
Remember me
This study was approved by the institutional review board with a waiver of consent granted. This was a retrospective review of radiographic images of distal femurs and proximal tibias in children up to 1 year of age who underwent a skeletal survey for suspected child abuse.
Using our institution’s radiology information system (RIS), a pediatric radiologist with 28 years of experience post-fellowship, who did not participate in the imaging evaluation, retrospectively retrieved all skeletal surveys performed for evaluation of child abuse from 2007 to 2023. Two groups of patients were identified. The first group included children with a diagnosis of child abuse and reports of distal femur or proximal tibia CMLs. The second group included children without a diagnosis of child abuse and a reported distal femur or proximal tibial metaphyseal variation, with either no fractures or isolated accidental skull fracture, as isolated skull fracture has been found to be associated with a low risk for child abuse [12].
For the CML group, the RIS was searched using the keywords of “CML,” “classic metaphyseal lesion,” “corner fracture,” or “bucket handle fracture.” For the metaphyseal variation group, the keywords were “irregularity,” “step off,” “beak,” “spur,” “fragmentation,” and “variation.”
Radiograph selection and preparationInitial and follow-up radiographs (if available) were included. From the skeletal surveys, the anteroposterior and lateral Digital Imaging and Communications in Medicine (DICOM) radiographs of the femurs and tibias were selected and anonymized. To minimize potential bias from other injuries visible on the radiographs, all images were trimmed by an experienced radiologic technologist under the supervision of a pediatric radiologist who was not involved in the image evaluation. Trimming was performed using the Santa DICOM Editor (Santsoft, Athens) to isolate the metaphysis of the distal femur or proximal tibia, or both —depending on which structures were included in the original radiograph.
Medical record reviewTwo child abuse pediatricians, who were not involved in image interpretation, reviewed the electronic medical record (EMR) and documented the following: demographic information, history of prematurity, underlying medical conditions, the original radiologist’s interpretation of distal femur and proximal tibia findings, other injuries noted in the skeletal survey, additional imaging obtained to evaluate for abusive injuries, and the presence of physical injuries such as bruising, burn injuries, other skin injuries, retinal bleeding, subconjunctival hemorrhage, and torn frenula.
The reports of neuroimaging studies were reviewed for the presence of subdural hematoma, parenchymal contusion or tear, parenchymal bleeding, and hypoxic-ischemic changes. If there was no history or medical conditions to adequately explain them, the presence of at least one of these findings was considered a sign of high likelihood of abusive head trauma.
The child abuse pediatrician’s report was reviewed and categorized as positive, negative, or indeterminate for the diagnosis of physical abuse. Children with an indeterminate diagnosis of child abuse were excluded.
Exclusion criteriaPatients with metabolic bone disease or skeletal dysplasia were excluded. Additionally, cases were excluded if the radiology report indicated a CML, but the child was not diagnosed with child abuse, or if the report described a metaphyseal variation in a child with either an intermediate or positive diagnosis of child abuse. Radiographs were also excluded if imaging of the distal femurs and proximal tibias was limited to a single view, obscured by casting material or intraosseous lines, or demonstrated bony or soft tissue post-traumatic abnormalities that could not be adequately trimmed. Finally, patients for whom a consensus diagnosis of either CML or metaphyseal variation could not be reached were excluded from the study.
A reference standard for diagnosis of CML and metaphyseal variationA consensus diagnosis, serving as the ground truth, was established by two pediatric radiologists with 19 years and 28 years of post-fellowship experience respectively, who were unblinded to clinical and imaging follow-up. Based on this consensus, cases were categorized into two groups: those with CML and those with metaphyseal variations.
Radiograph reviewDICOM images were reviewed independently by eight radiologists using a diagnostic high-resolution monitor on the Synapse PACS system (FUJIFILM Medical Systems, Lexington, MA). All evaluations were performed in a randomized order and blinded to clinical information. To prevent paired comparison, initial and follow-up radiographs were separated and randomized, ensuring that radiologists could not view corresponding studies concurrently. Four reviewers were pediatric radiologists with 2 years, 5 years, 13 years, and 19 years of experience. Four were adult emergency radiologists with 5 years, 16 years, 16 years, and 23 years of experience. Data collection and management were conducted using a secure, web-based application (REDCap; Vanderbilt University, Nashville, TN).
For each metaphysis, the radiologist selected one of the following options: normal, variation, CML, or indeterminate. If normal, variation, or CML was selected, the radiologist assigned a level of low, moderate, or high confidence.
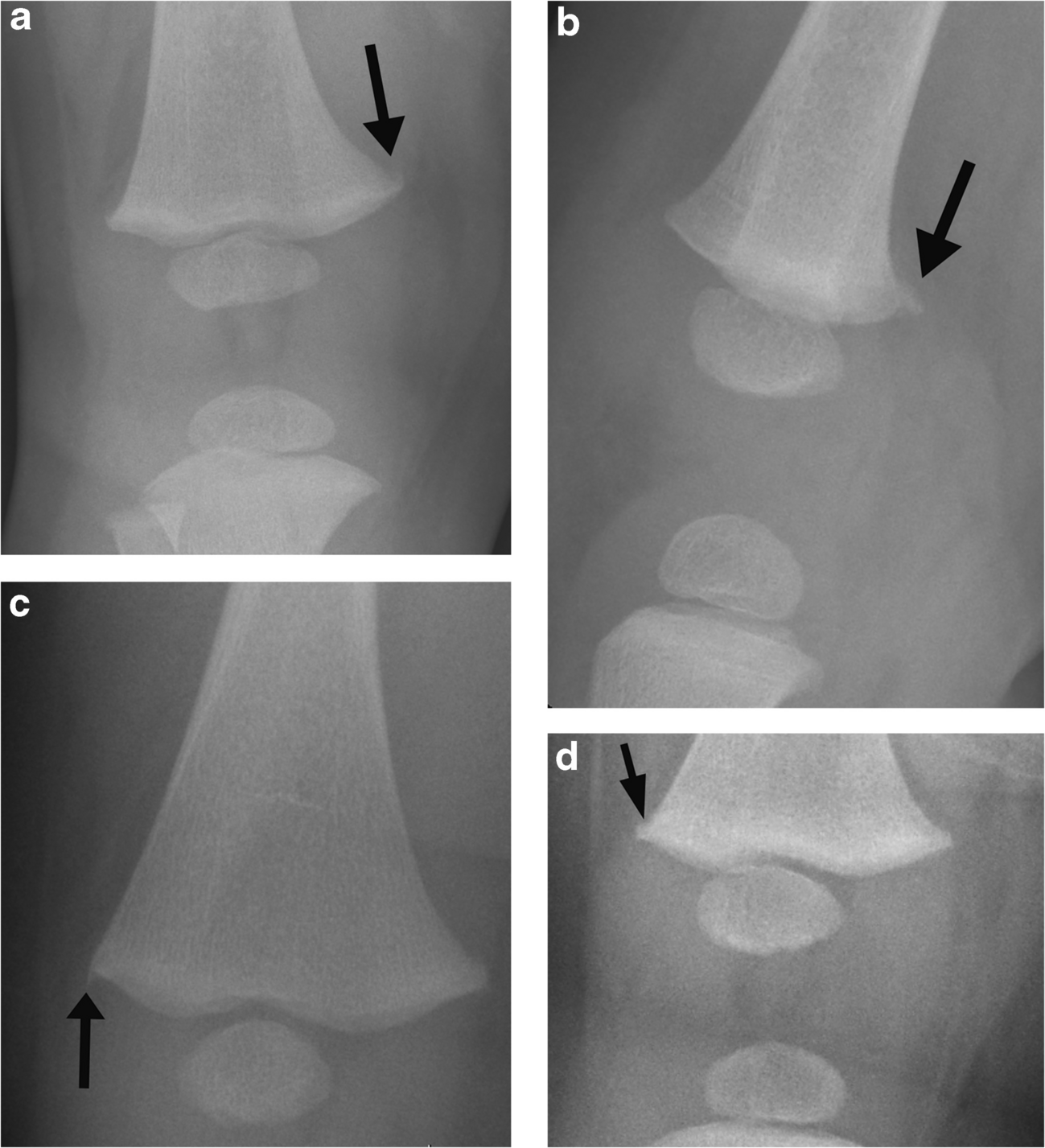
For diagnosing CML, radiologists identified corner or bucket-handle fractures (any healing stage), corner deformity, subphyseal lucency, or metaphyseal irregularity with a rough metaphyseal–physeal margin. Metaphyseal variation (Fig. 1) is diagnosed by the presence of step-off (acute discrete distal metaphyseal angulation), spur (longitudinal thin cortical projection beyond the metaphyseal edge), or fragmentation (metaphyseal corner fragmentation oriented along the shaft), with the specific location (medial, lateral, anterior, or posterior) noted. The location is described as affecting either the entire metaphysis or at least one of the following locations: medial, lateral, anterior, or posterior metaphysis.
Fig. 1
Metaphyseal variations a. Metaphyseal fragmentation variation in a 3 month-old girl. Anteroposterior (AP) radiograph of the right knee demonstrates bony fragmentation extending proximally from the distal medial femoral metaphyseal corner (arrow). b. Lateral radiograph of the right knee in the same patient shows corresponding posterior metaphyseal fragmentation (arrow). c. Metaphyseal spur variation in a 4 month-old boy. AP radiograph of the right knee demonstrates a discrete longitudinal projection of bone (arrow) that is continuous with the cortex and extends beyond the metaphyseal margin. d. Metaphyseal step off variation in a 7 month-old boy. AP radiograph of the right knee demonstrates an acute cortical angulation at the junction of the distal lateral metaphysis and the physis (arrow)
In cases where both a metaphyseal variant and a CML were present, only the CML is included in the analysis.
Before formally reviewing images, a pilot training session was conducted using 11 cases not meeting the study’s inclusion criteria and excluded from the final cohort. These cases included six metaphyseal variations, four CMLs, and one indeterminate metaphyseal irregularity. The annotated cases were presented to the readers to familiarize them with the spectrum of appearances and reinforce the classification criteria.
Statistical analysisFisher’s exact tests and two-sample t-tests were used to compare the CML and metaphyseal variation groups for differences in patient characteristics. Agreement between radiologists in diagnoses with moderate and high confidence was evaluated using crosstabs, percentage agreement, and kappa statistics. Kappa values of 0.10–0.20 were considered as slight, 0.21–0.40 as fair, 0.41–0.60 as moderate, 0.61–0.80 as substantial, and 0.81–0.99 as near perfect agreement [13]. A bootstrap analysis with 10,000 iterations was used to test the difference in kappa statistics between pediatric and adult radiologists.
For sensitivity and specificity calculations, we evaluated diagnoses with moderate and high confidence. A true positive diagnosis was defined as follows: a diagnosis of CML was considered correct for children in the CML group, and a diagnosis of metaphyseal variation was considered correct for children in the metaphyseal variation group. Generalized estimating equation models (GEEs) for binary outcomes were used to obtain combined estimates across all radiologists for accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). The GEEs accounted for correlations among readings from multiple radiologists for each patient. GEEs were then used to compare pediatric and adult emergency radiologists for differences in the percentages of correct moderate or high confidence interpretations.
Using all confidence diagnoses levels, GEEs were also used to compare patients with metaphyseal variation and CML for differences in the frequencies of radiographic signs typically associated with metaphyseal variation (metaphyseal step off, beak, spur, fragmentation) and radiographic signs typically associated with CML (corner fracture, bucket-handle fracture, subphyseal lucency, metaphyseal irregularity).
GEEs were used to compare confidence levels (low confidence and indeterminate diagnoses versus moderate and high confidence diagnoses) between pediatric and adult emergency radiologists.
Comments (0)