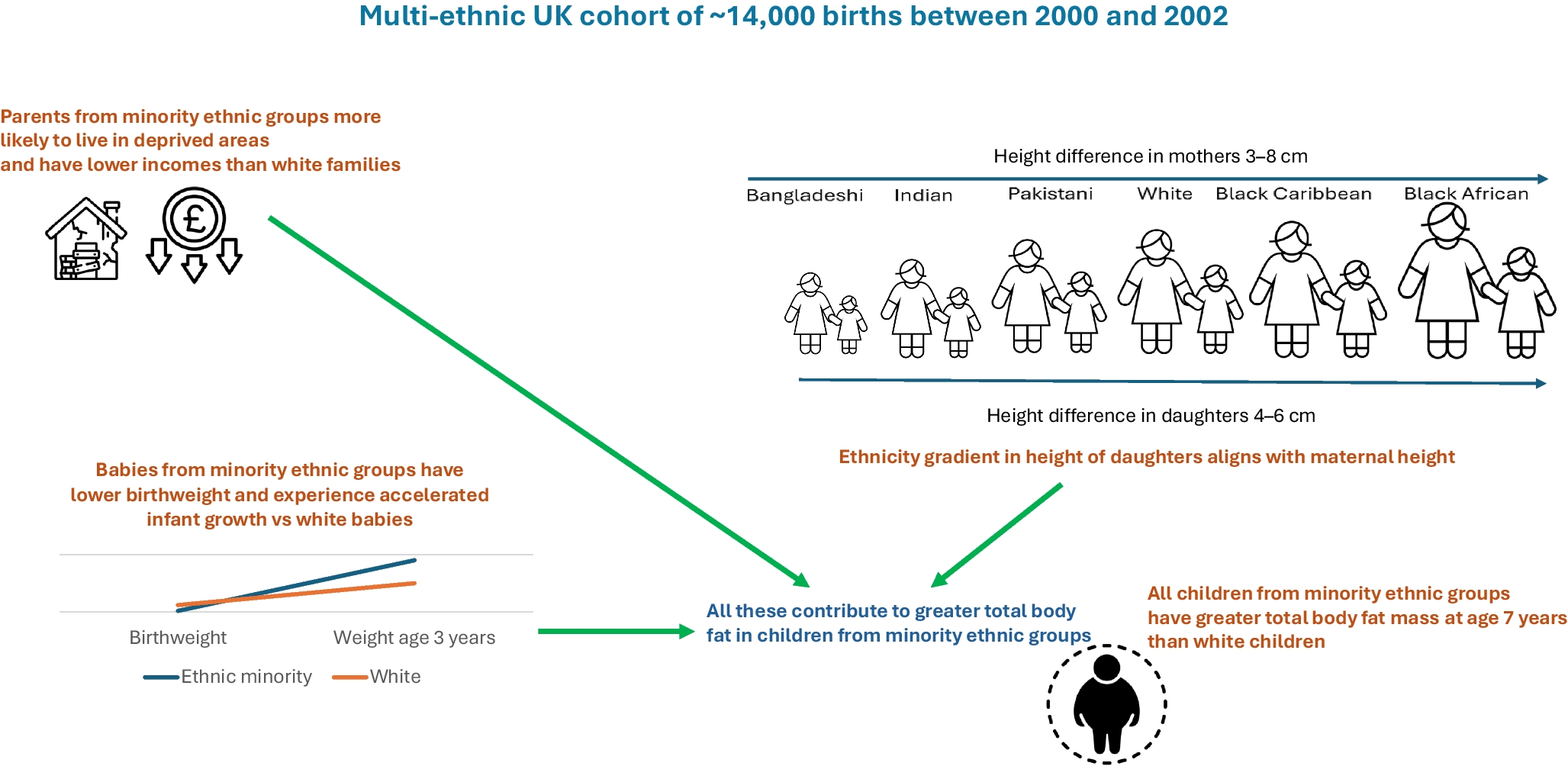
Young adults of South Asian, Black African and Black Caribbean ethnicity born in the UK at the turn of this century have distinct early life growth patterns compared with the White population. They share low birthweight and early accelerated growth, accompanied by premature growth deceleration. The magnitude of the former and timing of the latter, however, differs by ethnicity, impacting final body habitus. At age 17 years, South Asian people were lighter and shorter, while Black African and Black Caribbean people were heavier and of similar or marginally lower height compared with their White counterparts. Minority ethnic groups had greater total FM than White people but South Asian children had lower, and Black Caribbean children and Black African girls higher, indices of FFM than White children. However, the ratio of FM to FFM was uniformly greater in all minority groups at age 7 years than in White children. Low birthweight followed by greater postnatal growth in all minority groups studied here contributes to excess FMI compared with White children, with further contributions from adverse individual and neighbourhood socioeconomic position in people of Black African and Black Caribbean ethnicity. All analyses were stratified by sex, but largely, ethnic differences in anthropometry and associations with determinants were similar in both sexes.
Low birthweight in children of South Asian, Black Caribbean and Black African ethnicity in the UK is known [16], and previous analyses of this cohort concluded that this was largely due to adverse socioeconomic circumstances [10]. While accelerated postnatal growth is also recognised [17], the current analysis is the first to identify important differences in the effects this has on achieved height and weight beyond the age 5 years for different ethnicities. Relative weight gain from birth in all ethnic minority groups is of similar magnitude, and greater than that observed in White children. However, as children of Black African and Black Caribbean ethnicity have higher birthweights than South Asian children, this accelerated weight gain results in heavier children by age 3 years compared with White children, an advantage that persists through to late adolescence. Absolute weight gain in South Asian children is lower, and weight only briefly achieves levels similar to or greater than those in White boys around age 11 years, otherwise remaining lower than in White boys and girls throughout early life.
In contrast to weight, all minority ethnic groups are taller by the age of 3 years. This height advantage is also progressively and differentially lost. By age 17 years, Black African children are of similar height to, and Black Caribbean children somewhat shorter than, White children. The height advantage at age 3 years in South Asian groups is progressively lost, first in those of Bangladeshi, then of Pakistani and finally of Indian origin. By the age of 14 years all South Asian ethnicities are shorter than White children. This ethnic difference is particularly marked for Bangladeshi children, who by age 17 years are ~5.0–6.0 cm shorter than their White counterparts.
Interestingly the ethnic subgroup gradient in achieved height and weight by age 17 years in the current generation is identical to that observed in their parents. Persistence of low birthweight has been observed some generations after migration from Surinam to the Netherlands [18], and in African-Americans in the USA [19] resident in the USA for many generations. Short maternal stature and lower lean mass correlate with smaller organ mass and smaller birth canal dimensions [20, 21], which may then constrain fetal growth through both genetic and plastic mechanisms [22]. More broadly, poor in utero development as a consequence of constrained early growth of the mother, and continuing adverse maternal circumstances, may determine persistence of adverse growth patterns in migrant populations [20,21,22]. It should be noted that height is strongly influenced by environmental factors (e.g. in just a few decades, South Koreans have become on average 8 cm taller than their North Korean counterparts).
Continued low socioeconomic position in minority groups is, however, a unifying feature in high-income countries and others have shown that low socioeconomic position is a key determinant of these low birthweights [10]. Most previous studies focus on the period of early weight gain [23] but we show that while relative weight gain is similar across minority groups (and uniformly greater than in the White group) the absolute consequences for height and weight, allied to differential ‘wearing off’ of this rapid growth, is markedly different. Accelerated postnatal growth was observed in all minority groups, even though certain standard risk factors, such as maternal smoking, breastfeeding and maternal educational status, were often more favourable.
All minority groups displayed earlier growth deceleration compared with White children, and all minority girls were markedly more likely to experience early puberty, defined here as menstruation onset before age 11 years, than White girls. This confirms previous analyses on this cohort but notably the percentage of Black Caribbean girls, at ~18%, is far higher than previously reported (13.0%) [13], as we excluded those of mixed ethnicity from our analysis. This earlier onset of menarche will make an additional contribution to adult obesity and type 2 diabetes [24].
We confirm FMI at age 7 years is greater in all minority groups [25], and remains so through to age 17 years apart from in Indian girls. We also confirm that FFMI is lower in South Asian children but higher in children of Black Caribbean, and girls of Black African, ethnicity [6]. However, in resolution of this paradox in FFM, we also show that the ratio of FM to FFM is uniformly greater in all minority ethnic groups studied here compared with White children at age 7 years. Skeletal muscle, proxied here by FFM, is an important determinant of type 2 diabetes risk [26]. Mechanisms include impaired insulin-stimulated glucose uptake, fatty deposition, imbalanced protein synthesis and poor mitochondrial function. While bioelectrical impendence analysis captures quantity, and we show that relative quantity is lower in minority groups than in the White group, this tells us little about relative quality. Given the more adverse early life patterns of growth in minority groups, we suggest that lean mass quality may also be poorer [27] and contribute to the observed greater risk and earlier onset of type 2 diabetes.
Biological, specifically genetic explanations have been invoked to account for ethnic differences in body composition [28]. However, self-reported ethnicity is not a biological construct [29] and the importance of current lifestyle and of socioeconomic position should not be overlooked. Generational increases in height [8], by some 6 cm over 50 years in the UK, have been ascribed to better diets and to a reduction in catastrophic childhood infection. Socioeconomic status, as a determinant of access to adequate and healthy nutrition, may account for the reversal in the socioeconomic gradient in obesity [8] and for the more adverse fat patterning observed in latter generations.
Ethnic differences in FMI were most strongly associated with relative weight gain between birth and age 3 years. Birthweight and maternal pre-pregnancy weight also made independent contributions to ethnic differences in FMI. It should be noted that South Asian mothers were both lighter and shorter than their White counterparts, accounting for the multivariable estimated ethnic difference in FMI in South Asian vs White children being of greater magnitude than the unadjusted estimate, as generally lower maternal height and weight should each associate with lower rather than higher FMI in the offspring. While we distinguish maternal/early life and socioeconomic determinants of ethnic differences in FM, it should be noted that the former, such as maternal height, smoking status and offspring birthweight, are also dependent on socioeconomic factors. Thus it is likely that we have underestimated the role of socioeconomic position in accounting for ethnic differences. Additionally, similar to previous analyses of socioeconomic differentials [9], we show that individual and neighbourhood socioeconomic position each contribute to ethnic differences in FM, indicating that beyond familial circumstances, the more obesogenic environments of neighbourhood deprivation (greater density of fast-food outlets, fewer opportunities for recreation), play a role in adverse fat accumulation. Yet adverse neighbourhood socioeconomic factors, which should similarly affect people of both South Asian and of African ethnicity, cannot explain the markedly lower levels of FFM in South Asian groups. Pomeroy and colleagues demonstrated a marked reduction in stature in people from the Indian subcontinent allied to adoption of an agricultural lifestyle some 11,000 years ago, and of a low lean mass for given body size [30]. They hypothesised that these expressions of body habitus are due to historical climatic adaptation and to cumulative ecological pressures.
The MCS is representative of the UK population at birth, and efforts were made to ensure appropriate representation of minority ethnic groups. Sample attrition and attendant data missingness have been overcome by multiple imputation. We largely report absolute (standardised) differences in body habitus at each age, rather than model growth trajectories. This is a critical initial first step to identify important differences and critical time points before embarking on methods to model growth trajectory heterogeneity; such models often make a priori assumptions, require careful specification and ideally multiple approaches to compare consistency of outcomes and thus enable robustness of conclusions [31]. BIA estimates FM% and can be used to derive FM and FFM, and the respective indices. These equations make assumptions about relationships between body habitus and FM, and about the relationship of body proportions with FFM. Previous BIA validation studies against gold standard deuterium methods in UK multi-ethnic childhood and adolescent populations variously report both over- and underestimation of FM and FFM by bioimpedance in minority ethnic groups [6, 32]. Bioimpedance equations that overcome these biases have been proposed. Unfortunately, the MCS did not record direct bioimpedance measures, so that more ethnically valid derived equations could not be applied. However, as the direction of ethnic difference in FMI and FFMI remains consistent in validation studies, even though the magnitude may differ [6], we do not view this as a major limitation.
In conclusion, we demonstrate marked ethnic subgroup differences in early development that relate to achieved height and weight, body fat, FFM and reproductive maturity in the UK. Minority ethnic groups in the UK display more adverse patterns in body habitus than White children, likely determining early onset of type 2 diabetes and other chronic conditions, though further follow-up of the MCS is needed to be certain of this. The role of ethnic differences in quality, as opposed to quantity, of fat and of lean mass in accounting for the differential risk of type 2 diabetes is not known, nor is the impact of disordered early growth on tissue quality understood. Part of these ethnic differences can be accounted for by adverse individual and neighbourhood socioeconomic position, which persists across generations [33]. Addressing socioeconomic adversity is imperative if we are to resolve the intergenerational cycle of adverse growth and premature onset of chronic disease.



Comments (0)