
Remember me

Us2.AI is a CE-marked, vendor-neutral software platform for automated analysis of TTE’s (Fig. 1). It integrates with standard ultrasound systems or with picture archiving and communication systems (PACS) and can be deployed either on-premises or in the cloud, depending on institutional requirements for data governance and infrastructure. The system performs automated view classification, image quality assessment, segmentation, and quantification of 68 guideline-recommended parameters, including left and right ventricular volumes and function, atrial size, Doppler indices (e.g., E/e’), and global longitudinal strain [1,2,3]. A full analysis and structured draft report are typically generated within two minutes after DICOM upload, without any manual input. Measurements are already generated during the echo examination, giving the sonographers live feedback on the generated analyses. All outputs, including numeric values, contours, and textual interpretations, are presented in an editable, ASE/EACVI-aligned format. Users can review, adjust, or reject results, with all changes automatically propagated throughout the report. This ensures full clinical control, traceability, and transparency in every step of the workflow. Integration with hospital systems is supported via HL7 or PDF, among other options. An automated audit trail is incorporated, allowing careful post-analysis follow-up for any necessary future evaluations of system performance.
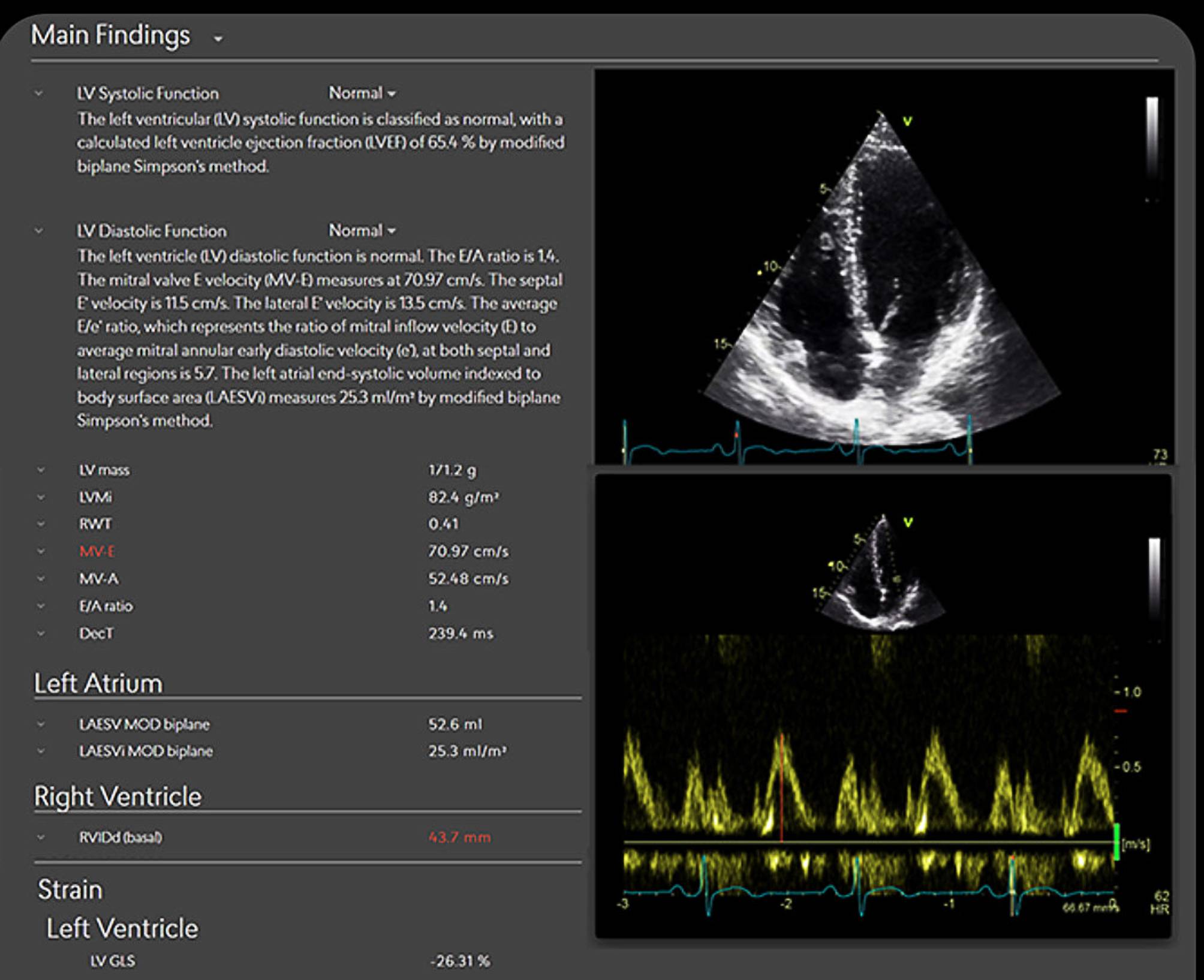
Fig. 1
AI-generated echocardiography report using Us2.AI. Example of an automated report displaying measurements for systolic and diastolic function, left atrial volume, right ventricular size, and strain, with editable contours and Doppler tracings. All outputs are presented in a guideline-aligned format, allowing clinician review and adjustment
In a multicenter validation study of 602 echocardiographic exams, the algorithm achieved an individual equivalence coefficient (IEC) < 0 for all parameters, with 95% confidence bounds < 0.25, indicating that AI-human variability was lower than expert inter-reader variability [1]. ICCs ranged from 0.74 for left ventricular ejection fraction to 0.97 for interventricular septum thickness. These findings support its reproducibility and readiness for clinical use.
Comments (0)