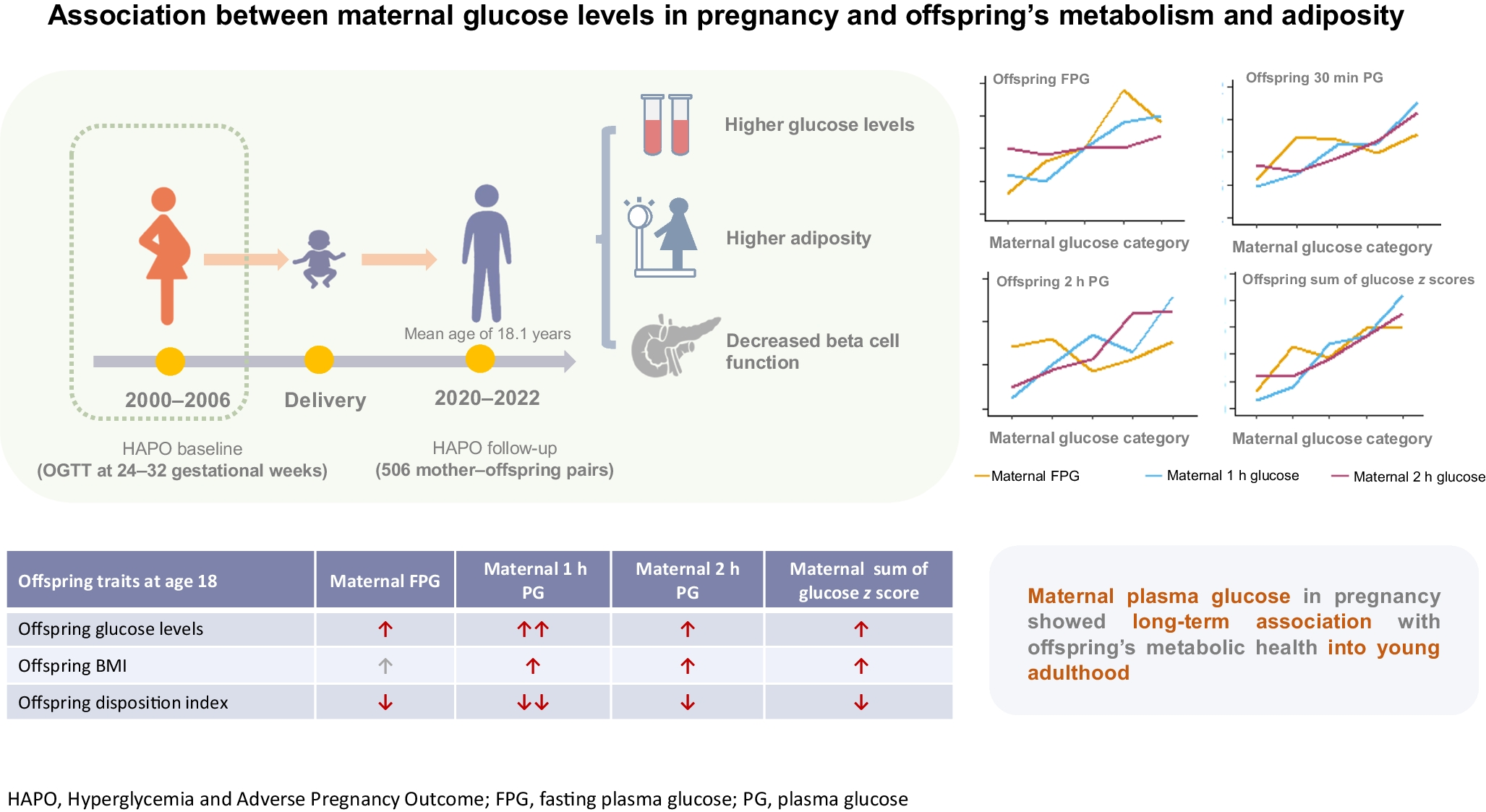
In this 18-year birth cohort study, our main findings include a consistent association between maternal plasma glucose in pregnancy, analysed as a continuous variable, and offspring’s metabolic outcomes and adiposity traits in early adulthood. Although offspring of mothers with GDM showed trends towards higher metabolic risks, not all associations reached statistical significance. We also observed a significant association between maternal plasma glucose levels during pregnancy and offspring’s indices of insulin secretion evaluated in early adulthood.
Long-term associations of maternal hyperglycaemia: comparisons with other studies
The long-term association between maternal glucose levels and offspring’s health outcomes has been well documented across different populations and time periods [15]. Evidence linking maternal hyperglycaemia during pregnancy to children’s metabolic health was first documented in the Pima Native American population, where maternal hyperglycaemia during pregnancy was related to fetal programming in a population with notably high rates of obesity and type 2 diabetes [16, 17]. These early findings have since been confirmed by studies in diverse populations, including in Hong Kong cohorts [18].
Regarding glycaemic parameters, our study revealed that maternal plasma glucose in pregnancy, particularly 1 h glucose levels, significantly influenced offspring’s glucose metabolism in early adulthood. While the associations with 1 h glucose levels were particularly strong, the relationships with fasting glucose were relatively weak. This might be partially explained by the larger variability and lower intra-individual consistency in fasting glucose values than in other glycaemic traits, as demonstrated by recent continuous glucose monitoring studies in populations without diabetes [19]. Such inherent variability in fasting glucose measurements could potentially underestimate the true associations between maternal fasting glucose levels and offspring’s outcomes. This finding extends the findings of previous studies showing that offspring exposed to maternal hyperglycaemia face IGT and insulin resistance that persists into adolescence [20]. Our findings provide important clinical insights, highlighting that the impact on offspring’s health occurs across the entire glycaemic spectrum, rather than only above the current diagnostic threshold [21]. Notably, these patterns persisted after adjusting for maternal and offspring’s BMI, suggesting an independent association between maternal glucose levels and offspring’s metabolic health. As demonstrated by McIntyre et al, conventional diagnostic criteria show poor performance in specifically identifying individuals at risk, with receiver operating characteristic (ROC) analyses revealing both the inadequacy of existing classification strategies for hyperglycaemia in pregnancy and the inherent challenge of applying dichotomous approaches to what is essentially a continuous spectrum of risk [22]. These results highlight the potential need for metabolic screening and intervention strategies and for risk stratification that better captures the continuous nature of glycaemic risk rather than focusing solely on GDM diagnosis.
Consistent with previous observational studies that demonstrated an increased risk of childhood obesity in offspring exposed to maternal hyperglycaemia [23, 24], our analysis showed that maternal glucose levels in pregnancy, particularly 1 h and 2 h glucose levels, were positively associated with offspring’s BMI at 18 years. While earlier studies reported that GDM exposure was associated with increased adiposity measures [25], our study found that these associations with long-term adiposity were more evident when analysing maternal plasma glucose as a continuous variable than when using GDM status alone.
Previous animal and epidemiological studies have shown the association between maternal diabetes and offspring’s insulin resistance [26, 27]. A Danish cohort found that intrauterine hyperglycaemia exposure was associated with impairments of glucose metabolism, increased adiposity and an adverse cardiometabolic profile in offspring aged 9–16 years [25]. The persistence of these metabolic alterations into early adulthood is particularly noteworthy, suggesting that intrauterine exposure to hyperglycaemia may programme long-term changes in insulin sensitivity. While adjusting for offspring’s BMI attenuated some of these associations, they remained significant, indicating that the influence is partly independent of adiposity. This observation suggests that maternal hyperglycaemia may have a direct impact on offspring’s metabolic pathways, potentially through epigenetic modifications or altered development of pancreatic beta cells and insulin-sensitive tissues [28]. Moreover, the consistent association with 1 h glucose levels suggests that this time point might be particularly crucial for metabolic programming, offering potential insights for targeted intervention strategies [29].
Comparisons with earlier observations from the HAPO-FUS
Our 18-year follow-up study extends and differs from the HAPO-FUS conducted at ages 11–14 years in several aspects [7]. While the HAPO-FUS showed associations across all maternal glucose time points, our study identified particularly strong correlations with 1 h glucose levels, suggesting that this time point might be crucial for long-term metabolic programming. The comparison between these two studies at different developmental stages provides valuable insights: although some associations appear to weaken from early adolescence to young adulthood, their persistence at young adulthood demonstrates the lasting impact of maternal plasma glucose on offspring’s metabolic health. This pattern was more pronounced when maternal glucose was examined as a continuous variable rather than using GDM diagnosis alone, indicating the importance of considering the full spectrum of maternal glucose levels in pregnancy.
Developmental programming of maternal glycaemic influence
Our findings align with and provide further support for the Developmental Origins of Health and Disease (DOHaD) hypothesis, first proposed by David Barker [30] and later expanded by Hanson [31] and others. This concept suggests that the intrauterine environment can substantially influence long-term growth and development outcomes, with both inadequate and excessive nutrition before and during pregnancy contributing to increased risks of obesity, insulin resistance and type 2 diabetes in offspring [32]. The impact of maternal hyperglycaemia on offspring’s metabolic health involves both genetic and environmental factors [33]. Beyond maternal plasma glucose, other maternal factors including obesity and gestational weight gain have been shown to have similar graded effects on offspring’s cardiometabolic outcomes [34]. Our recent genome-wide association study identified several genetic variants associated with gestational diabetes, indicating that genetic predisposition plays an important role in maternal glucose metabolism during pregnancy [35]. The complex interplay between genetic variants and maternal metabolic factors contributes to the developmental programming of offspring’s metabolic health. Understanding these multiple pathways could help identify high-risk mothers and develop targeted intervention strategies.
The persistence of metabolic alterations into early adulthood in our cohort aligns with mechanistic insights from experimental studies. Early rodent experiments revealed the multigenerational impact of maternal hyperglycaemia. In these studies, maternal diabetes and experimentally induced hyperglycaemia were found to result in asymmetrical growth patterns, increased insulin secretion and hyperplasia of insulin-producing beta cells during fetal development, followed by impaired insulin secretion in later life [36]. Mice models of GDM have further shown that even transient glucose intolerance during pregnancy can programme increased adiposity and altered insulin sensitivity in offspring’s adipose tissue [37]. A better understanding of the pathophysiology and heterogeneity of GDM will help to develop targeted interventions with a focus on improved prevention of maternal and offspring’s complications across different life stages, from pre-conception, throughout pregnancy, and beyond [38].
Strengths and limitations
The strengths of our study include that it was conducted as part of the HAPO study, a blinded observational study in which both clinicians and participants were unaware of maternal glucose levels, thus eliminating potential confounding from treatment interventions. The extended follow-up to about 18 years allowed long-term metabolic consequences to be assessed, addressing a crucial gap in understanding the persistence of these associations into early adulthood. Our comprehensive metabolic evaluations, including detailed measures of glucose metabolism and adiposity, provided a thorough assessment of metabolic health. Additionally, our analysis of maternal glucose as a continuous variable provided important clinical implications, suggesting that even a modest increase in the glycaemic level that is below the IADPSG diagnostic criteria for GDM in maternal glucose levels may influence offspring’s metabolic health, regardless of GDM diagnosis.
This study has several limitations. First, approximately two-thirds of participants were lost to follow-up over 18 years, which might introduce selection bias. A comparison of key characteristics between those who completed follow-up and those who were lost to follow-up showed no significant difference for most variables, suggesting minimal bias in the final model; therefore, the generalisability of our findings may not be affected. Notably, mothers with GDM were slightly more likely to be lost to follow-up than mothers with NGT. While we noticed no significant differences in baseline characteristics between mothers with GDM who were followed up vs those who were lost to follow-up, unmeasured factors might still differ between these groups. Second, our sample size may have been insufficient to detect some clinically meaningful differences, especially in the analyses of categorical outcomes. The limited number of cases of GDM reduced statistical power when using GDM as a categorical exposure, which is why we emphasised continuous glucose measures in our primary analyses. Third, as our study included only Asian women from Hong Kong, the findings may not be applicable to other ethnic populations. Fourth, while we adjusted for many potential confounders, we could not account for all factors that might influence offspring’s outcomes, such as genetic background, familial environment, maternal nutrition and offspring’s psychological stress levels. Fifth, we used OR rather than RR in our analyses, which may overestimate the true associations for outcomes with higher prevalence. Finally, the more robust associations seen with continuous glucose measures than with GDM status may be explained by several methodological limitations. A single OGTT may not adequately reflect the dynamic nature of maternal glycaemic management throughout gestation. In addition, the use of IADPSG criteria for GDM diagnosis, which were primarily based on pregnancy outcomes rather than long-term offspring effects, might not be optimal for identifying mothers whose offspring are at risk of metabolic complications in early adulthood. Further research is needed to determine whether better management of maternal glucose levels during pregnancy could improve long-term offspring health outcomes.
In summary, this 18-year follow-up study demonstrated significant associations between maternal plasma glucose in pregnancy, particularly 1 h glucose levels, and offspring’s metabolic health extending into early adulthood. These associations were most apparent when analysed as continuous traits, suggesting that a metabolic relationship exists across the full range of maternal glucose levels, rather than only above the current diagnostic threshold for GDM. Our findings not only support the Pedersen and DOHaD hypotheses, but also highlight the importance of monitoring and managing maternal glucose levels across the glycaemic spectrum beyond traditional thresholds for GDM screening. The persistence of these associations into early adulthood, despite potential attenuation over time, emphasises the need for glycaemic management during pregnancy. Future studies with more frequent glucose measurements throughout pregnancy may better understand the critical windows for metabolic programming, leading to the development of prevention strategies for complications in offspring’s long-term metabolic health.



Comments (0)