Participant eligibility
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Providence IRB (approval number STUDY2020000637). All participants were over the age of 18 and a current Providence patient with one or more visits with a Providence provider in the previous 12 months. Participants provided the name and contact information for their primary Providence provider, who would receive the lab report. All racial and ethnic backgrounds were eligible; however, due to limitations in educational and consent materials, initial enrollment was restricted to English or Spanish speakers who could enroll online. Participants were required to have a current, viable email, mailing address, and telephone number. Participants were excluded if they were pregnant, had a history of bone marrow transplantation, or had an active hematologic malignancy.
Participant outreach and recruitment
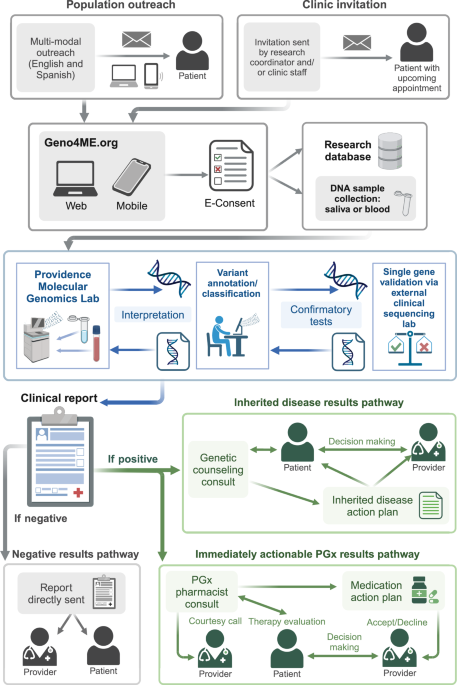
Figure 1 describes the participant process starting from initial outreach. Between March 2021 and April 2023, eligible Providence patients were invited to participate in Geno4ME (https://www.geno4me.org). Participants could return their sample kits until June 30, 2023. There were two invitation pathways: a clinic-centered outreach for assay and process validation in three clinics in Oregon (OR), California (CA), and Washington (WA) (March-September 2021), and a direct-to-patient outreach using stratified random sampling in five states (OR, CA, WA, Alaska (AK), and Montana (MT)) within the Providence system (population outreach) (September 2021 onward). Outreach began in CA and OR in September 2021 due to the large number of eligible patients and expanded to WA, MT, and AK in May 2022.
Clinic-based recruitment involved identifying patients with upcoming appointments. These patients received a MyChart invitation from a research coordinator or clinic staff two weeks before their appointment or a flyer during their visit. To increase participation of underrepresented populations in genomic studies, we used population-level stratified random sampling focusing on patients of Asian, Black, and Hispanic ancestry, Spanish speakers, and Medicaid patients (as a proxy for socioeconomic status and healthcare vulnerability). Recruitment outreach used mail, email, text messages, and auto calls in English and Spanish25.
Enrollment process
Participants could enroll in Geno4ME online using a novel e-consent platform designed by Providence. This platform included genetic testing information, frequently asked questions (FAQ) guides, and a step-by-step consent process with pre-enrollment educational videos (Fig. 1). The platform was the first comprehensive e-consent process of its kind approved by Providence. Participants were asked to create a study account to access the e-consent platform, choose their preferred language (English or Spanish), and sign consent documents. Study accounts allowed participants to answer surveys privately and securely, access their genetic report and consent document, receive post-enrollment education, and change their status regarding future research participation opportunities.
During enrollment, participants completed a brief survey about their personal/family medical history. This information was used to generate a tailored report cover letter for primary care physicians, informing them of participant-reported history that warranted formal evaluation. The responses were not used for variant curation. The survey included questions on race and ethnicity (see Supplementary Table 4), self-reported personal and family history of cancer and cardiovascular disease, and current use of any of the seven PGx medications included in the genetic screen. Personal and family history questions were based on National Comprehensive Cancer Network (NCCN) Guidelines and Heart Rhythm Society (HRS) and European Heart Rhythm Association (EHRA) consensus statements to determine if patients met the threshold for detailed risk assessment and genetic counseling.
Sample collection
Sample collection was divided into two phases: Phase 1 involved both blood and saliva samples for WGS assay validation with a limited number of participants. Phase 2 used mailed saliva collection kits only, designed to be more scalable, easier for participants and clinic staff, and to mirror a true population-based approach. Ultimately, 88.7% of all study participants were part of Phase 2.
Phase 1 sample collection
To validate our Geno4ME assay and processes, Phase 1 involved collecting blood and saliva samples at a clinic encounter by local staff. A phlebotomist at the clinic or a Providence laboratory collected 8–10 mL whole blood in standard EDTA tubes and 5 mL in standard PPT Pearl tubes. Saliva was collected using an Oragene Saliva DNA Collection kit (DNA Genotek) (2 mL). All collection tubes were labeled with participant information as required by CLIA and CAP regulations. Specimens were transferred via courier (in Oregon) or FedEx overnight shipping at room temperature to the Providence Molecular Genomics Laboratory (MGL; Portland, Oregon, CLIA #38D2032720, CAP #8034828). In September 2021, after validating the assay and process, all enrollment channels transitioned to the Phase 2 saliva-based population outreach sample collection workflow.
Phase 2 sample collection
In Phase 2, all enrolled participants received an Oragene Saliva DNA Collection kit (DNA Genotek) sent directly to their residence, auto-generated by our study platform. Participants collected their saliva sample (2 mL) at home and mailed it at room temperature to the Providence MGL using approved regulatory and postage-paid packaging. If a participant’s primary saliva sample failed, they were asked to provide a blood sample at a Providence phlebotomy station. Blood samples were collected in 8–10 mL EDTA tubes and transferred via courier (within Oregon) or FedEx overnight shipping to the Providence MGL.
WGS-based assay workflow and validation process
DNA extraction from blood or saliva was performed using the QIAsymphony DSP Midi Kit on a QIAsymphony instrument (Qiagen). WGS libraries were prepared from 300 to 500 ng of gDNA with the Illumina DNA PCR-Free Prep, Tagmentation kit and sequenced on an Illumina Novaseq 6000. Genomic secondary analysis for the genes included in the Geno4ME test was performed using standard analysis pipelines on the Illumina DRAGEN (Dynamic Read Analysis for GENomics) Bio-IT Platform.
A validation set of 188 DNA samples (119 whole blood, 69 saliva, with 60 paired blood/saliva specimens) from newly enrolled patients, known positives, and control reference materials was used for assay validation along with orthogonal testing at a CLIA/CAP commercial molecular laboratory (Invitae). A training set of 18 DNA samples from the CDC Genetic Testing Reference Material program (GeT-RM) was used in addition to the blood/saliva DNA patient samples for validation of the PGx results41. These 18 samples were sequenced at MGL following the same procedure as the participant DNA samples.
Variant curation and confirmation
Initial variant prioritization and scoring were performed using the Health Insurance Portability and Accountability Act (HIPAA)-compliant Fabric Genomics cloud platform42. For PGx, pre-selected variants were genotyped, and phenotypes were assigned in the Fabric Genomics platform based on Pharmacogenomics Knowledge Base (PharmGKB), Clinical Pharmacogenetics Implementation Consortium (CPIC), and Pharmacogene Variation Consortium (PharmVar) annotations43,44,45. For inherited diseases, single-nucleotide variants (SNVs), multi-nucleotide variants/polymorphisms (MNVs), insertions, deletions, and copy-number variants (CNVs) were automatically annotated and classified using the Automated Variant Classification Engine (ACE) from Fabric Genomics. ACE scores variants based on the 2015 guidelines for variant interpretation from ACMG and the Association for Molecular Pathology (AMP)46, which uses evidence from public databases such as ClinVar47, dbSNP, and gnomAD to classify and prioritize variants.
Variants were initially classified if ACE provided enough ACMG criteria to assign a pathogenic/likely pathogenic (P/LP) or benign/likely benign (B/LB) classification. Variants where ACE could not provide enough criteria and/or those with a ClinVar interpretation of P, LP, conflicting, or not provided were prioritized for manual review. CNV pathogenicity classification was performed based on recommendations by Riggs et al. (2020)48. Prior to curation, variants of interest identified by ACE (i.e., P/LP variants, certain prioritized VUS, and CNVs) were visually inspected using Integrative Genomics Viewer (IGV) for alignment quality and evidence of variant phasing49. Curation and final assignment of these variants were completed in-house by Clinical Scientists using the 2015 ACMG guidelines and the Mastermind literature search engine46,50. Variants classified as P/LP were included in the clinical report, while those classified as VUS or B/LB were not returned to participants. After final review, the presence of P/LP variants associated with inherited diseases was independently confirmed by Invitae using an orthogonal NGS process (Fig. 1).
Geno4ME return of results panel design
As part of Geno4ME enrollment, clinically actionable genetic results were reported back to participants and their designated providers to guide clinical decisions. Study consent required agreeing to the return of results; participants could not “opt out.” While WGS was performed, the data analyzed for the return of results was limited to genes selected for assessing inherited disease risk and PGx. All other genome regions outside the scope of the Geno4ME return of results were bioinformatically masked for the team preparing the clinical interpretation and report.
For inherited diseases, the gene panel included clinically relevant genes with well-established disease associations, especially for cancer and cardiovascular disease, where knowledge of the pathogenic variant warrants medical recommendations. The panel included the 59 genes identified by the ACMG as relevant secondary findings from sequencing (ACMG 59)5, and 18 additional genes with actionable management recommendations by the 2021 NCCN Guidelines for genetic/familial cancer risk (Table 1)20,21.
For PGx, the panel included seven gene-drug pairs selected based on FDA and CPIC guidelines, prescription usage data across the Providence St. Joseph Health (PSJH) system, and race and ethnicity data (Table 2; FDA, Table of Pharmacogenomic Biomarkers in Drug Labeling)51,52,53,54. PGx variants were pre-selected based on the published joint recommendations from the AMP and the CAP, as well as CPIC guidelines. For CYP2C19, both Tier 1 (*2, *3, and *17) and Tier 2 (*4 A, *4B, *5, *6, *7, *9, *10, and *35) alleles were included per AMP/CAP recommendation55. As recommended by the CPIC guideline for warfarin, CYP2C9 Tier 1 alleles (*2, *3, *5, *6, *8, and *11), VKORC1 (c.-1639G > A, rs9923231), CYP4F2 (*3), and the single variant rs12777823 (CYP2C cluster) were initially included56,57.
For the variant analysis, a 5000 bp buffer region on both sides of each gene of both panels was included. For three genes, GREM1, EPCAM, and PMS2, the analyzed regions were expanded further to include large known duplications and deletions58.
Return of results process to participant and provider
Results were electronically returned to participants, their providers, and genetic counselors when appropriate (Fig. 1). Positive inherited disease results were indicated by the presence of any P/LP variant(s) in the 77 panel genes. The I1307K variant within the APC gene was reported as associated with “moderate colorectal cancer” only. VUS, LB, and B variants were not reported for the inherited disease panel. The results report included a cover letter to providers explaining: (1) the study purpose, (2) if any P/LP variant(s) had been identified, and (3) any reported personal or family history of cancer or cardiovascular conditions associated with inherited disease risk, which might warrant further genetic counseling referral (Supplementary Data 1). The report also included links to a Geno4ME provider portal with educational material, including 1–2-page, gene-specific “Just In Time” information sheets summarizing clinical risks, condition management recommendations, and participant next steps (Supplementary Data 2). This portal was created and hosted by study partner and telehealth counseling provider, Genome Medical (GM) (Supplementary Data 3). For participants seen by a GM genetic counselor, providers were sent the participant’s personalized action plan generated during their counseling appointment.
Participants with a positive panel disease result were contacted by a Providence research coordinator by phone and/or email to disclose initial results and arrange a GM genetic counseling consultation appointment. After this visit, participants and their providers received a personalized care plan from the GM genetic counselor. Personalized care plans for hereditary cancer were based on the NCCN guidelines version for Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic as well as Colorectal at the time of return of results and tailored for sex-based risk, screening initiation and frequency, and risk-reducing medication and surgery options as relevant. A clinical note was created following the standard genetic counseling visit format after a complete review of personal medical and family history. Participants with negative results but a positive personal or family history on screening questions received a cover letter recommending further risk evaluation. For cardiovascular disease, recommendations were based on AHA guidelines for hyperlipidemia, cardiomyopathy, and rhythm disorders. Participants with a potentially actionable PGx genotype/phenotype for drugs reported at enrollment were offered a pharmacist consultation. Following the consultation, any recommended medication changes were shared with their provider. The Geno4ME provider portal also included “Just In Time” clinical decision support material based on CPIC guidelines for the seven gene-drug pairs.
If the participant did not respond after six outreach attempts (phone and/or email), results were automatically provided through MyChart and their Geno4ME participant portal. The participant was then given resources to schedule genetic counseling for a personalized care plan in the future.
Research data management and biorepository
In addition to the Geno4ME clinical report, participants consented to the storage and approved researchers’ use of aggregate de-identified data to support research into genetic disease risks and clinical, family history, health behavior, and social risk factors. Upon enrollment, each participant was assigned a unique Subject ID Number by Providence’s HIPAA-compliant, cloud-based platform for patient education, engagement, and consent. Geno4ME resources (processed WGS data including binary alignment map [BAM] and variant call format [VCF] files, survey responses, and clinical EHR extracts) were de-identified, tagged with the MPT-generated Subject ID Number, and stored in an encrypted cloud-based infrastructure.
Statistical analysis
Chi-square tests of independence were performed in R version 4.3.1 to assess associations between categorical variables59. Where race and ethnicity were analyzed as a combined variable, the “Other” racial and ethnic category was excluded because of too few instances. Post hoc analyses of standardized residuals with a Bonferroni correction were conducted where needed to further characterize any significant associations using the “chisq.posthoc.test” R package60.

Comments (0)