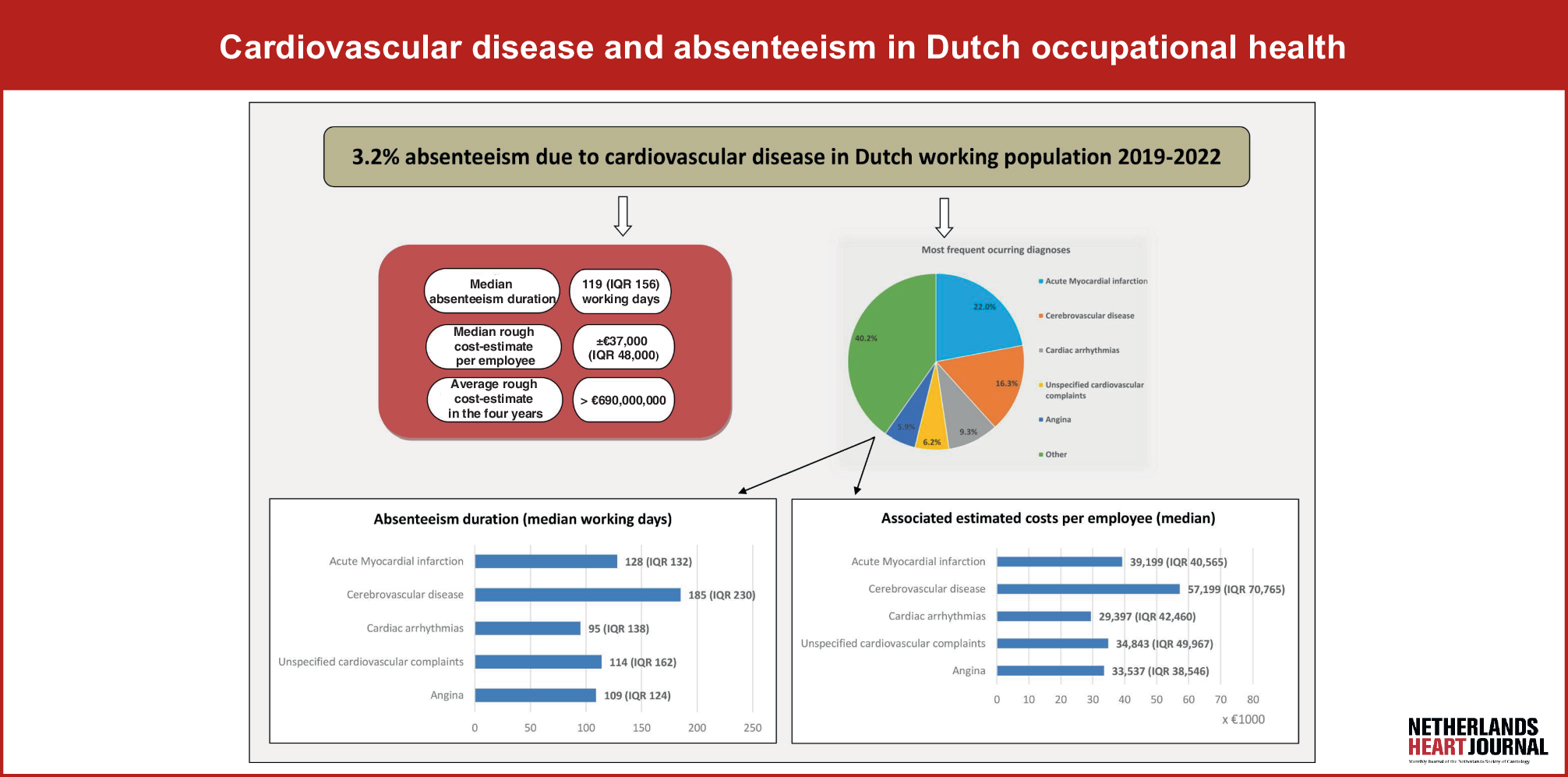
In this exploratory study, we used standard-of-care data from two major occupational health services in the Netherlands to examine absenteeism due to cardiovascular disease (CVD) within a large cohort of the Dutch working population from 2019 to 2022. We observed a 3.2% incidence of absenteeism due to CVD, a median absenteeism duration of 119 working days, and a minimum rough cost-estimate for employers of around € 37,000 per employee. Of all CVD diagnoses, cerebrovascular disease was found to be associated with the longest absenteeism duration. For reference, in the Netherlands two frequently occurring causes of absenteeism or work disability are stress-related illness (average absenteeism duration 101 working days; average cost to the employer of € 19,151 per employee [11]) and low back pain (median absenteeism duration 95 days; mean cost to the employer of € 15,350 per employee [17]).
In our study acute myocardial infarction (AMI) and cerebrovascular disease were the two most frequently occurring diagnoses, with an average absenteeism duration of 128 days and 185 days, respectively. These absenteeism durations are quite similar to earlier findings, thus even though medical care has evolved over time, AMI and cerebrovascular disease are still associated with a relatively long absenteeism duration. This highlights the critical importance of focusing rehabilitation efforts on achieving return-to-work (RTW) after AMI and cerebrovascular disease. Effective rehabilitation can help employees resume work, enhance their quality of life, and reduce absenteeism costs.
RTW rates within 12 months after acute coronary syndrome (ACS) range from 67–93%, with an average delay of 2–3 months. Kruse et al. reported 79% RTW after coronary heart disease (CHD) admissions versus 93% after other diagnoses [2]. In our study, approximately 86% of employees returned to work within 6–12 months following AMI. RTW outcomes after CVD are influenced by medical (e.g., ventricular function, ischemia, rhythm stability), occupational (e.g., physical demands, shift work, commuting), and psychosocial factors (e.g., depression, self-perceived health, cognitive impairments) [18, 19]. A multinational review identified six barriers (job strain, anxiety, depression, comorbidity, older age, low education) and four facilitators (job control, work ability, good perceived health, high socioeconomic status) to RTW after CVD [19]. Non-fatal CHD is associated with increased absenteeism, presenteeism, delayed RTW, early labour force exit, and unemployment, challenges that likely extend to AMI survivors, who also face risks such as reduced job responsibilities, part-time work, lower income, and dismissal [5, 19].
Cardiac rehabilitation (CR) uptake in the Netherlands is suboptimal. A nationwide cohort study analysing 106,212 patients with CVD between 2013 and 2019 reported an initial increase in CR participation from 28% in 2013 to 41% in 2016, after which rates stabilized [20]. Previously, RTW rates following CR have shown to be 65% at six months and 67% at twelve months following CR, with predictors including younger age, non-manual work, self-employment, higher quality of life, and favourable exercise ECG outcomes [21]. Although one Danish study indicated a lower probability of RTW at three months following CR, it demonstrated a higher probability at nine and twelve months [22]. In the Netherlands, CR programs are multidisciplinary, comprising exercise training, cardiovascular risk management, psychological support, and occupational counselling, aligned with national and European guidelines. Regarding neurorehabilitation, 86% of patients with acquired brain injury returned to work immediately after a four-month vocational rehabilitation program, with 64% remaining employed at long-term follow-up [23]. Dutch neurorehabilitation similarly integrates physical, cognitive, psychological, and vocational interventions to enhance functional recovery and work reintegration. Interestingly, Yokota et al. demonstrated in a small study population that cardiac rehabilitation following standardized in-hospital rehabilitation improved exercise tolerance and functional strength in patients recovering from cerebrovascular stroke [24].
Implications for clinical practice
Occupational health professionals play a key role in ensuring sustainable reintegration for employees recovering from significant health conditions such as CVD. Their responsibilities include helping employees regain optimal functioning, ideally returning to pre-CVD performance levels, or finding new roles when full recovery is not feasible. Effective reintegration requires enhanced collaboration among medical disciplines such as cardiologists, neurologists, rehabilitation physicians, and occupational health experts. An integrated approach focusing on rehabilitation participation and work-related factors can improve employees’ quality of life, reduce employer costs, and provide broader societal benefits, including higher tax revenues and reduced social security expenses [19]. Person-centred care and digital rehabilitation programs have been shown to improve return-to-work rates after ACS and assist professionals in maintaining progress while resuming work activities [19].
Conclusions
This study demonstrates that cardiovascular disease (CVD) is a primary cause of absenteeism in at least 3.2% of cases within the Dutch labour force. CVD is associated with relatively prolonged absenteeism and incurs substantial costs for employers. Additionally, acute myocardial infarction, cerebrovascular disease, cardiac arrhythmias, unspecified cardiovascular disease, and angina are the most frequently occurring diagnoses among this working population.
We advocate for a greater focus on work-related aspects in both in-hospital and outpatient treatments for CVD. To achieve this, it is essential that in-hospital and outpatient medical specialists collaborate more effectively with occupational health professionals. Furthermore, there is a pressing need for the development of more work-focused guidelines to better integrate occupational health considerations into cardiovascular care.


Comments (0)