
Remember me


We are currently experiencing the advent of biologics in cardiovascular medicine. Recent scientific research has focused on peptides, i.e., short chain of amino acids, as well as nucleic acids, particularly microRNAs (miRNAs), as promising therapeutic agents for a multitude of diseases. Accordingly, growing evidence shows that miRNAs play an important role in the onset and progression of cardiovascular disease [1, 2]. Although several miRNAs have emerged as promising therapeutic candidates in cardiovascular medicine, the majority of clinical trials are focusing on circulating miRNAs as diagnostic or prognostic biomarkers. The use of miRNA antisense as therapeutic for heart disease is limited to only one active clinical trial (NCT05350969). The reason for that is related to the knowledge of the multi-target effect of miRNAs potentially inducing unwanted off-target side effects such as thrombocytopenia or severe immune response [2]. Despite their promising potential, delivering these molecules preferentially into cardiomyocytes remains a significant challenge, further complicated by their instability and rapid degradation in the body. While chemical modifications can enhance stability, as demonstrated with miRNA antisense, achieving the right balance between efficacy and safety remains challenging for synthetic miRNA mimics. Currently, cardiac delivery of biologics in large mammals requires invasive approaches and their enrichment at the heart strongly varies with the route of administration, e.g., intramyocardial injection, intracoronary infusion, or carrier used, e.g., nanoparticles or viral vectors [3]. For instance, adeno-associated viruses (AAVs), typical harmless viruses used as drug-carriers, have been adopted but are difficult to direct to target individual tissues, and they simply do not work in up to 40% of people because they have already been exposed to them in life and they produce antibodies against them [4]. In addition, prolonged, uncontrolled, and persistent expression of delivered therapeutics can be harmful and potentially lethal [5]. Genotoxicity may arise from rare viral vector integration into the genome [6]. Intramyocardial injection overcomes blood interaction and the endothelial barrier, while obviously needle injury is an important concern. Moreover, the volume injected can be a determinant of myocardial leakage or myocardial embolization and plugging.
In summary, the lack of an efficient delivery system capable to allow preferential cardiac uptake, controlled drug release, low toxic side effects, and low-dose administration remains a major issue for the translatability of novel therapeutic compounds.
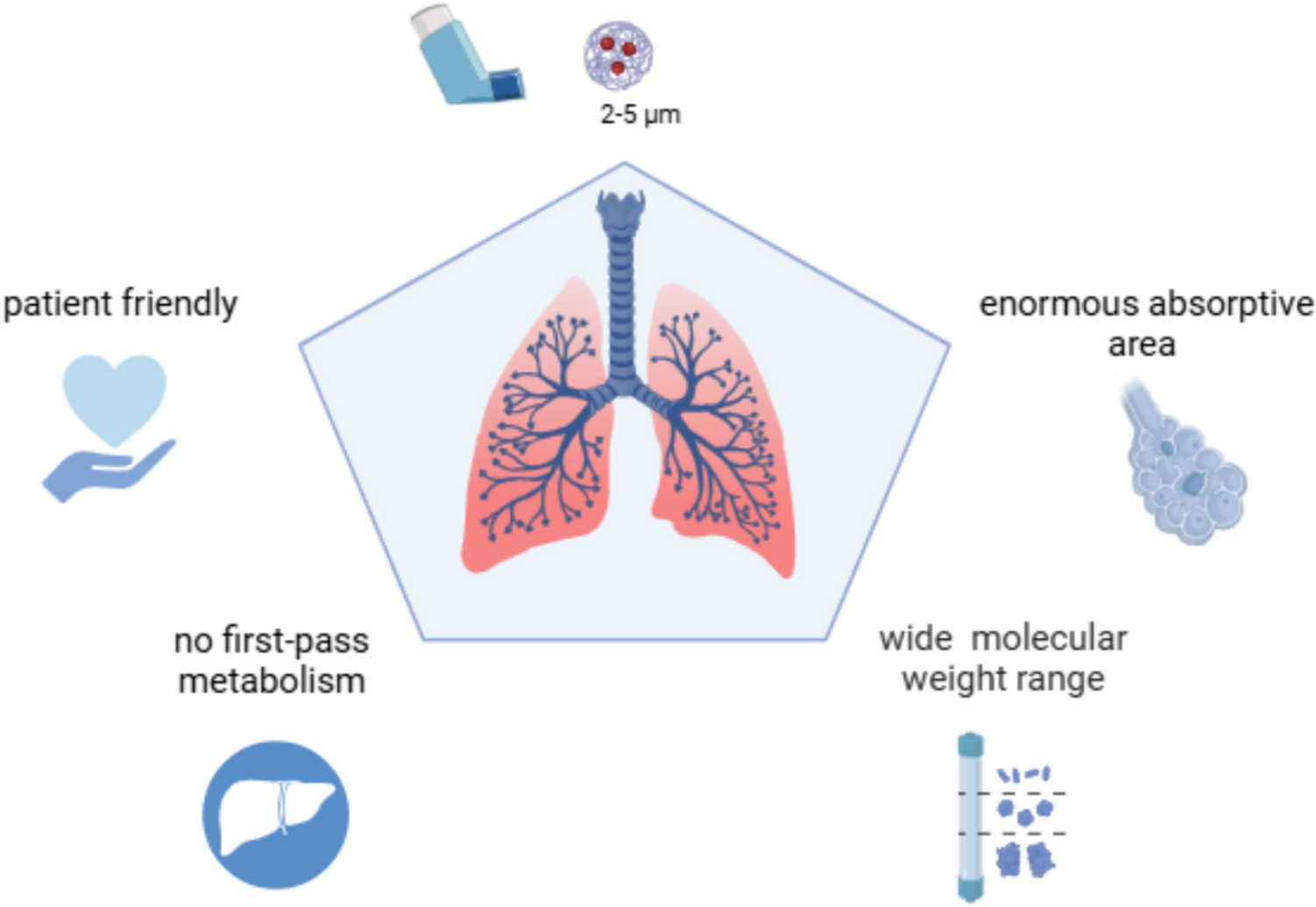
Inhalation for systemic delivery of biologicsInhaled drugs are well established for the treatment of lung-disease, in particular asthma and chronic obstructive pulmonary disease [7]. The idea of applying the inhalation route for treating diseases beyond the lung has been thoroughly explored as it offers several advantages, as summarized in Fig. 1: (i) It is patient friendly, while (ii) directly delivering the therapeutic compound to the systemic circulation, therefore bypassing the first-pass metabolism in the liver [7]; (iii) it is suitable for a wide range of substances from small molecules to very large proteins [8], given the (iv) enormous lung surface with a easily permeable membrane such as the alveolo-capillary membrane. However, previous attempts to leverage this administration route have mostly been disappointing. The long-term use of inhalable insulin for diabetic patients has been documented to induce wheezing and bronchoconstriction and, potentially, gradual loss of lung function [9]. Inhalable levodopa showed promising results in different clinical trials for Parkinson’s disease, but again the most common adverse event was bronchospasm, which was found in approximately15% of patients in the SPAN-PD trial [10].
Fig. 1
Major advantages of pulmonary drug delivery for biologics
With the growing relevance of peptides and miRNAs in the pharmaceutical industry, there is a new wave of significant research and development interest in exploring less-invasive or non-invasive methods for the systemic delivery of biologics, such as inhalation [11]. The development of biologics for inhalation presents several challenges, including proper deposition and distribution in the deep lungs, and the complex permeation through the pulmonary surfactant and the alveolocapillary membrane, all while avoiding resident macrophages and ubiquitarian enzymes [11]. Several inhalable formulation and devices have therefore been developed in the past decades with the aim of enhancing pulmonary drug deposition, and dry powder (dp) inhalers have emerged as the preferred method for delivering inhalable biologics, because of the stability of dp-formulated biologics for storage [12]. To enable the pulmonary delivery, formulating effective drug powders is essential. Most inhalable drug powders consist of particulate carriers, with various synthesis methods—such as spray drying, milling, and freeze-drying—allowing for optimization of formulation parameters. Early research established that characteristics such as particle density, size (preferentially in the range of 2–5 µm), porosity, and charge significantly influence lung deposition and drug absorption, boosting the clinical translation of several formulations for clinical use [11].
Overall, the development of inhalation formulations for biologics targeting organs other than lungs requires a substantial paradigm shift for the accomplishment of a complete preclinical package in terms of pharmacokinetics, pharmacodynamics, and toxicity studies. The most obvious example is related to the peak plasmatic concentration of an inhaled compound, e.g., COPD or asthma spray, which is rather seen as a drug spill-over to be avoided. Indeed, these drugs should exert their effect only locally, i.e., in the lungs. On the contrary, inhaled drugs for systemic administration are supposed to exert their on-target effect shortly after hitting the systemic circulation, avoiding the trap of type II alveolar epithelial cells, i.e., macrophages, in order to minimize any deposition and related inflammatory reactions in the lungs. Furthermore, toxicity studies are of paramount importance in order to detect early signs of airways hyperreactivity related to a novel formulation, especially after long-term exposure to daily inhalation. Challenges related to delivering biologics via the inhaled route are summarized in an excellent overview published in 2021 as a result of a cross-industry working-group survey [13].
Building on these challenges, understanding the underlying chemical principles of inhaled biologics and their formulation strategies is essential to optimizing therapeutic outcomes. The development of inhaled biologics requires careful consideration of their chemical and physicochemical properties, including molecular weight, solubility, and stability during aerosolization. Synthetic peptides and nucleic acids, for example, often require encapsulation in nanocarriers to protect them from enzymatic degradation and facilitate pulmonary absorption, as these biomolecules are typically unstable in the extracellular lung environment [11, 12]. Small molecules, depending on their physicochemical traits, can be formulated as dry powders or solutions, with excipients enhancing dispersibility and lung deposition [12]. Both conventional drugs and experimental biologics have been evaluated for inhalation delivery; while conventional drugs may rely on straightforward formulations, novel biomaterials often demand advanced engineering to ensure bioavailability and tissue targeting [13].
Dosing for inhaled biologics must be carefully optimized to ensure sufficient systemic exposure while minimizing local pulmonary side effects [14]. Unlike oral or intravenous routes, inhalation allows for lower doses due to rapid alveolar absorption and avoidance of hepatic first-pass metabolism. However, factors such as particle size, deposition efficiency, and mucociliary clearance can significantly influence bioavailability and must be further optimized in patients with pathological lung conditions such as pulmonary congestion. Tailoring dose delivery through patient-adapted inhalation devices and consistent dry powder performance will be crucial for maintaining therapeutic exposure across patient populations and should be accounted for during dose selection and formulation development.
Cardiovascular Inhalation as a novel therapeutic paradigm.
Among the potential organs to target via inhalation, the heart has emerged as a promising candidate due to the growing number of novel therapeutic biologics for cardiac diseases [15] and the lack of safe, effective delivery methods for targeted administration [3]. Here, we introduce the term cardiovascular inhalation to describe the novel approach of using inhaled therapeutics to target the heart. Although still in its early stages, this concept is attracting significant attention for its potential in various therapeutic applications [16].
To fully exploit the potential of cardiovascular inhalation, careful selection of appropriate drug candidates is critical. The selection of therapeutic candidates for cardiovascular inhalation therapy requires a strategic evaluation of several key parameters. Molecules must exhibit adequate physicochemical stability during aerosolization and resistance to enzymatic degradation within the lung environment. Furthermore, they should demonstrate sufficient permeability across the alveolar-capillary barrier and favourable pharmacokinetics for systemic or targeted cardiac uptake. Candidates such as short peptides, RNA-based molecules (e.g., miRNA mimics), and small hydrophilic drugs are particularly suitable due to their size, modifiability, and established preclinical efficacy. In addition, drugs with well-characterized mechanisms of action in cardiac pathophysiology provide a rational basis for translational development via inhalation. Ultimately, the goal is to identify compounds that balance lung safety, systemic bioavailability, and cardiac selectivity, either through inherent properties or via nanocarrier-based targeting strategies [11, 16].
In the mammalian circulatory system, blood from the lungs flows directly to the heart via the pulmonary vein after gas exchange. This direct pathway presents a unique opportunity to deliver peptides or miRNAs via inhalation, provided that an efficient carrier facilitates alveolar transcrossing, protects the biologics from plasmatic degradation, and ensures targeted cellular internalization. This process, which we have termed the lung-to-heart administration route [17], leverages the pulmonary circulation for direct cardiac access. However, a primary technical challenge lies in achieving an optimal formulation size: while particles in the 3–5-µm range are needed to reach the deep lung, avoiding direct exhalation, further reduction to < 2 µm is necessary to cross the alveolar-capillary barrier and ensure effective delivery to the heart [13]. An ideal dp formulation consists then of microparticles embedding the drug-loaded nanoparticles (NanoInMicro technology, NIM).
Nanocarriers are needed for cardiovascular inhalationFigure 2 summarizes the lung-to-heart journey. After reaching the deep-lung, the dp microparticles need to dissolve within the surfactant in the alveoli and release the nanoparticles, which translocate into the bloodstream [17]. Nanoparticles (NPs) provide a strategy for an efficient, controlled, and safe drug-delivery. Indeed, NPs can potentially bind and deliver a large plethora of agents including peptides and miRNAs, protecting them from degradation and controlling drug release. Most inhaled nanoparticles tend to localize in the alveolar region, where they release their therapeutic payload gradually. Current research in nanoparticle-based inhalation therapies focuses on reducing adverse effects, improving treatment efficacy, and refining drug delivery specifically to lung tissues. Advanced nanoparticle platforms for inhalation-based delivery have been comprehensively characterized in a recent review [18].
Fig. 2
Lung-to-heart journey: from left to right: (i) oral inhalation, (ii) microparticles dissolve within the surfactant in the alveoli, (iii) translocation in the systemic circulation of the loaded nanoparticles, and (iv) the drug is entering the cardiomyocytes via endocytosis and released intracellularly via an effective endosomal escape
Overall, three major classes of inhalable NPs have emerged in recent years, including polymeric nanoparticles (PNPs), lipid-based nanoparticles (LNPs), and inorganic nanoparticles (INPs). PNPs, such as those composed of chitosan, poly(lactic-co-glycolic acid) (PLGA), or polyethyleneimine (PEI), offer controlled drug release and protection from enzymatic degradation while exhibiting favorable physicochemical properties for inhalation. Chitosan-based nanoparticles, for instance, demonstrate mucoadhesive properties that enhance pulmonary retention and absorption due to their interaction with mucus glycoproteins and positive surface charge, which promotes epithelial uptake [19]. PLGA-based formulations, on the other hand, have been optimized for inhaled therapy via tailoring the porosity [20] as well as combining the high lung deposition advantage of microparticles with a nanoparticle in microparticle delivery system (NIM), which can quickly release free nanoparticles after lung delivery, so as to effectively overcome the lung clearance barrier and achieve good systemic therapeutic effect [21]. Their advantages for inhalation include biodegradability, controlled release, and ability to encapsulate both hydrophilic and hydrophobic drugs.
LNPs, including solid lipid nanoparticles (SLNs) and nanovesicles such as liposomes, have been widely investigated due to their ability to efficiently encapsulate bioactive molecules and facilitate cellular uptake [8]. Notably, exosome-based LNPs have gained attention in cardiovascular research for their role in delivering miRNAs and proteins involved in cardioprotection and tissue regeneration [22]. Exosomes are nanoscale extracellular vesicles of endosomal origin, secreted by progenitor cells, and several studies have demonstrated the dose-dependent efficacy of exosome therapy in improving cardiac function [23, 24]. Building upon this evidence, fibroblast-derived cardioprotective exosomes have recently been shown to ameliorate cardiac remodeling and improve function in preclinical heart failure, offering a scalable, noninvasive therapeutic approach [25]. In contrast, NPs composed of synthetic polymers and micelles often suffer from scarce biocompatibility, low encapsulation efficacy, and slow biodegradability [26]. For cardiac applications, it is well established that nanoparticle systems must meet specific physicochemical criteria—namely, colloidal stability, controlled size and shape, and a negatively charged surface—to avoid interference with cardiomyocyte function [27, 28].
Among INPs, negatively charged calcium phosphate nanoparticles (CaP-NPs) are characterized by high biocompatibility and pH-sensitive stability, which facilitates the release of their load in biological acidic environments (i.e., endosomes or lysosomes) [28]. The CaP-NPs have a platelet-like shape with a solid diameter of 20–50 nm and a hydrodynamic mean diameter < 200 nm, thus being in the perfect size for the inhalation route. The mechanism of cell internalization follows the conventional physiological process of clathrin- and dynamin-mediated endocytosis, thus without inducing toxicity or apoptosis. Moreover, the complete dissolution in Ca2+ and \(}_^\), the main constituents of CaP-NPs, prevents unwanted NP accumulation in cells and tissues. As shown by Di Mauro et al., CaP-NPs do not interfere with functional properties of the cardiomyocytes both in vitro and in vivo [28]. Following on this development, Miragoli et al. demonstrated the feasibility of using CaP-NPs and inhalation as an approach for delivering therapeutic peptides to the heart in vivo in mouse, rats, and pigs [29, 30]. Recently, Modica et al. verified the therapeutic application of these CaP-NPs as carriers of the miR133a mimic in a pressure-overload heart failure (HF) mouse model [31]. Finally, Quarta et al. produced a microparticulate dp product out of the peptide-loaded CaP-NPs to be inhaled from a commercially available inhalation device (e.g., DPI), thus improving their stability and making the dose control more predictable [32]. In their design of experiment, the formulation was achieved by spray-drying nanoparticle dispersions in an aqueous solution of mannitol, a common polyalcohol already used in the clinical treatment of cystic fibrosis patients. The resulting formulations were defined as the lung-to-heart nano-in-micro-technology (LungToHeartNIM).
Comments (0)