
Remember me
This retrospective study was conducted at a quaternary academic pediatric center. Institutional review board (IRB) approval was obtained, along with a waiver of documentation of written informed consent. All study activities adhered to the guidelines of the Health Insurance Portability and Accountability Act (HIPAA).
Department and hospital electronic medical records were reviewed to identify all (pediatric) patients under the age of 18 years who underwent a clinically indicated 18F-FDG PET/CT between January 2014 and May 2024. To ensure an even age distribution and account for the known age dependence of brown fat uptake, a maximum of 50 scans per year of age was included. Examinations were excluded if performed at an outside hospital, if a non-FDG imaging agent was used, or if the primary diagnosis was pheochromocytoma. Pheochromocytoma is known to increase FDG-uptake in brown fat [9, 10].
Demographic and clinical data for each patient, including variables that may influence 18F-FDG metabolism (e.g., age, sex, BMI, concurrent medications, underlying diagnoses, glucose levels), were recorded along with details of patient preparation (e.g., fentanyl dose or reason for not administering). Concurrent medications administered within 24 h of the PET/CT exam were reviewed to identify children who received medications which may have suppressed brown fat uptake (e.g., opioids, benzodiazepines, or beta blockers). Additionally, the outside temperature on the day of each scan was documented.
All patients imaged with 18F-FDG PET/CT at our hospital undergo the following preparatory steps. First, patients are put in a warm room and/or in a warming chair. Then, warm blankets are placed around their entire body including wrapping around the legs and shoulders. All patients are warmed starting approximately 30–60 min prior to 18F-FDG-injection. A nursing workup is performed to determine if patients are appropriate for fentanyl administration. If deemed appropriate, fentanyl is administered 10 min prior to FDG injection at a dose of 1 mcg/kg up to 50 mcg/kg. For patients weighing more than 50 kg, fentanyl is administered on a sliding scale of 5 mcg per additional 10 kg of body weight beyond 50 kg, with a maximum dose of 70 mcg. Patients are monitored by nursing staff for at least 15 min after fentanyl administration.
Our institutional guidelines for fentanyl administration are as follows. Fentanyl is administered to individuals over 1 year of age with a diagnosis of lymphoma or those with head, neck, or upper extremity disease. In all other cases, fentanyl is administered in female individuals 1–25 years of age and male individuals 1–20 years of age. Administration is withheld under specific exclusion criteria. These include prior allergic reaction to fentanyl, driving self to appointment, body weight less than 10 kg, or patients less than 1 year of age. Fentanyl is also contraindicated in patients who have recently received narcotic medications, display current or potential respiratory compromise, or patient/family preference against fentanyl.
Clinically obtained 18F-FDG PET/CT scans were reviewed by six board-certified pediatric radiologists, one of whom has additional board certification in nuclear radiology, with each scan reviewed by three radiologists. Reviewers assessed each scan for the presence, location, and intensity of brown fat uptake. Brown fat intensity was graded using a 5-point scale analogous to the Deauville scale (Fig. 1) [11]. The anatomical location of brown fat uptake was categorized into five predefined regions: neck, supraclavicular, paraspinal, mediastinal, and retroperitoneal/perinephric. Final determination of the presence of brown fat uptake for the purpose of study analysis was defined based on the agreement of at least two radiologists. Final anatomical distribution of brown fat uptake was based on the agreement of at least two radiologists. Final brown fat uptake intensity was defined by agreement of at least two radiologists or the mean of the scores of three radiologists if all disagreed.
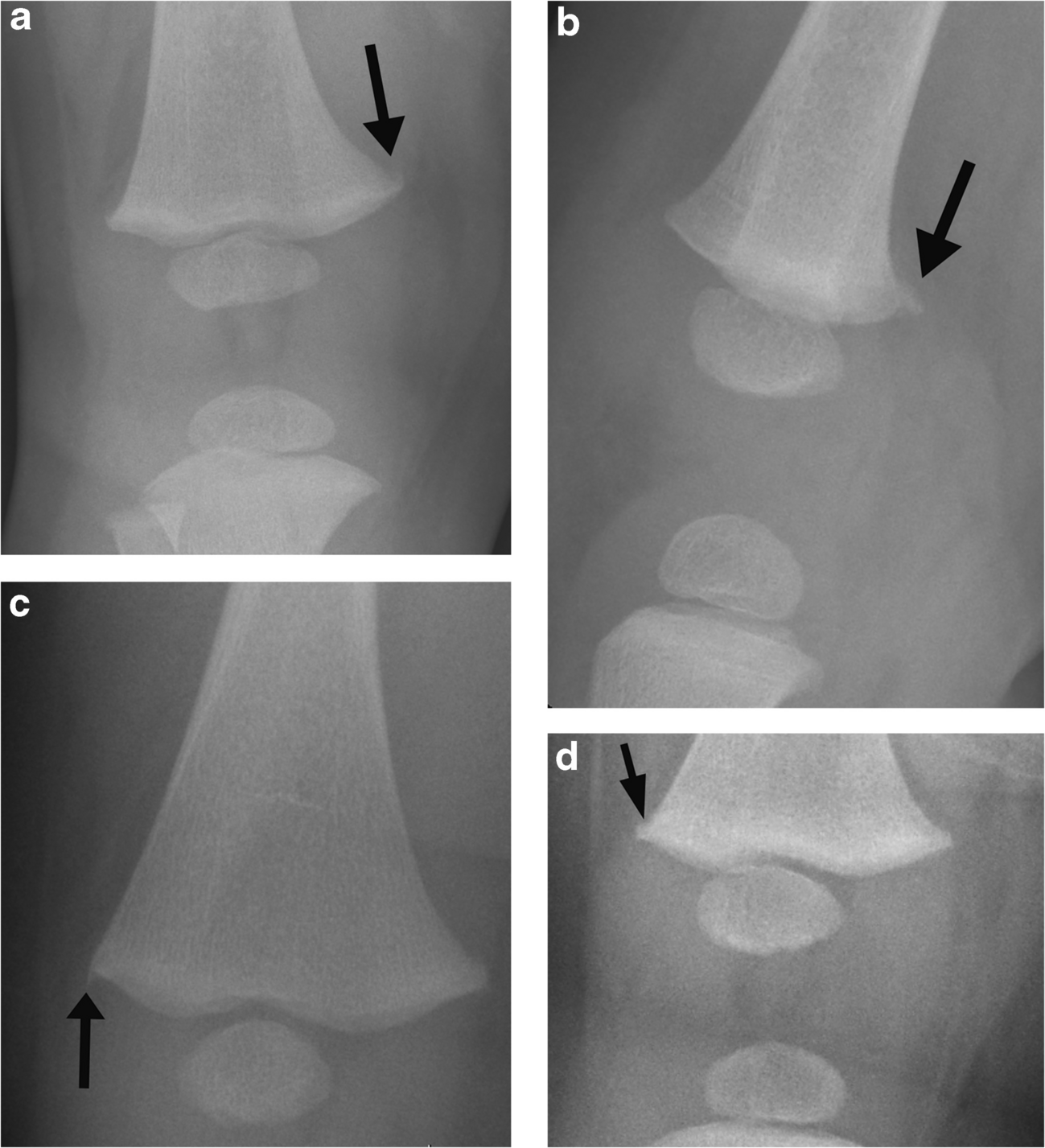
Fig. 1
Examples of the Deauville-analog scoring system used to grade brown fat uptake intensity (arrows). All images are maximum uptake projection images from 18F-FDG-PET exams. a Score 2, uptake less than mediastinal blood pool; a 15-year-old female with thrombotic thrombocytopenic purpura; b score 3, uptake greater than mediastinal blood pool and less than liver; a 16-year-old male with suspected lymphoma; c score 4, uptake moderately more than liver; a 15-year-old male with suspected lymphoma; d score 5, uptake markedly more than liver; a 16-year-old male with Hodgkin lymphoma
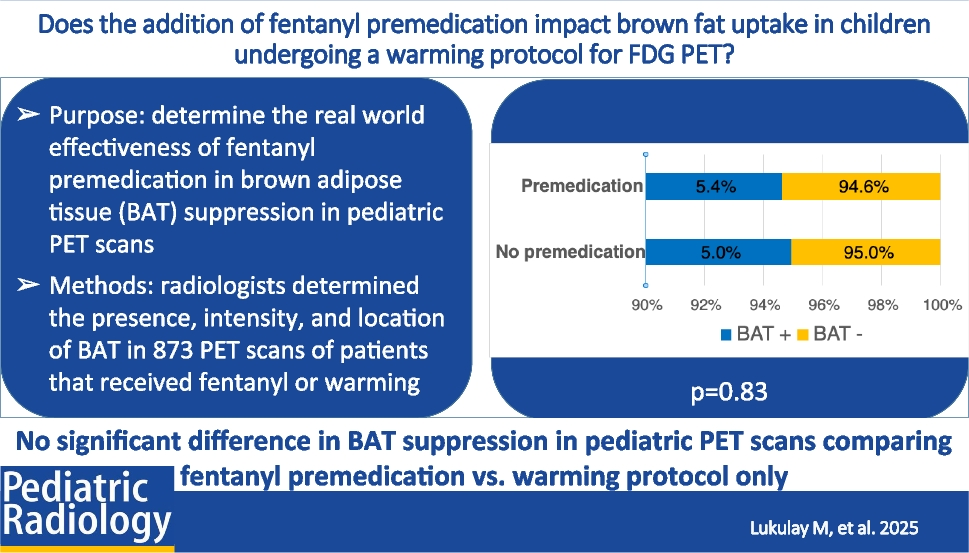
Statistical analysisParticipant demographics were summarized using descriptive statistics. Median and inter-quartile range (IQR) were used for continuous variables, whereas counts and percentages were used for categorical variables. Premedication and non-premedication groups were compared using the chi-square test (categorical variables) and the two-sample t-test (continuous variables). A statistically significant difference was defined as P < 0.05 for all inference testing. All statistical analyses were performed using MedCalc Statistical Software version 22.009 (MedCalc Software Ltd.) or R (R version 4.3.1, http://www.r-project.org).
Comments (0)