In recent years, the use of remote monitoring for patients with HF has expanded dramatically with the increased availability of advanced technology. Unfortunately, remote monitoring approaches have not demonstrated adequate sensitivity for detecting worsening HF events and improved clinical outcomes have been difficult to demonstrate [7,8,9]. For example, the sensitivity of daily weight change in predicting a worsening HF event is on the order of 10 to 20%. In one study, daily weight change (3 pounds in one day or 5 pounds in 3 days) demonstrated a sensitivity of 22.5% and a false alert rate, also called an unexplained detection rate, of 4.3 meaning that 4.3 alerts per year were not associated with a subsequent HF event [10]. Thus, an unmet need in HF management is for remote monitoring technology that provides high levels of accuracy (i.e., high sensitivity and low false alert rates) for detecting HF events and subsequently results in improved patient outcomes.
While remote telemonitoring for chronic HF events is an important unmet need, guidance on their use is unavailable from professional cardiology associations likely attributable to the lack of high-quality research in this area. In a 2023 update of the European Society of Cardiology (ESC) guideline for managing acute and chronic HF, little mention is made of remote monitoring [11]. A 2022 update of guidance for HF management from the American Heart Association, American College of Cardiology Foundation, and the Heart Failure Society of America (AHA/ACCF/HFSA) acknowledges the potential of remote monitoring for HF management, but found little support for use of remote monitoring in this population [12].
Clearly, what is considered standard of care outpatient HF monitoring today (i.e., monitoring of patient symptoms, vital signs, and daily weights) has proven insufficient and resulted in few avoided hospitalizations. While some single- and small multi-center center observational experiences have reported success with this approach, large and adequately powered randomized controlled trials have consistently failed to demonstrate benefit (TELE-HF, TEN-HMS, BEAT-HF) [13,14,15]. For example, the Telemonitoring in Patients with Heart Failure (TELE-HF) trial—a U.S. National Institutes of Health-sponsored multicenter randomized controlled trial of telemonitoring versus usual care—showed that telemonitoring did not improve outcomes [14]. Telemonitoring was accomplished by using a telephone-based interactive voice-response system that collected daily information about symptoms and weight that was reviewed by the patients’ clinicians. A total of 1653 patients were randomized. The primary end point was readmission for any reason or death from any cause within 180 days after enrollment. Secondary end points included hospitalization for heart failure, number of days in the hospital, and number of hospitalizations. There were no significant differences between the two groups with respect to the primary endpoint, the individual components of the primary endpoint, or any of the secondary endpoints.
The Better Effectiveness After Transition–Heart Failure (BEAT-HF) study used a more comprehensive and aggressive telemanagement strategy than TELE-HF but proved to be equally ineffective [15]. The intervention consisted of three components implemented by registered nurses: predischarge HF education, regularly scheduled telephone coaching, and home telemonitoring of weight, blood pressure, heart rate, and symptoms using Bluetooth-enabled devices. Devices automatically transmitted data back to central servers for telemonitoring review by telephone call center study nurses and prompted protocolized telephone interventions by these nurses. A total of 1437 patients were randomized to this intervention versus usual care in this multicenter randomized controlled trial. Despite the intensity of this approach, the intervention did not significantly reduce readmissions for any cause 180 days after discharge (primary endpoint) or 30-day readmission or 30-day and 180-day mortality (secondary endpoints) (Ong et al., 2016).
The failure of these studies suggests that we are measuring the wrong signals of heart failure clinical status. This issue has been discussed extensively elsewhere, leading to the conclusion that accurate assessment of hemodynamic or pulmonary congestion (i.e., changes in intracardiac or pulmonary artery pressure or lung fluid content) may be a prerequisite to success in HF remote monitoring [9, 16].
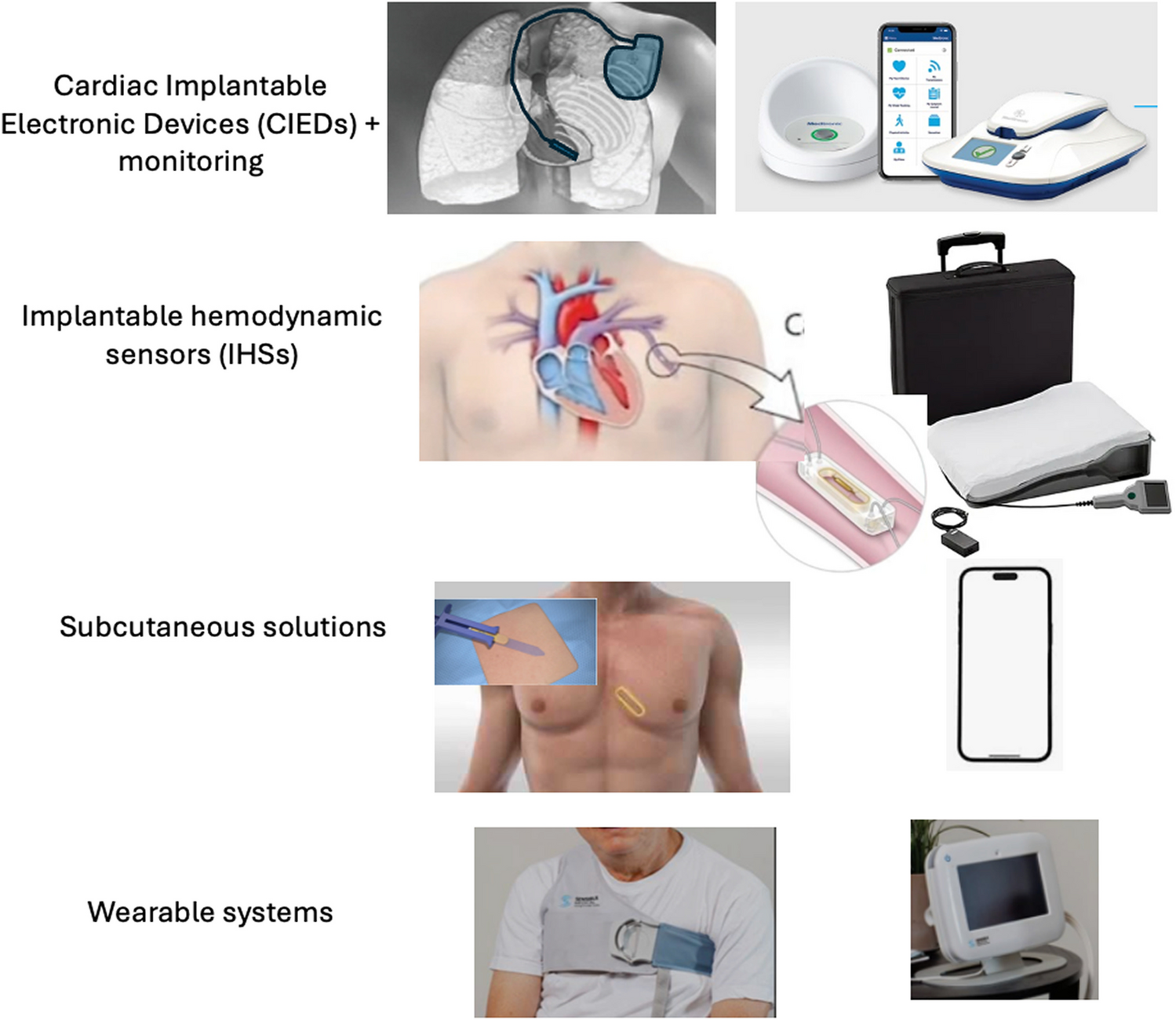
While implantable hemodynamic monitors represent a proven approach that results in reductions in the risk of HF hospitalizations, their expense and invasive nature may limit their use in the broad heart failure population. Remote monitoring systems which provide non-invasive, intuitive, and relatively low-cost options to accurately monitor and treat patients with chronic HF are needed. Such systems may provide an alternative to implantable devices for many patients and perhaps a compliment to implantable devices in others. An example of how new technology advancements can incorporate the learnings noted above and leverage both traditional speech signal processing, statistical-based and AI-assisted approaches to develop and optimize the performance characteristics of HF monitoring systems is discussed below.



Comments (0)