This review and meta-analysis demonstrated substantial variation in anticoagulation prescription in critically ill patients with trigger-induced AF and low adherence to CHA2DS2-VASc. The meta-analysis demonstrated no association between anticoagulation prescription and thromboembolism (or stroke) reduction in patients with trigger-induced AF. Notably, the use of anticoagulation was associated with improved short-term survival but an increased incidence of long-term stroke, while the incidence of bleeding was not influenced.
The decision to initiate anticoagulation is preceded by a careful weighing of the benefits (prevention of thromboembolism) and risks (increased bleeding risk). Ideally, the decision is informed by the baseline risks and the relative effect of anticoagulation on these outcomes. However, in trigger-induced AF, the CHA2DS2-VASc score has been shown to perform poorly in predicting stroke risk [9]. Additionally, the available data from the included studies did not allow us to assess any association between the CHA2DS2-VASc score and stroke risk.
We found that the association between anticoagulation and the risk of in-hospital thromboembolic events was small in both relative and absolute terms. We identified no statistically significant association between anticoagulation and in-hospital thromboembolism. The outer limit of the 95% confidence interval (an OR of 0.61) would constitute an absolute risk difference of merely 0.8% in favour of anticoagulation at an average baseline thromboembolic risk of approximately 2% during hospitalisation [26]. This should be weighed against the risk of bleeding. Although we also found no association between anticoagulation and in-hospital bleeding, the uncertainty in terms of absolute risks is higher because clinically significant bleeding is much more common than thromboembolism. The outer limit of the confidence interval (OR 1.22) would constitute an absolute risk increase of 2.8% at an average baseline bleeding risk of approximately 12.6%. It is possible that some deaths may have resulted from fatal strokes or bleeding, which might have been missed due to the observational nature of these studies.
These findings persist despite the implementation of methods such as propensity score matching and sensitivity analyses to address potential biases in several studies. Likely, the observed associations do not represent the unbiased causal effects of anticoagulation [9, 26, 29]. Yet even in the face of potential biases, the results indicate, on the whole, that the conventional risk-benefit analysis is not applicable in trigger-induced AF during acute hospitalisation. The high absolute risk of bleeding and the high relative risk of stroke under anticoagulation (i.e., the apparent lack of protective effect) are profoundly different from patients with ambulant AF. Appropriate and validated stratification of stroke and bleeding risk for this population is an important knowledge gap.
The retrospective nature of the included studies introduces several types of bias, most notably confounding by indication. Patients at a perceived increased risk of thromboembolism or stroke or with a high AF burden are more likely to be prescribed anticoagulation therapy. This is one of the likely explanations for the association between anticoagulation use and long-term thrombotic complications. Also, the adequacy of anticoagulation therapy remains uncertain due to the lack of data regarding patient adherence, the presence of treatment interruptions, maintenance of therapeutic INR levels, or the appropriateness of DOAC dosing.
Immortal time bias is potentially introduced as clinicians may choose to delay anticoagulation therapy and thereby increasing mortality in non-treated patients as a result of early deaths [32,33,34]. Also, if a patient survives, sinus rhythm restoration may impact the decision regarding long-term anticoagulation This form of AF, which appears in the context of critical illness, is potentially transient [19, 35], and overall AF burden is reported to be relatively low [36,37,38], with about two-thirds of patients experience AF for less than 24 h [1, 19, 35].
Long-term recurrence data indicate that about one-third to half of patients experience AF within one year of hospitalisation [36,37,38]. Its prevalence may be underestimated, and intensive monitoring increases the likelihood of detecting recurrent AF [39]. The decision to initiate, continue, or terminate anticoagulation should be guided by the actual recurrence of AF and its associated AF burden, not merely by the occurrence of a single AF event. Andreotti and De Caterina have proposed such an approach for post-CABG AF [40, 41]. Here, advances in the clinical quality of care can be made even without randomized trials. Extensive monitoring can provide better insight into which patients have recurrent AF, and this should be easier with recent technological advances.
Limitations and future perspectives
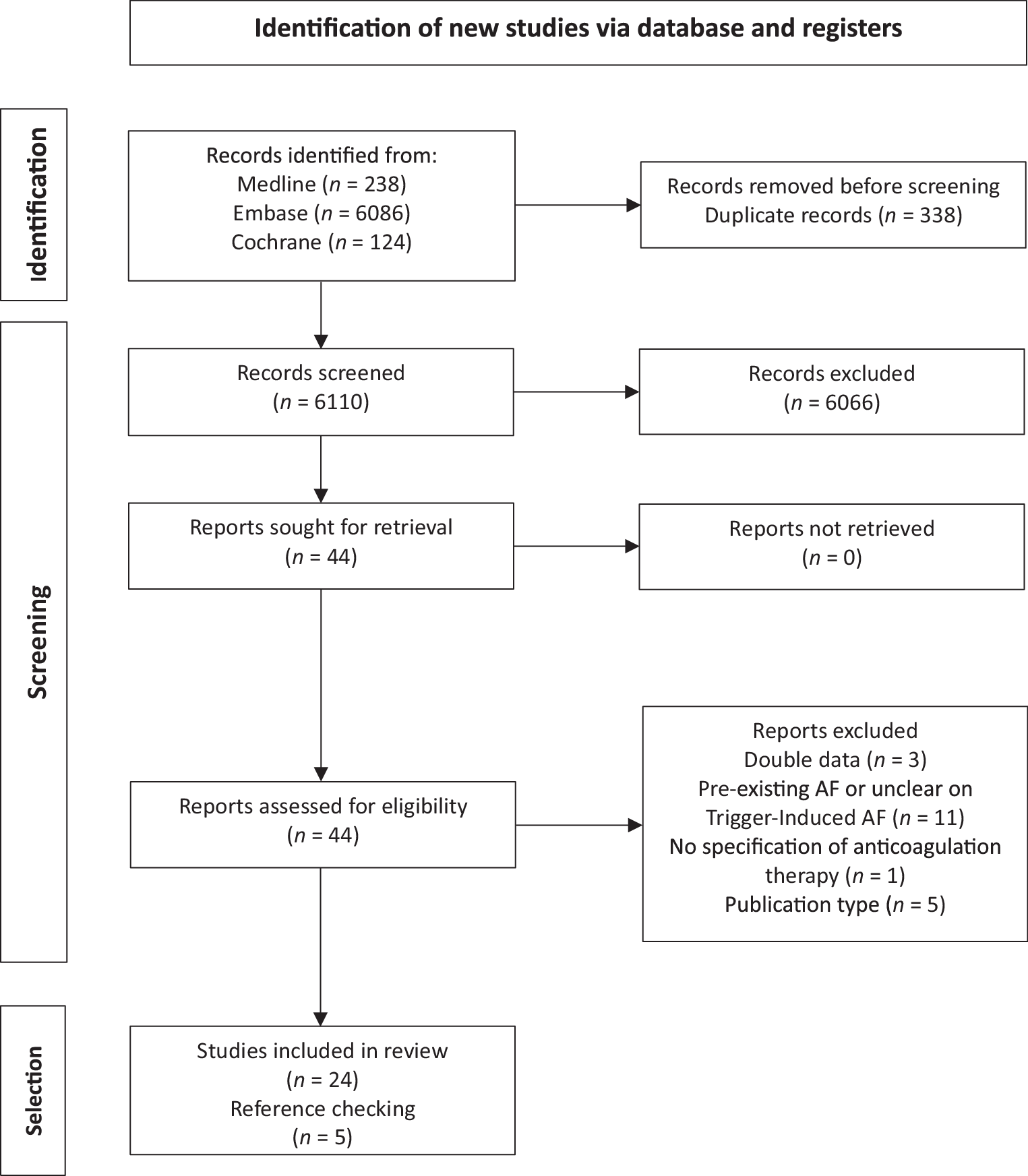
First, due to the paucity of data with a high potential for bias, only three or four eligible studies were identified for each outcome (thromboembolism, bleeding, mortality) and time frame (short-term and long-term). Second, heterogeneity was present, as the patient population and follow-up varied considerably between publications. Although most patients were admitted with sepsis or infection (approximately 95%), a proportion of those classified as critically ill had no documented underlying disease. Third, no publications included in the meta-analysis reported on the severity or sequelae of thrombotic and bleeding events, precluding a more detailed assessment of the overall risk-benefit profile of anticoagulation. Fourth, and of importance, there is no clear standardized definition of trigger-induced AF or secondary AF. Recently, the term trigger-induced AF has been adopted by the 2024 European guidelines, and ‘acute AF’ was used in a scientific statement of the AHA. It was defined as “AF detected in an acute care setting or during an acute illness” [2, 4]. This term was explicitly introduced to avoid the need to determine if the atrial fibrillation is truly (temporarily) triggered by the acute illness or has simply been undiagnosed until that moment. This dilemma is applicable to most patients in the existing literature and consequently to our current analysis.
No randomized controlled trials are underway that address anticoagulation in patients with trigger-induced AF, both for the short term (during hospitalisation) and the long term (after discharge). Due to the low incidence of the primary endpoints, such trials will require the enrolment of thousands of patients and may not be forthcoming in the foreseeable future. More importantly, due to the heterogeneity of acutely hospitalised patients, no single best strategy for all trigger-induced AF cases will likely ever be identified. To make meaningful progress, we should first prioritize prediction and risk stratification.
Future research should focus on the predictive value of a prolonged in-hospital or post-discharge monitoring period for long-term AF recurrence. Ultimately, a comprehensive approach to decision-making should also incorporate thromboembolic risk stratification. For now, it remains unclear if the CHA2DS2-VASc score is a reliable predictor of thromboembolic complications in this patient category. Efforts should be made to either validate or improve the performance of available risk scores. This may help to avoid exposing patients with low thrombotic risk and those without recurrent AF to anticoagulants.


Comments (0)