HF is associated with significant morbidity and mortality. Results from an observational/longitudinal cohort study (EVOLUTION-HF) (n = 73,763 American adults) experiencing their first event of hospitalization for HF (HHF) showed that the most common reason for rehospitalization within 12 months of hospital discharge was another HF episode; the all-cause death (in-hospital) event rate for this group was 10.3 per 100 patient years [1].
In addition, the prevalence of CKD is also increasing in the United States. Currently, approximately 35.5 million American adults have CKD and approximately 808,000 Americans were living with end-stage kidney disease (ESKD) in 2020 [2]. Furthermore, globally, 42–53% of people with HF have comorbid CKD [3], representing a significant health and economic burden. For example, when comparing the annualized medical cost for comorbid CKD-HF vs. CKD only (based on 2016 or 2017 patient data from Kaiser Permanente Northwest), the annualized mean medical cost for comorbid CKD-HF is 2-to threefold higher than the cost for CKD only, even when accounting for patients with stage 5 (ESKD) CKD [4]. Thus, effective prevention and treatment strategies for both CKD and HF in the United States is of ongoing importance, both for improving individual quality of life and for reducing healthcare costs.
A chronic inflammatory state in CKD and HF
There are several pathophysiologic mechanisms and risk factors that lead to the development of CKD and HF. Metabolic derangements that occur in diabetes and hypertension cause a prolonged inflammatory state [5]. This inflammatory state may cause endothelial cell dysfunction, hemodynamic dysregulation, oxidative stress, fibrosis, and vasoconstriction [6,7,8,9]. After initial compensatory responses, such as glomerular hyperfiltration in the kidneys, the heart and kidneys eventually lose structural and functional capacity. The filtration efficiency of the kidneys decreases that can be measured clinically as a reduction in the estimated glomerular filtration rate (eGFR) [10]. Structural kidney damage can be estimated clinically by assessment of albuminuria via the urine albumin-to-creatinine ratio (UACR) [10]. Some of the effects of kidney dysfunction include an increase in the volume of waste products in the blood, which can damage the heart, and hypertension due to sodium dysregulation [11, 12]. In the heart, the effects of sustained proinflammatory processes result in ventricular hypertrophy, fibrosis, and damage to the microvasculature supplying the heart, which may manifest as reduced cardiac output [11, 12]. As a result of reduced cardiac output, organs such as the kidneys and the liver may receive a reduced oxygen supply.
Preventing CKD and HF
Given the significant public health and economic burden of CKD and HF, it is important to implement strategies to prevent both conditions. Common risk factors for CKD and HF include obesity, diabetes, and hypertension [13, 14]. Additionally, having CKD is a risk factor for developing HF, and having HF is a risk factor for CKD [12, 14]. Patients may also have albuminuria, which increases the risk of cardiovascular disease (including HF) and cardiovascular mortality [15]; and, a reduced eGFR, which increases a person’s risk of death, cardiovascular events, and hospitalization, independently of known risk factors [16].
Such bidirectional heart–kidney activity for incident disease is consistent with the physiologic interconnectivity of the heart and kidneys [11, 12]. Indeed, the term CKM syndrome is used to describe a multisystem disorder attributed to the intricate connections between obesity, diabetes, CKD, and cardiovascular disease, including HF [17]. CKM syndrome includes those at risk for cardiovascular disease and those with existing cardiovascular disease, and so not only highlights the interconnectivity of the heart and kidneys but also the significance of metabolic disorders such as diabetes as a factor in the development of and progression of CKD and HF [17].
The principal way of preventing the development of both HF and CKD is having a healthy lifestyle throughout the lifespan [13, 14, 18]. Prevention of CKD in individuals with diabetes includes maintaining a blood glucose A1C target below around 7%, and achieving optimal blood pressure (less than ~ 130/80 mmHg) as well as lipid targets [19, 20]. Maintenance of such targets may necessitate taking evidence-based medications, such as metformin (alone or in combination) for A1C, a statin for lipid control, and/or an ACEi or an ARB for blood pressure control [20, 21]. These preventative approaches also apply in the absence of diabetes in individuals who are still at risk of HF/CKD.
For those at continued risk of HF (stage A), or with pre-HF (stage B, asymptomatic), preventing development of symptomatic HF should be a priority. According to HF and CKD clinical practice guidelines, patients at risk for HF or CKD should be considered for natriuretic peptide-based biomarker screening for HF and UACR and eGFR screening for CKD [10, 22]. In addition, those with T2D and cardiovascular disease, or who are high risk for cardiovascular disease (placing them at risk for HF), should be considered for a sodium-glucose cotransporter 2 inhibitor (SGLT2i) to reduce their risk of developing HF (class 1 recommendation) [22]. Such patients should continue to adhere to lifestyle modifications and management strategies. A similar recommendation for SGLT2i in HF prevention is also included in European Society of Cardiology (ESC) guidelines (class/level 1 A), and these guidelines also include a recommendation for finerenone for patients with CKD and T2D to reduce their risk of HHF [23]. Asymptomatic individuals with structural and/or functional abnormalities (pre-HF, or stage B) should take an angiotensin-converting enzyme inhibitor (ACEi) (or an angiotensin receptor blocker [ARB] if ACEi intolerant and a recent myocardial infarction) plus a β-blocker if their left ventricular ejection fraction (LVEF) is ≤ 40%, and they should continue on lifestyle modifications and management strategies (class 1 recommendation) [22]. Final drug treatment choices for those at risk or with pre-HF depends on multiple factors, such as drug tolerability, comorbidities, contraindications, patient preference, and drug availability. Treatment recommendations for CKD are based on eGFR, UACR (or proteinuria), cardiovascular risk, and CKD progression risk [10]. As for HF prevention recommendations, lifestyle modifications and medication optimization for comorbid conditions are recommended for CKD [10].
Symptomatic HF
The three main HF subtypes based on ejection fraction (EF) are HF with a reduced EF (HFrEF [LVEF, ≤ 40%]), HF with a mildly reduced EF (HFmrEF [LVEF, 41–49%]), and HF with a preserved EF (HFpEF [LVEF ≥ 50%]) [22]. Patients with an HFrEF diagnosis should continue with lifestyle modifications plus class 1 guideline-directed medical therapy recommendations consisting of an angiotensin receptor–neprilysin inhibitor (ARNi) or a renin–angiotensin–aldosterone system inhibitor (RAASi), a β-blocker, an MRA, an SGLT2-i, and a diuretic as needed, with dose adjustments and drug alternatives considered according to tolerability and contraindications [22].
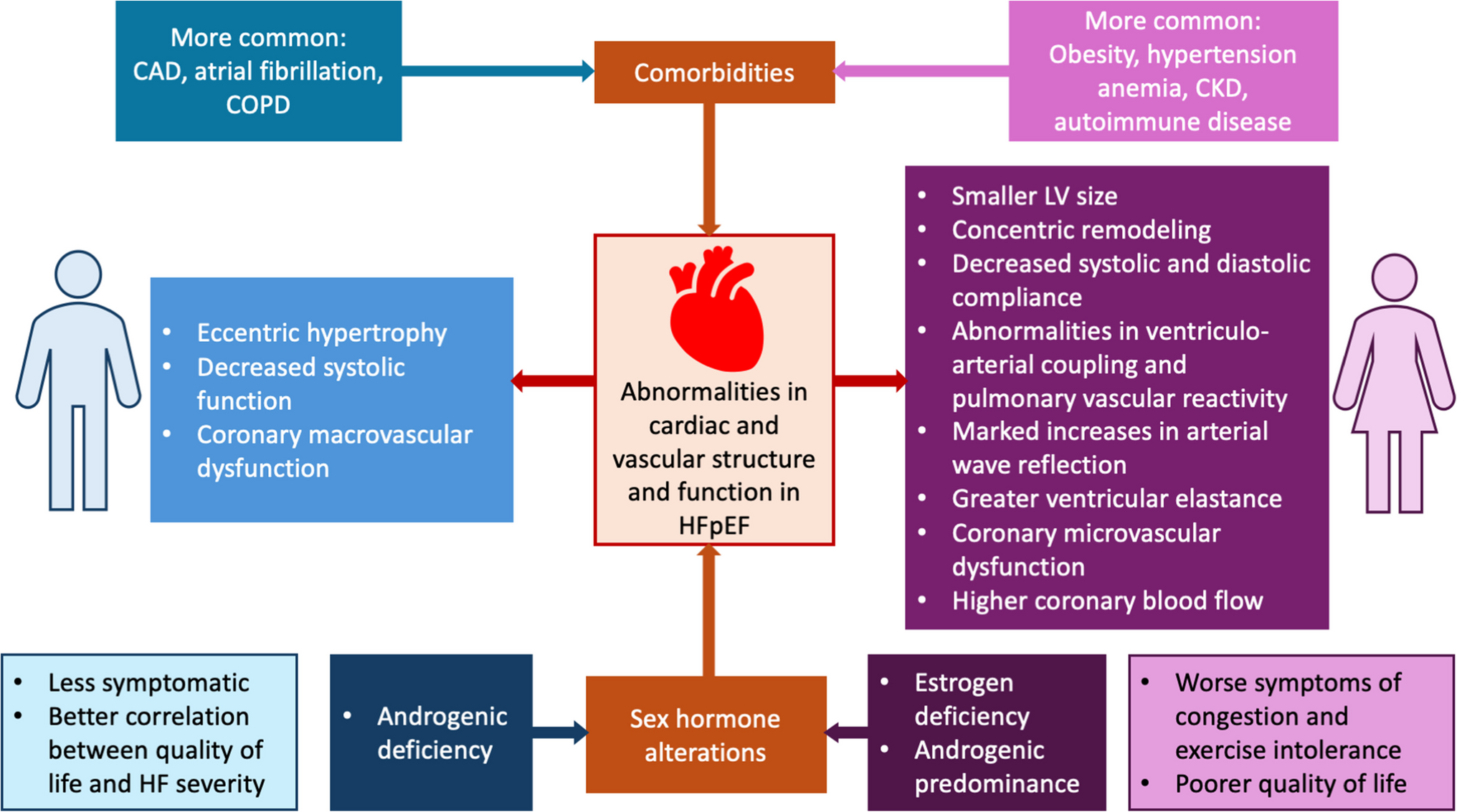
HFpEF is increasing in prevalence (at least 50% of HF cases in the United States [24]) and is more common in older people, women, individuals with diabetes, those with obesity, and those with atrial fibrillation (AF), hypertension, and/or kidney dysfunction [25]. Compared with HFrEF, there are fewer classes of medical therapy definitely proven to improve outcomes in HFmrEF or HFpEF. SGLT2is are part of the foundational therapy for patients with HFpEF in the absence of absolute contraindications and have a class 2a–level recommendation by the AHA/American College of Cardiology (ACC)/Heart Failure Society of America (HFSA) for use in this HF subpopulation [22]. SGLT2is are also included as class 1 recommendations in the ESC guidelines (2023 focused update) for HFmrEF and HFpEF [23]. ARNi, MRAs and ARBs are also included in the AHA/ACC/HFSA recommendations for HFpEF but these are class 2b–level recommendations [22]. Blood pressure management and use of diuretics, as needed, are also strongly recommended by AHA/ACC/HSFA for the HFpEF population [22]. These recommendations for symptomatic HF do not stipulate what to do if a patient also has CKD, but the treatment approach used will likely consider factors such as pretreatment and ongoing kidney function, serum potassium, comorbidities, and current medications.



Comments (0)