
Remember me

The first clinical recommendations for CVRM in women originated from 1999 [17] and were updated in 2020 [18]. Since then, female-specific and traditional risk factors with a greater impact on women than men have been identified. Key modifiable factors include hypertension, smoking, cholesterol, obesity, and diabetes. While these affect both sexes, the magnitude of the associations is not the same [19]. Large-scale meta-analyses have shown that diabetes confers a 44% greater excess risk of CHD in women [20]. Mechanisms are unclear but may involve biological or care-related factors. Women also achieve better blood pressure control, possibly due to differences in drug type and dosage [21], and show sex-specific vascular responses to smoking [22], potentially explaining their increased risk.
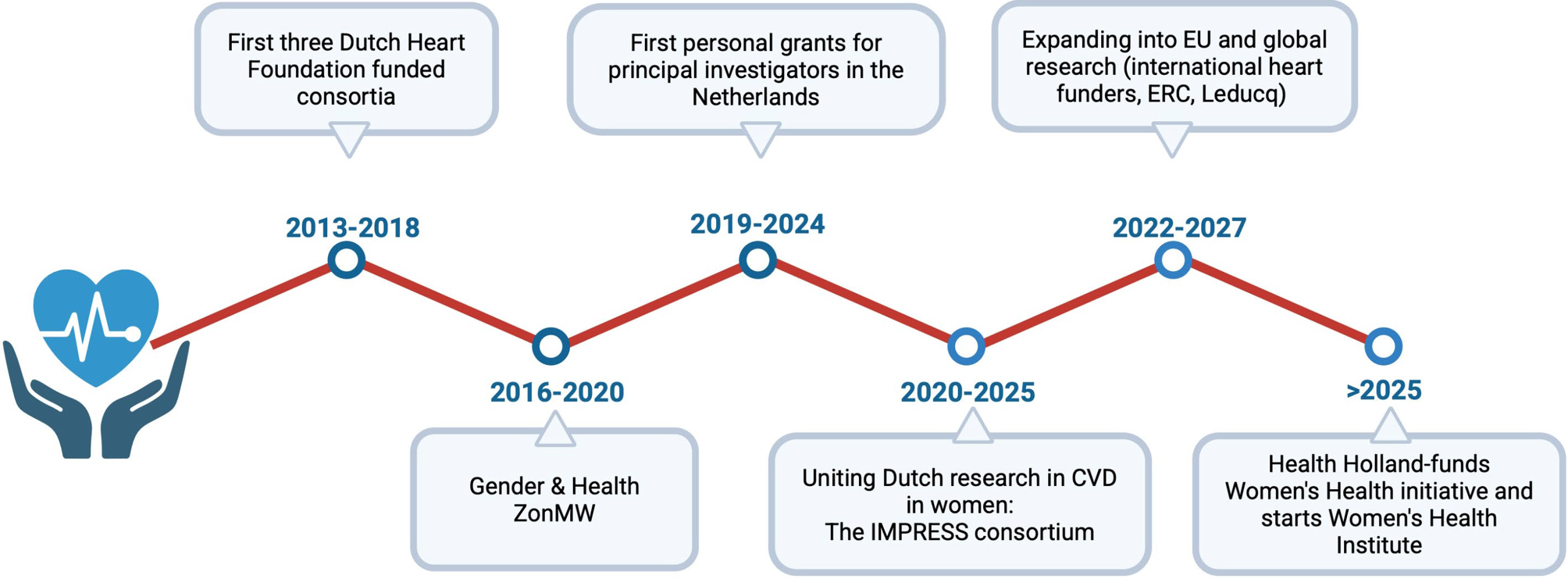
Female-specific factors related to pregnancy, reproduction, and hormonal changes, such as adverse pregnancy outcomes, polycystic ovary syndrome, and menopause timing, have been linked to long-term CVD risk [23, 24]. In 2013, the Dutch Heart Foundation launched new consortia co-led by experts in gynaecology. A key early study showed a linear increase in cardiovascular mortality with earlier age at menopause [25], but many underlying mechanisms remain unclear. Our studies have advanced knowledge on the long-term cardiovascular consequences of hypertensive pregnancy disorders [14, 26, 27], yielding prediction models to guide screening and follow-up after complicated pregnancies [28].
While observational studies have advanced the field, they are inherently limited by residual confounding or reverse causation. Moreover, many are underpowered to detect sex-specific effects. To address this, we performed several Mendelian randomisation studies and found no sex differences in the genetically proxied relationship between diabetes, age at menopause, and CHD [16, 19, 29, 30]. However, body mass index had a stronger causal effect on diabetes risk in women [31]. Similarly, age at menarche and pre-eclampsia were also causally linked to increased CVD risk [32, 33]. Complementing these findings, coronary CT angiography showed atherosclerosis in 30% of women aged 45–55 with prior preeclampsia, versus 18% of controls [13]. Platelet RNA profiles in these women showed enrichment for CAD susceptibility genes [34], contributing evidence to the link between preeclampsia and CAD. While CAD and HF have distinct mechanisms, preeclampsia also correlates with higher HF risk [14, 35], highlighting the need for broad preventive measures for both CAD and HF in this population.
Clinical presentation of CAD in womenWomen differ from men not only in cardiovascular risk profiles but also in symptom presentation. Although chest pain is common to both sexes, women with ACS often report less typical symptoms such as atypical chest discomfort, fatigue, or dyspnoea [36]. In the Netherlands, general practitioners (GPs) are the first point of contact for patients with chest pain. Each year, approximately 700,000 individuals present with such complaints, making up 44% of all chest pain cases in primary care. Yet only 15% are referred to cardiology [37], and ultimately, just 6.6% are diagnosed with CVD [38]. This pathway creates a diagnostic gap, particularly for women with ischemic symptoms but normal or near-normal angiographic findings, many of whom have ANOCA and are misclassified as having non-cardiac chest pain.
To address this issue, the IMPRESS consortium has co-developed an accredited e‑learning program for GPs. This program trains providers to recognize key features of ANOCA—such as prolonged rest-related chest pain accompanied by fatigue—and to distinguish these from other causes like reflux or musculoskeletal complaints. This program, accessible online, aims to reduce misdiagnosis and improve outcomes [39].
Obstructive CADAtherosclerotic plaques in women and men differ in composition and behaviour. In the setting of ACS, women often present with plaque erosion rather than plaque rupture compared to men [40], and tend to have fibrous plaques whereas men more frequently present with unstable and inflammatory lesions (Fig. 2; [41]). Also, plaque haemorrhage is associated with plaque vulnerability and adverse outcomes in men, but not in women, suggesting sex-specific differences in the prognostic value of plaque features [42]. As one of the breakthroughs in understanding sex differences in atherosclerosis, the identification of cellular and molecular drivers of atherosclerotic plaques in women in two independent vascular tissue biobanks explains why plaques can differ between sexes [43, 44]. In women, plaque gene expression was enriched for vascular cell plasticity processes like endothelial-to-mesenchymal transition. In men, immune-related pathways predominated. Notably, even in postmenopausal women (~ 2 years), several gene expression patterns were still linked to oestrogen signalling, suggesting long-lasting effects of sex hormones. Sex differences were also evident in vascular gene expression studies using endothelial cells from opposite-sex twins and adults, showing that 14–25% of the endothelial cell gene expression is sex-biased, identifying both innate (likely sex chromosome-based) and acquired (likely sex hormone-based) sex differences. Genes with acquired sex-related differences in adults were indeed more likely to be influenced by sex steroids [45].
Fig. 2
Spectrum of obstructive and non-obstructive coronary artery disease. Schematic representation of the continuum of coronary artery disease (CAD) encompassing both obstructive and non-obstructive phenotypes. The diagram distinguishes obstructive CAD from non-obstructive forms, which include endotypes such as coronary microvascular dysfunction and vasospasm, grouped under the term ANOCA, as well as other entities (Takotsubo cardiomyopathy and spontaneous coronary artery dissection)
Together, these findings indicate that sex differences in vascular biology are present from birth and evolve throughout life, likely contributing to the distinct pathways of CAD in women and men.
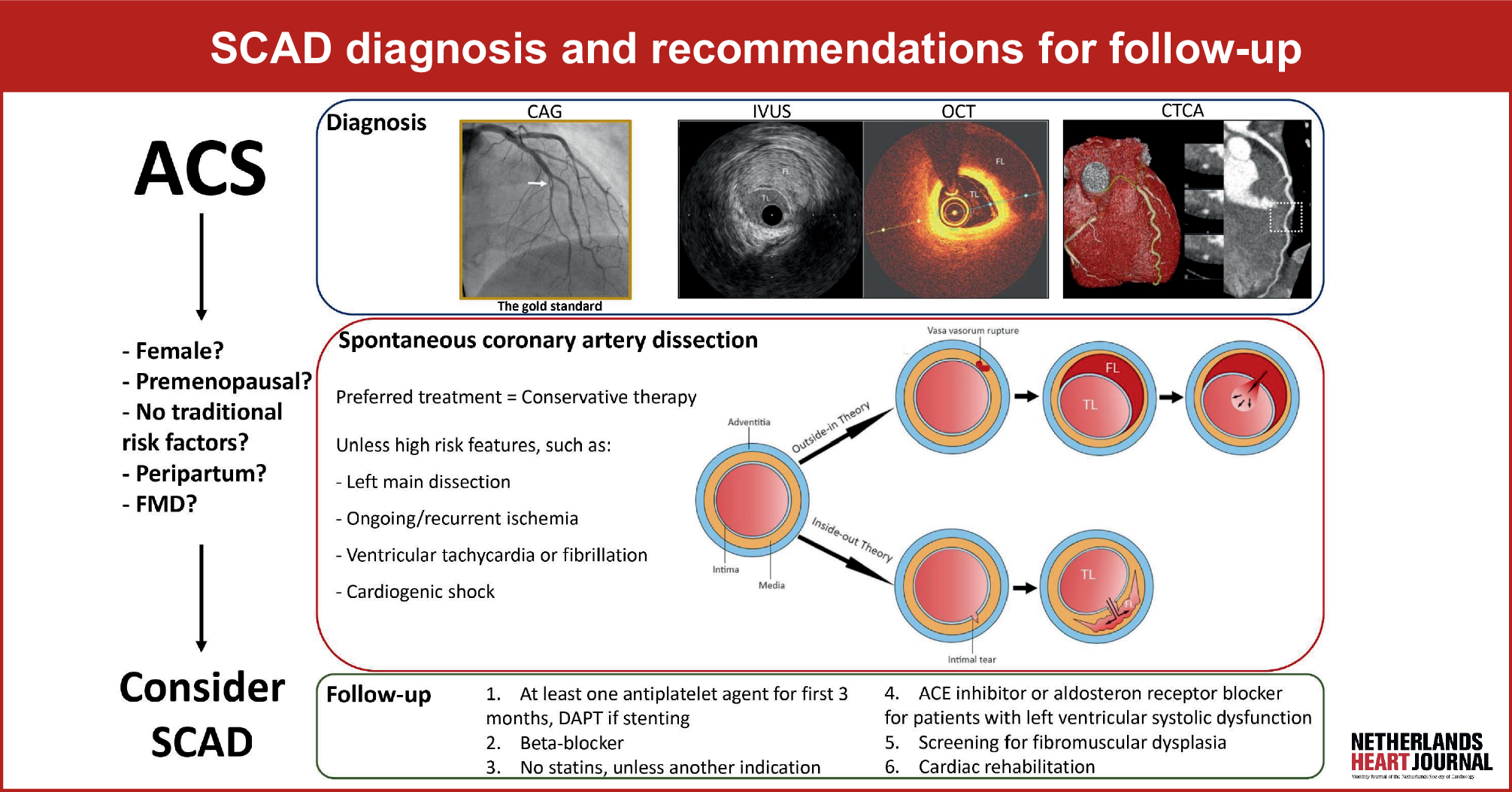
Non-obstructive CADNon-obstructive CAD, defined as < 50% luminal stenosis, is more frequently diagnosed in women than in men [46]. In the IMPRESS—Julius GP data-linkage (n = 2,546), 39% of women versus 23% of men had non-obstructive CAD. During follow-up, these patients reported persistent symptoms, high healthcare use, as well as an increased HF risk [15]. The term angina with non-obstructive coronary arteries (ANOCA) is a broad, symptom-based umbrella that describes angina in the absence of significant epicardial obstruction. The clinical spectrum of ANOCA includes two groups: ischemia with non-obstructed coronary arteries (INOCA)—characterized by objective evidence of myocardial ischemia such as abnormal stress test, coronary function test (CFT), or perfusion MRI without myocardial injury—and myocardial infarction with non-obstructive coronary arteries (MINOCA) involving acute myocardial injury confirmed by biomarkers or imaging evidence of necrosis. Additionally, spontaneous coronary artery dissection (SCAD) and Takotsubo cardiomyopathy (TTC) represent further non-obstructive entities commonly linked to mechanisms such as coronary microvascular dysfunction (CMD), vasospasm, and myocardial stunning (Fig. 2). These conditions predominantly affect younger or perimenopausal women and present atypically, complicating timely diagnosis and optimal management [47]. Despite the absence of obstructive lesions, all these entities impose significant symptom burdens and adverse outcomes.
To address this unmet clinical need, the Netherlands Society of Cardiology (NVVC) published dedicated guidelines on ANOCA in 2020 [48], advocating a structured diagnostic approach with CFT to differentiate vasospastic from microvascular angina endotypes. However, these recommendations are not yet incorporated into the Dutch General Practitioner guidelines (NHG 2019), which continue to advise against cardiology referrals for atypical chest pain frequently observed in ANOCA.
To facilitate clinical implementation and research, the IMPRESS consortium has supported the establishment of the Netherlands Registry of Invasive Coronary Vasomotor Function Testing (NL-CFT), currently involving data from 20 of the 69 hospitals in the Netherlands [49]. This registry provides a strong infrastructure for ongoing ANOCA research, particularly trials. Initial medical therapy typically precedes invasive testing; however, recent ESC 2024 guidelines strongly recommend CFT (Class I, Level B) for patients experiencing persistent angina despite medical treatment [50]. The diagnostic utility of CFT is high, demonstrating vasomotor dysfunction in approximately 78% of tested patients while maintaining a low complication rate (< 1%) (see Electronic Supplementary Material (ESM) in reference S1). Nonetheless, limited availability and associated costs represent significant barriers, motivating further exploration of alternative diagnostic tools such as ECG-based predictors, Holter monitoring, and peripheral vascular assessments (S1–S3). CFT allows clinicians to differentiate CMD from vasospastic angina, the two main ANOCA endotypes (Fig. 2). Differentiating these endotypes has been shown to improve prognosis and quality of life in ANOCA patients (S4). Furthermore, by recognizing the complexity and diagnostic uncertainty faced by patients, their experience can be improved. Therefore, we developed a patient decision aid that is publicly available online to support shared clinical decision-making for the diagnostic trajectory (S5).
Comments (0)