Study design
This dual-cohort analysis utilizes a hybrid approach, supplementing clinical data with Real-World Data (RWD) as epidemiological validation. By design, the study represents a retrospective analysis.
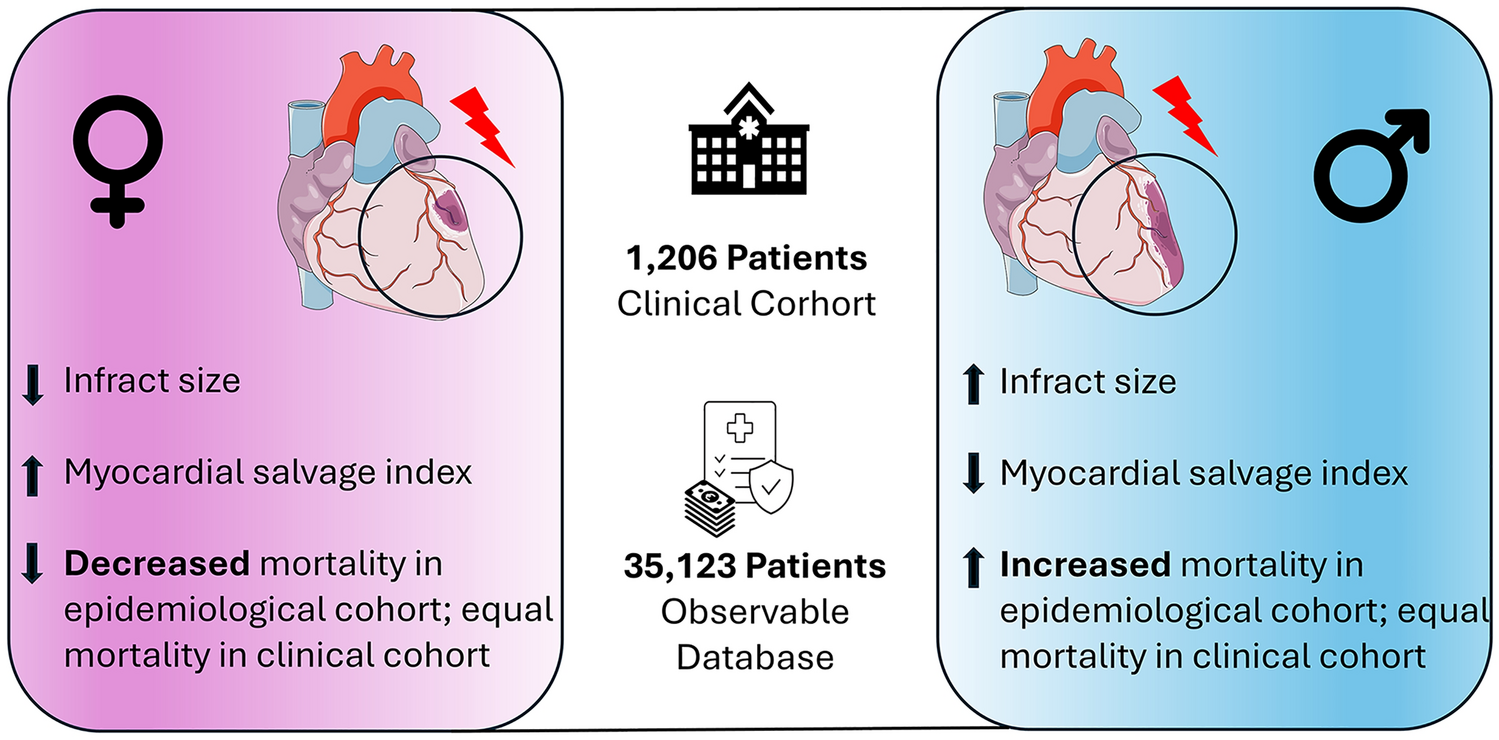
Details of the clinical study patients were described before [14,15,16]. In brief, between January 2002 and December 2007, patients with STEMI undergoing primary percutaneous coronary intervention (PPCI) and serial scintigraphic imaging at two tertiary cardiac care centers (Deutsches Herzzentrum München and Klinikum Rechts der Isar, both Technical University of Munich, Munich, Germany) were included in this study. The diagnosis of STEMI was based on chest pain lasting ≥ 20 min and persistent ST segment elevation ≥ 1 mm in at least two extremity or ≥ 2 mm in at least two chest leads or new onset of left bundle branch block. As reported recently [15], 200 out of 1,406 STEMI patients were excluded because exact time of symptom onset was not clearly documented. Hence, the remaining 1,206 patients were included into this analysis. All patients gave written informed consent for PPCI and imaging procedures.
RWD cohort was derived from observational data collected by the Observational Bavarian Health Insurance Registry (OBSERVABLE). This database is an extensive repository of secondary health claims data provided by the Allgemeine Ortskrankenkasse (AOK) Bayern, a component of the German Statutory Health Insurance system. The OBSERVABLE database includes detailed records from over 1.3 million individuals residing in Bavaria, a state in southern Germany. These individuals are aged 18 years and older and have been diagnosed with atherosclerotic disease between January 1, 2012 and December 31, 2021. The registry contains anonymized patient-level data, which comprises demographic information, diagnoses (coded according to the International Classification of Diseases, 10th Revision, ICD-10), medical procedures, pharmaceutical prescriptions dispensed at pharmacies, and causes of mortality.
For our study, we identified a cohort based on the recorded diagnosis of STEMI, followed by any type of revascularization within 24 h. The cohort was monitored over a five-year period starting from the date of the STEMI to assess clinical outcomes comprehensively. To ensure an adequate assessment of baseline covariates, only those individuals with a minimum of 12 months of continuous enrollment in the database prior to the index revascularization procedure were included. The data covered all levels of care, from tertiary hospitals to outpatient services, thus reflecting a broad spectrum of the healthcare landscape relevant to cardiology. This robust dataset is particularly suited for analyzing clinical outcomes using a mixed-data approach. All used codes can be found in Supplementary Table S1.
Ethical considerations and study conduct
The study protocol was approved by the institutional ethics committee (454/21 S-KH for the first and 2019-50-S-SR for the second cohort) and conforms to the Declaration of Helsinki.
Angiography and PPCI
For the clinical cohort, angiography data were available. The culprit lesion in the infarct-related artery was identified during coronary angiography, based on several angiographic features including the presence of acute occlusion, intraluminal filling defects (or thrombus), ulcerated plaques with contrast-filled pockets protruding into the plaque with or without delayed contrast wash-out, extraluminal contrast, dissection or intraluminal flaps. Coronary artery disease in non-culprit lesions was defined as coronary stenosis of at least 50% lumen obstruction [15]. Left ventricular ejection fraction (LV-EF) on admission (baseline) and after six months was measured on left ventricular angiograms using the area–length method [15]. For periprocedural anticoagulation, unfractionated heparin was administered [15]. The anti-thrombotic regime included an initial loading dose of 600 mg clopidogrel, and aspirin 325 to 500 mg aditionally [15]. Post-procedure, patients received 150 mg clopidogrel until discharge, not exceeding 3 days, mostly followed by maintenance dose of 75 mg/day for at least 1 month. Along with clopidogrel, aspirin 200 mg/day was given indefinitely [15]. Few patients received ticlopidine (250 mg twice/day). In patients presenting with new onset of atrial fibrillation, either aspirin and clopidogrel or aspirin and ticlopidine was combined with phenprocoumon [14].
Measurement of myocardial area at risk and final infarct size using SPECT
In the clinical cohort, 99mTc-sestamibi single-photon emission computed tomography (SPECT) imaging studies were performed as described previously [14,15,16]. SPECT imaging was performed twice in each patient at pre-defined time points. For the first measurement, 99mTc-sestamibi (27 mCi (1000 MBq)) was injected intravenously prior to PPCI. This was followed by imaging 6–8 h afterward to assess the perfusion defect and by that estimate the myocardial area at risk. During a second measurement, 99mTc-sestamibi was injected intravenously again between 7 and 14 days after the PPCI, followed by imaging 6–8 h afterward. Perfusion defects were defined as less than 50% uptake of 99mTc-sestamibi and were expressed as percentage of the left ventricle [14,15,16]. The myocardial salvage index (i.e., relative salvage) represents the proportion of initial myocardial area at risk salvaged by reperfusion therapy and was calculated as initial myocardial area at risk minus final infarct size divided by initial myocardial area at risk [14, 15]. All measurements were performed by investigators unaware of the clinical or angiographic data of the patients [14,15,16].
Laboratory data, medical history and definitions
In the clinical cohort, laboratory measurements were routinely performed daily at the institute of laboratory medicine of our hospital, and data were extracted from patients’ charts up to ten days post-admission. As enzymatic estimate of infarct size creatine kinase myocardial band (CK-MB) and troponin T were measured daily. Peak levels were defined as the highest value obtained during hospitalization. Renal function was evaluated by calculating the creatinine clearance using to the Cockroft–Gault formula.
Study outcomes and follow-up
The primary outcome of the study was the five-year all-cause mortality rate. For both study groups, major adverse cardiovascular events (MACE), a composite endpoint of acute myocardial infarction, stroke and all-cause death, were evaluated as secondary outcomes. Additionally, within the clinical cohort alone, several specific parameters were assessed: the infarct size, the maximum levels of troponin, the myocardial salvage index, and the LV-EF. These measurements were taken at the time of admission and then again at a six-month follow-up.
As a standard practice in our institutions at the time of patient’s recruitment, six months after the index procedure a repeat coronary angiography was scheduled. The six-month angiograms were used for the assessment of the LV-EF at this time point. For the clinical cohort, the follow-up information was obtained by staff members who were not aware of the clinical data via phone calls 30 days after PCI, 1 year after PCI, and yearly thereafter [14, 15]. Data on mortality were obtained from hospital records, death certificates, or phone contact with patients’ relatives or referring physicians [14, 15].
Statistical analysis
Continuous data were presented as mean ± standard deviation (SD) or median with interquartile ranges (25th–75th percentiles) [IQR] and 10th–90th percentiles, depending on the normality of the distribution assessed by Shapiro–Wilk test for normality. These data were analyzed using either Independent Samples t-Test or the Mann–Whitney U test. Discrete variables were expressed as proportions (percentages) and analyzed using the chi-square test. A two-sided P value of less than 0.05 was considered statistically significant. We employed the standardized mean difference (SMD) to compare baseline characteristics between male and female within our epidemiological cohort. By convention, a SMD within ± 0.1 was used to define the achievement of a good between-group balance.
To control for potential confounders between female and male participants, we implemented a nearest-neighbor caliper matching without replacement, based on the log-odds of the propensity score (PSM). The propensity scores were calculated using similar pre-exposure covariates, which encompassed baseline demographics and various cardiovascular risk factors present in both the clinical and RWD cohorts (Supplementary Table S2 + S3), thus rendering the groups comparable. The caliper width was set to 20% of the standard deviation of the propensity log-odds. Survival outcomes for the matched cohorts were visualized using Kaplan–Meier survival curves and plotted over a five-year period. Hazard ratios were calculated using Cox proportional hazards models, including variables, such as follow-up times, censoring indicators, and the allocated treatment group, with sex as the primary predictor.
For statistical analysis and data visualization, we utilized Python version 3.10.9, R-Studio version 4.1.2, IBM SPSS Statistics version 29, and GraphPad Prism 9.


Comments (0)