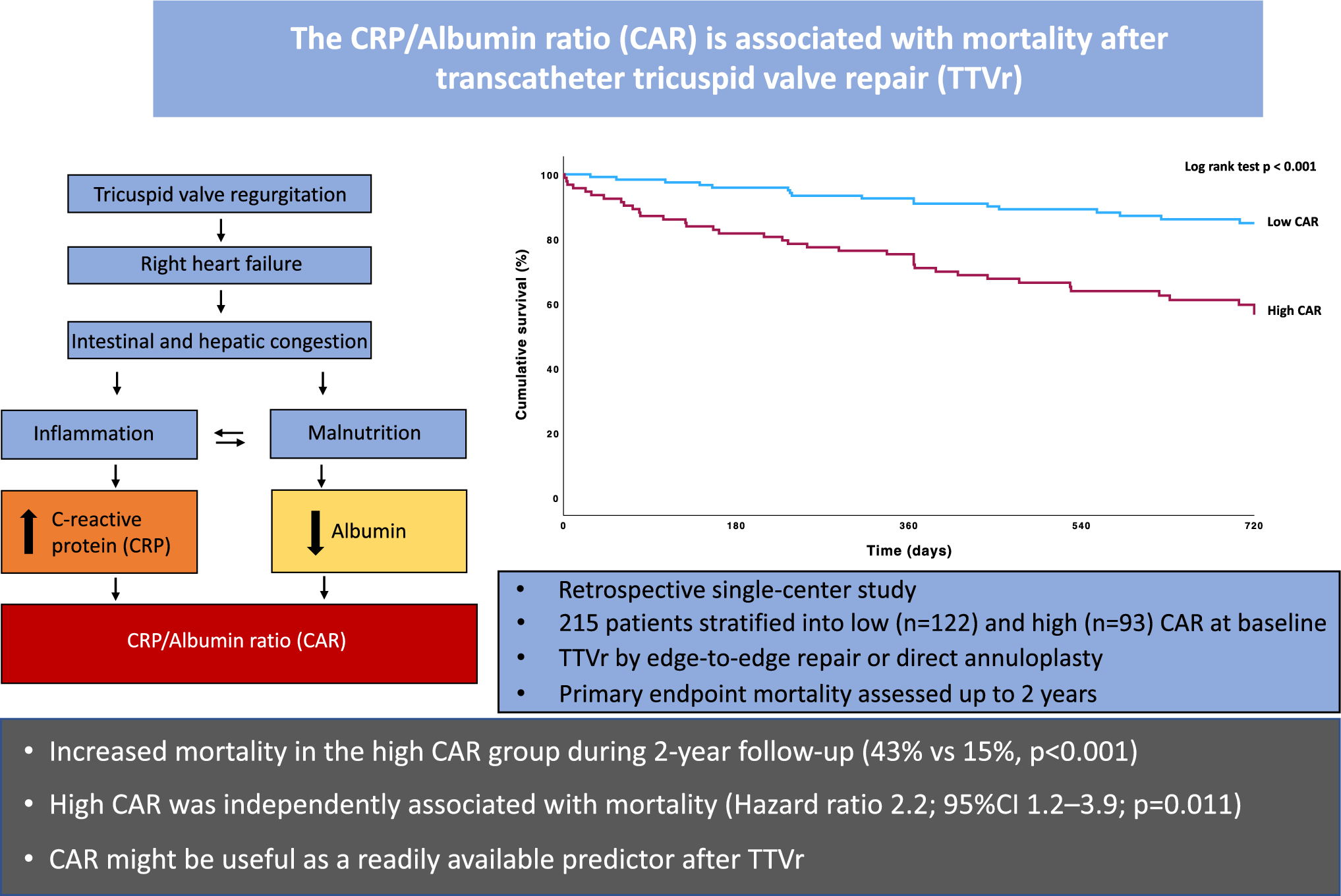
Aim of this study was to evaluate the association of CAR with mortality after TTVr. The main findings were:
a)
Patients of the high CAR subgroup had significantly worse renal function, increased mean right atrial pressure, and demonstrated less intraprocedural success compared to the low CAR group.
b)
CAR was independently associated with worse survival after TTVr even after adjusting for other significant parameters.
c)
Achieving intraprocedural success in patients with high CAR led to better survival after TTVr compared to patients with high CAR and procedural failure.
Risk stratification is key in identifying patients which benefit from TTVr. In search of everyday parameters representing risk in patients undergoing TTVr, we investigated CAR and its association with mortality. As a matter of fact, severe TR is complicated by backward failure and many patients present in late-stage disease [1]. Thus, CAR bears the potential of being readily available and reflects multi-organ complications of TR due to backward failure identifying high-risk patients. To the best of our knowledge, this is the first study to analyze CAR in the setting of TTVr.
The group of patients which died during follow-up had significantly higher CRP and lower albumin levels. Backward failure with intestinal congestion and micro-translocation of bacteria leading to systemic low-grade inflammation might be a mechanism of CRP elevation [6]. Advanced organ damage due to systemic congestion might further contribute to this inflammation and systemic congestion is represented by the higher right atrial pressure in the high CAR group. The overall study population was elderly and comorbidities were common, representing patients at risk for nosocomial infections [21]. As patients with pre-procedural infections were excluded or had TTVr postponed until clearance of infection, infections do not seem to be a relevant driver of mortality in the immediate postinterventional period in this study population. Patients with the highest CRP values were evaluated to assess infections as a cause of high CRP and driver of mortality. While infections were present in the patients with the highest CRP values, infections occurred only after procedure and were not associated with death in the first days after procedure. High CAR remained significantly associated with mortality even after exclusion of the CRP outliers, which supports that CAR reflects low-grade inflammation. The low albumin levels in the high CAR group can be explained by malabsorption and following malnutrition due to intestinal wall congestion [6]. Further hepatic congestion leads to hepatic damage and decreased hepatic synthesis of albumin [22]. Hepatic impairment is also represented by the significantly higher bilirubin in the high CAR group. Low albumin therefore also reflects backward organ damage due to TR.
Both CRP and albumin contribute to the CAR increase in this study, this being representative of progressive right-heart failure with systemic congestion, intestinal impairment with malnutrition, and low-grade systemic inflammation described by the other studies [6]. This study underlines this aspect of TR pathophysiology and suggests that increased attention should be given to patient factors like malnutrition and systemic low-grade inflammation representative of organ damage.
Several factors might drive the mortality in the high CAR group including low-grade inflammation, malnutrition, and organ damage which all can be attributed to systemic congestion. Increased right atrial pressures reflect the backward transmitted splanchnic congestion leading to multi-organ damage [6]. Mean right atrial pressure was increased in the high CAR group accompanied by decreased renal function. Studies have previously linked increased right atrial pressure with decreased renal function and increased mortality [5, 23].
Increasing evidence suggests that patients in late-stage RV failure due to TR do not profit from TTVr and timing of intervention is essential [24, 25]. Increased right atrial pressures in the high CAR group might generally indicate decompensated patients at procedure and increased focus might be given to pre-procedural decongestion and optimization before procedure. On the other hand, there were no significant differences in peripheral edema at baseline between the CAR groups in this study, indicating clinical euvolemia. This might mean that persistently increased right atrial pressures after recompensation reflect more severe TR and atrial dysfunction in otherwise euvolemic patients.
High CAR was independently associated with increased mortality 2 years after TTVr after adjusting for RV function, renal and liver function, and importantly procedural failure according to TVARC criteria. The increased risk of death independent of the procedural outcome would suggest that patients with high-grade TR and late-stage RV failure might not benefit from TTVr, even if substantial TR reduction can be achieved [24, 25]. Opposingly, patients of the high CAR group with intraprocedural success had significantly reduced mortality during follow-up. This indicates that while patients with high CAR have higher mortality risk, they have a survival benefit when achieving intraprocedural success during TTVr. This effect was not observed in the low CAR group. This study therefore identifies a high-risk subgroup which may lower its mortality risk due to a successful TTVr procedure. On the other side, a very high CAR of 6.85 or more identified patients with a dismal prognosis of only 50% 1-year survival after TTVr. These results suggest a rather conservative approach in patients with very high CAR and careful consideration of other patient characteristics is warranted. However, multicenter studies are needed to generalize these findings.
CAR has been tested in other patient groups and conditions for predictive power of mortality or disease activity [15, 26, 27]. Increased CAR has been associated with increased risk of cardiovascular disease, and has been shown to be a marker for 30-day mortality after transcatheter aortic valve replacement [16, 28]. However, this is the first study evaluating CAR after tricuspid valve repair. Another study has already assessed the nutritional status using the mini nutritional assessment score including albumin as a prognosticator after TTVr [29]. Albumin was also included in a novel risk score predicting mortality in isolated TR [30]. However, these scores neglect low-grade inflammation, which is reflected by combining CRP with albumin in CAR. Further studies should characterize the low-grade inflammation induced by TR and investigate the impact of TTVr on this pathophysiological aspect. Finally, in our supplementary analysis, the TRI-SCORE showed a slightly better AUC than CAR. Compared to the multi-parametric TRI-SCORE, the components of CAR are routinely available in everyday practice and easily calculated. Since adding CAR to the TRI-SCORE in the supplementary analysis led to an increase in predictive capacity, this could be an option to use CAR in addition to established risk scores. The novel multi-parametric TRIVALVE Score predicts mortality and rehospitalization in the 12 months after TTVr, [31] It should be noted that the multi-parametric TRIVALVE score had a slightly worse AUC (0.681) than CAR. However, a direct comparison to CAR is limited due to divergent endpoints and future studies could analyze the combination of CAR and TRIVALVE after TTVr.
Limitations
Limitations of this study include the retrospective and single-center design. Comparative studies evaluating the TRI-SCORE from other centers showed even more morbid patients which were treated by TTVr compared to this study population, and this might influence the generalizability of scores like CAR [4]. Furthermore, this study included a population treated with either T-TEER or TTVA, representing different interventional techniques. However, there was no significant difference between the different types of procedures regarding mortality during follow-up. High sensitive CRP (hs-CRP) is able to detect even lower levels of inflammation and is associated with cardiovascular events and mortality [32]. In this study, only CRP, as a routinely available marker of inflammation, was investigated. Although hs-CRP is more costly, it might improve the sensitivity of CAR and could be investigated in further studies.


Comments (0)