Study design and participants
This clinical trial was conducted at the Karolinska University Hospital between 2021 and 2024. Ethical approval was obtained from the Swedish Ethical Review Authority (2019–04747), and the trial was prospectively registered in the Clinical Trial Registry (ClinicalTrials.gov NCT05115682). The study adhered to the ethical principles outlined in the Declaration of Helsinki, and all participants provided written informed consent prior to participation.
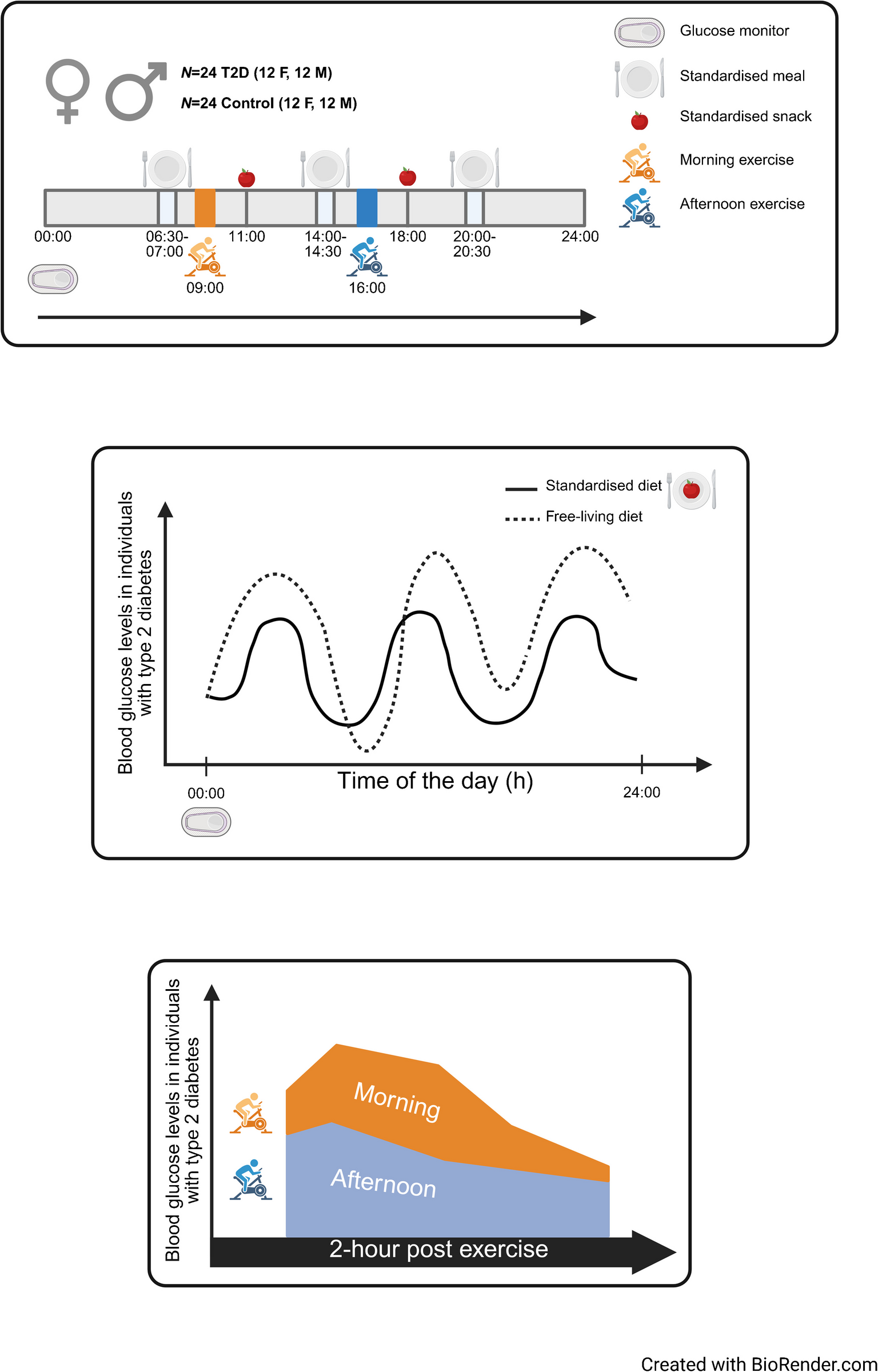
A crossover design was employed, in which participants completed morning and afternoon high-intensity interval exercise sessions on separate days at least 7 days apart. The study comprised two visits consisting of a pre-intervention day (baseline), day 1 (meal intervention), day 2 (meal and exercise intervention), day 3 (meal intervention) and a post-intervention day (baseline). Interstitial glucose levels were continuously monitored using continuous glucose monitors (CGMs) from 72 h before to 72 h after each exercise session. To standardise dietary intake, participants were provided with standardised meals and instructed to adhere to a fixed eating schedule comprising three main meals and one snack for women or two snacks for men per day, with any deviations recorded in a food diary.
Clinical cohorts
Participants were recruited prospectively through advertisements in media such as newspapers, diabetes newsletters and various social media platforms in the larger Stockholm area. Regional and socioeconomic factors were not accounted for in the recruitment process. Initial eligibility screening was conducted via phone, email or using an online screening questionnaire via the REDCap application [19], and included assessments of medical history, age and BMI. To minimise potential genetic and physiological variability, we intentionally recruited a sample of individuals who described themselves as being of European descent; while this approach aims to reduce heterogeneity, it also limits the generalisability of our findings and thus the results may not represent the broader population’s metabolic responses to exercise timing. The study design was unique, and no directly comparable cohorts were available to support a formal a priori power calculation. Thus, an estimation based on anticipated biological effects was performed. Assuming the primary source of variability stemmed from CGM measurements, with an estimated SD of approximately 1.5 mmol/l, we calculated that approximately 15 participants would be required to detect a 1 mmol/l difference in glucose levels with 80% power and a two-sided alpha value of 0.05. As we anticipated greater variability in the glucose responses among individuals with type 2 diabetes, the final sample size was 24 participants per group.
Participants were included if they met the following criteria: men and women (sex was self-reported) aged 45–68 years, with a BMI between 23 and 33 kg/m2. All the women were postmenopausal. For individuals with type 2 diabetes, eligibility required that diagnosis according to the diagnostic criteria established by the Swedish National Board of Health and Welfare [20] was confirmed at least 12 months previously. Control participants were required to have HbA1c levels below 5.7%.
The exclusion criteria were prior or current insulin therapy, not being able to use a cycle ergometer, active smoking or smoking cessation within the past 6 months, cardiovascular conditions, blood-borne diseases, rheumatic illness, malignancies, other systemic disease, use of anti-anxiety medications, or inability to comply with the meal plan. Following screening, a total of 48 participants were enrolled; these participants were evenly distributed among four groups: 12 women with type 2 diabetes, 12 women without type 2 diabetes, 12 men with type 2 diabetes and 12 men without type 2 diabetes (see electronic supplementary material [ESM] Fig. 1).
Nine women and 11 men with type 2 diabetes were being treated with metformin, while six women were prescribed glucagon like peptide-1 agonists. Additionally, three women and two men with type 2 diabetes were being treated with sodium-glucose co-transporter-2 inhibitors. Seven women and six men with type 2 diabetes were receiving cholesterol-lowering statin medication, while only one man in the control group was receiving statin treatment. For BP management, seven women and five men with type 2 diabetes were being treated with BP medication, compared with two women and two men in the control group.
Cardiopulmonary exercise testing
Each participant completed an incremental exercise test to volitional exhaustion on a stationary cycle ergometer (eBike III comfort ergometer, GE Healthcare). The protocol began with a 3 min warm-up of unloaded cycling, after which resistance was increased at a rate of 10–20 W/min, tailored to each participant’s habitual exercise level and capability. Peak workload was recorded as the load achieved at the point of test termination.
During the cardiopulmonary exercise testing, expired air was analysed continuously using an automated breath-by-breath system (Vyntus CPX metabolic cart; Vyaire Medical, Mettawa, IL, USA). Peak oxygen uptake (\(\dot}_}\)) was taken as the highest 20 s oxygen uptake recorded during the test. The anaerobic threshold was identified using the ventilatory equivalent method, defined as the point at which the ventilatory equivalent for oxygen (\(\dot\text\)/\(\dot}_\)) increased without a corresponding rise in the ventilatory equivalent for carbon dioxide (\(\dot\text\)/\(\dot}_\)). The deflection point in the \(\dot}_\) vs \(\dot}_\) relationship was used to confirm the threshold [21]. The heart rate was monitored continuously using a 12-lead ECG (EC Sense ECG; Cardiolex Medical, Stockholm, Sweden). Ratings of perceived exertion (using the Borg 6–20 scale [22]) and the perception of dyspnoea were recorded.
Ultrasound
During the screening phase, a Vivid E95 ultrasound system (GE Healthcare) was used for transthoracic echocardiographic examination of the heart (using a 4Vc-D transducer, frequency 4.0–10.0 MHz) and for scanning of arterial neck vessels (using a 9L-D transducer, frequency 3.0–8.0 MHz, or an 11L-D 9L-D transducer, frequency 3.0–11.0 MHz, as applicable for best image quality). Investigations followed the standards established by the American Society of Echocardiography and the European Association of Cardiovascular Imaging [23]. Tissue images and Doppler flow signals were recorded, ensuring optimal measurement accuracy by aligning the ultrasound beam with blood flow or myocardial motion. Images were stored on a Viewpoint server (Viewpoint 6, version 6.12; GE Healthcare). Trained physicians analysed the images and assessed participant suitability. Individuals with advanced atherosclerotic plaque in the carotid vessels were excluded from further participation.
Clinical chemistry
One week prior to the intervention, participants provided an overnight fasted blood sample at the Karolinska University Hospital for routine clinical chemistry analysis. The panel includes standardised assays performed at Karolinska University Laboratory. The following variables were measured: HbA1c, N-terminal prohormone of brain natriuretic peptide (NT-proBNP), troponin T, insulin, C-peptide, glucose, C-reactive protein (CRP), total cholesterol, LDL-cholesterol, HDL-cholesterol, triglycerides, alanine aminotransferase, aspartate aminotransferase, apolipoprotein A1, apolipoprotein B, creatinine, potassium and haemoglobin. During each experimental trial, venous blood samples were collected before, immediately after and 1 h after the exercise session for analysis of cortisol, CRP, NT-proBNP, insulin and glucagon.
Continuous glucose measurement
Participants were fitted with a Dexcom G6 CGM (Dexcom, San Diego, CA, USA), and glucose data were recorded every 5 min from approximately 72 h before exercise until approximately 72 h post-exercise. The CGM data from all participants were pre-processed individually, annotated and then merged to ensure standardisation of all time points. Data were grouped into morning and afternoon exercise sessions, with days defined as 24 h cycles starting at 06:00 hours on the day prior to the intervention. Glucose readings were categorised into 5 min intervals, and means for each interval were calculated.
To compare effects of morning and afternoon exercise, analyses of CGM data for each participant were performed relative to the time of exercise initiation. Glucose values were normalised to the mean glucose level measured within a 10 min window around the exercise start time (−5 to +5 min) for each individual and condition. This normalisation accounted for baseline glycaemic differences across groups and facilitated direct comparisons of glycaemic responses to exercise.
Glycaemic variability metrics, including AUC and MAGE were calculated using the R statistical software (www.r-project.org) package iglu version 4.1.6 [24].
Standardised meals
Standardised meals were provided during the meeting for CGM fitting. Participants were given a choice of six meal options and four snack options, all designed to meet standardised macronutrient profiles. The meals contained approximately 2259 kJ (540 kcal), comprising 50 g carbohydrates, 25 g protein and 25 g fat. Snacks provided 950 kJ (227 kcal), consisting of 24 g carbohydrates, 16 g protein and 7 g fat. Participants were instructed to adhere to a fixed meal schedule, consuming breakfast between 06:30–07:00 hours, lunch between 13:30–14:00 hours and dinner between 19:30–20:00 hours on the day before exercise, the day of exercise and the day after exercise. Snacks were consumed at 11:00 hours and 18:00 hours. Participants were required to consume identical meals for breakfast and lunch and a different meal for dinner on all meal intervention and meal and exercise intervention days, thus ensuring that the macronutrient composition was consistent between trials.
Exercise session
Participants completed a crossover trial consisting of a single high-intensity interval exercise session conducted in a clinical setting under the supervision of trained exercise physiologists and licensed physicians. The exercise session was performed either in the morning (09:00 hours) or afternoon (16:00 hours), with a minimum wash-out period of 7 days between sessions. Exercise sessions were performed on the same stationary cycle ergometer (eBike III comfort ergometer) as used during the cardiopulmonary exercise testing, with the saddle height adjusted to match the prior setting. The high-intensity interval exercise protocol began with a 7 min warm-up, starting at 50 W for men and 30 W for women, with a cadence of 75 rev/min. Resistance was increased incrementally each minute until 70% of the peak workload recorded during the cardiopulmonary exercise testing was reached, followed by a 1 min recovery period at the starting resistance (50 or 30 W). Participants then performed six intervals of 1 min at 100% of peak workload, followed by 1 min of recovery at 50 W (men) or 30 W (women), at a cadence of 75 rev/min. The exercise protocol concluded with a 3 min cool-down period at the starting resistance (50 or 30 W) and the same cadence. While the resistance was different between the sexes during the warm-up and recovery periods, the mean rating of perceived exertion was similar between men and women (16±1 and 15±1 arbitrary units, respectively), regardless of metabolic status or time of day. BP was measured before, during and after the exercise session. Heart rate was continuously monitored using a 12-lead ECG (EC Sense ECG). Participants were fitted with a peripheral i.v. cannula inserted into a superficial vein for repeated blood sampling. Blood samples were collected before exercise, immediately post-exercise and at 1 h post-exercise.
Statistical analysis
Statistical analyses were conducted using R software (version 4.4.1, www.r-project.org). A two-way ANOVA was used to examine the main effects of type 2 diabetes, sex and the interaction of these parameters on the outcomes of interest. The primary outcome was the effect of time of day on glucose management in relation to high-intensity interval exercise following standardised meals. The secondary outcome was to determine the effect of standardised meals on glucose management. Additionally, we determined the effect of exercise at different times of the day on metabolic markers, including stress and inflammatory markers. The normality of data distribution was assessed using the Shapiro–Wilk test, while homogeneity of variance was evaluated using Levene’s test. If assumptions of normality or variance were violated, a Tukey ladder of powers transformation was applied before conducting the ANOVA. Post hoc pairwise comparisons were performed using Tukey’s honestly significant difference (HSD) test. Statistical significance was set at p<0.05.
For analysis of glycaemic variability MAGE was calculated during 24 h periods and AUC was calculated 2 h following the start of the exercise. MAGE, AUC and plasma markers of stress and metabolism, were analysed with a linear mixed-effects model. Models were fitted using the lmer function from the R lme4 package (version 1.1-35) to assess the effects of exercise time of day, sex and diabetes status, while accounting for repeated measurements within individuals as a random effect. ANOVA was used to evaluate the significance of these effects. Post hoc pairwise comparisons were performed using estimated marginal means (R emmeans package version 1.10.4), with significance defined as p<0.05.
To assess potential carryover effects, a sequence factor (morning → afternoon vs afternoon → morning) as a fixed effect in the linear mixed-effects model was used to evaluate differences in glucose AUC following exercise at different times of day. This analysis was limited to women with type 2 diabetes, as this group showed the strongest intervention effect. The sequence term was not statistically significant (p=0.553), indicating no detectable carryover effects. The p values for the main effects remained unchanged after including the sequence term, continuing to demonstrate a significant increase in glucose levels following morning exercise, but not afternoon exercise.



Comments (0)