
Remember me
Ileocolic intussusception is the most common cause of bowel obstruction in young children. There is an ongoing debate about whether it is a middle-of-the-night emergency and if delays in intervention have a significant impact on outcome.
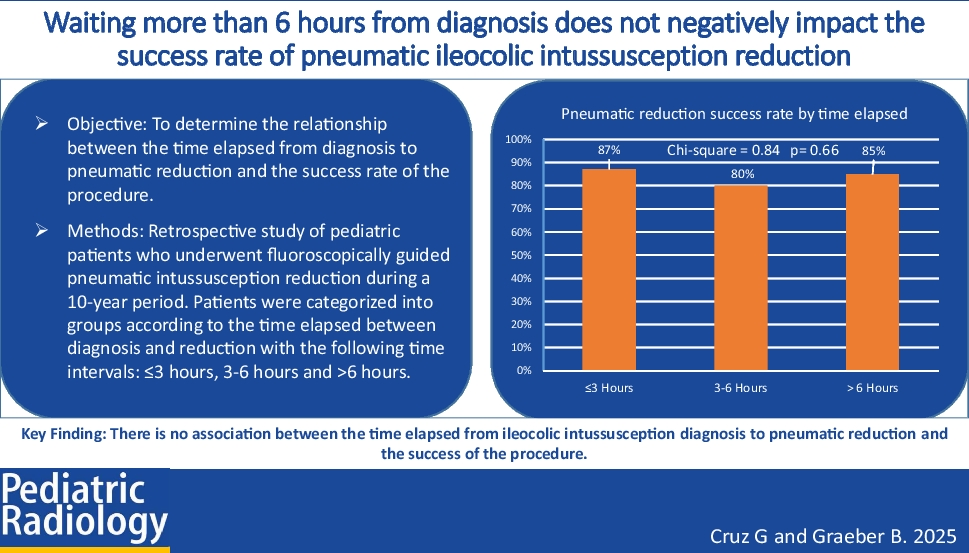
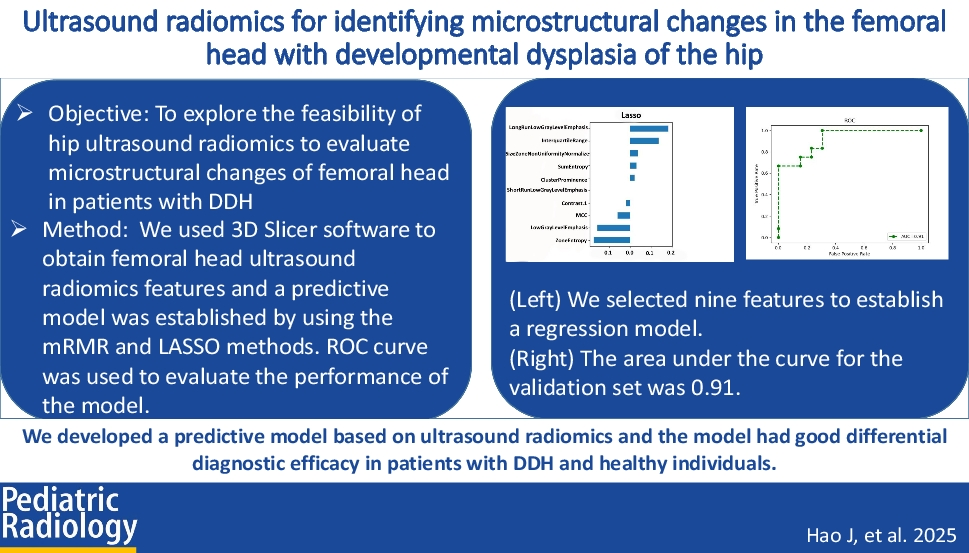
ObjectiveTo determine the relationship between the time elapsed from diagnosis to pneumatic reduction and the success rate of the procedure.
Materials and methodsA retrospective study was performed on pediatric patients who underwent fluoroscopically guided pneumatic intussusception reduction during a 10-year period. Patients were categorized into groups according to the time elapsed between diagnosis and reduction with the following time intervals: ≤ 3 h, 3–6 h, and > 6 h. A chi-square test analyzed the association between the time elapsed from diagnosis to attempted reduction and the success rate.
ResultsThe study population consisted of 78 males and 38 females. Median age was 22.5 months (2–129 months). Median time elapsed between diagnosis and attempted reduction was 149 min (25–1389 min; IQR, 261 min). The overall success rate of pneumatic reduction was 85% (108/127, 95% CI 79–91%). The recurrence rate was 9.4% (95% CI 4.2–15%). Within the three intervals studied (0–3 h, 3–6 h, and more than 6 h), the success rates were 87% (61/70, 95% CI 77–93%), 80% (24/30, 95% CI 63–90%), and 85% (23/27, 95% CI 68–94%), respectively. The chi-square test yielded a statistic of 0.84 with a P-value of 0.66, indicating no significant correlation between the time elapsed from diagnosis to reduction and the success of the procedure.
ConclusionThere is no association between the time elapsed from ileocolic intussusception diagnosis to pneumatic reduction and the success of the procedure.
Graphical Abstract
Comments (0)