
Remember me

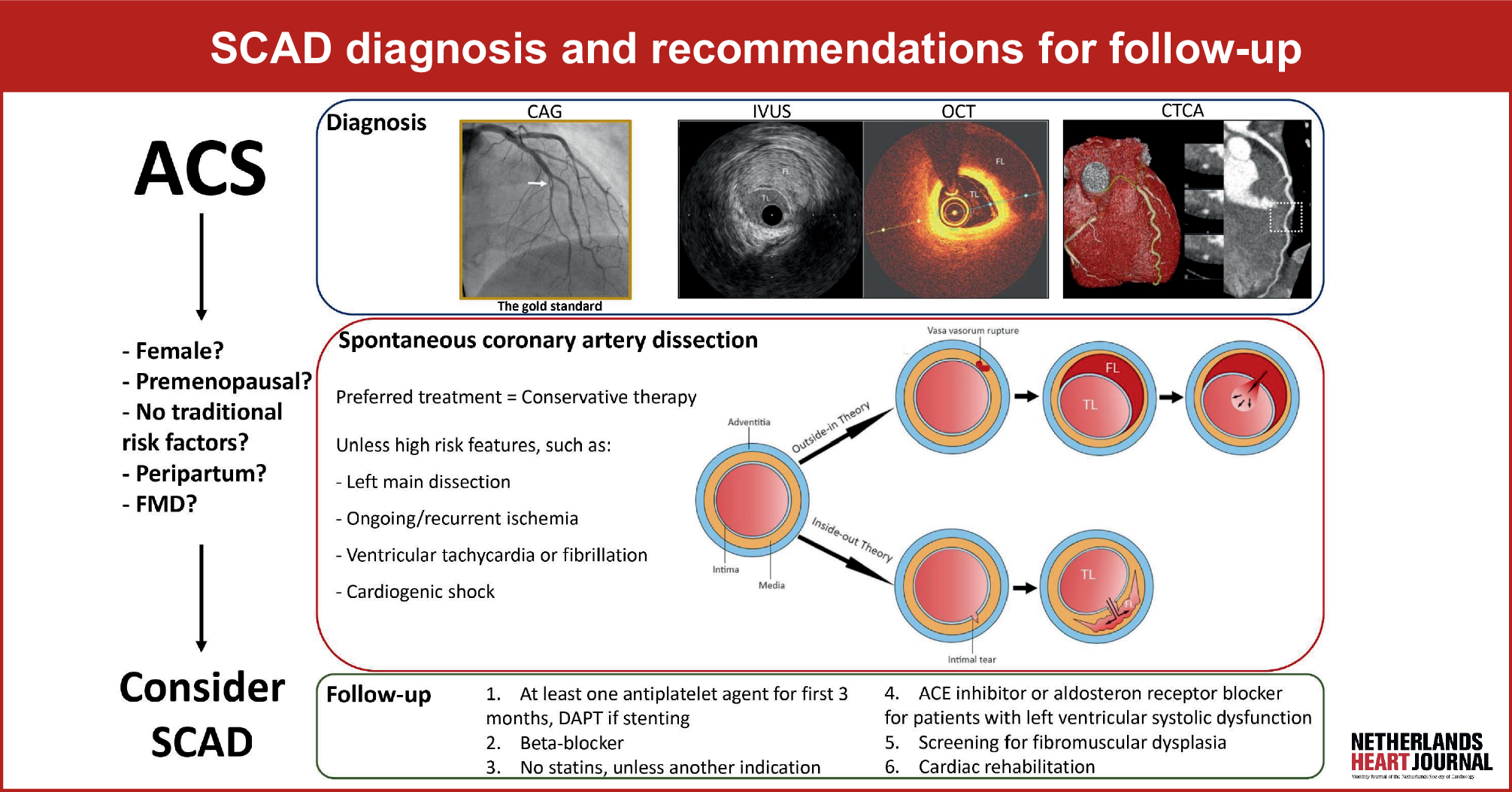
SCAD is caused by a spontaneous loss of vessel wall integrity [7]. Two hypotheses have been proposed for the pathological process the ‘inside-out’ and the ‘outside-in’ hypotheses. The ‘inside-out’ hypothesis suggests that due to a tear of the intima, blood enters the subintimal space from the true lumen, forming an intramural hematoma (IMH). The ‘outside-in’ hypothesis suggests a de novo IMH in the media due to a hemorrhage of the vasa vasorum [1]. Irrespective of the mechanism of IMH formation, the final common pathway for ACS is obstruction of the coronary blood flow by the expanding hematoma or dissection flap.
It is suggested that increased shear stress of the coronary vessel wall, together with increased catecholamines, and in some cases elevated intra-abdominal pressure, leads to SCAD, especially if there is a pre-existing arteriopathy such as fibromuscular dysplasia (FMD) [8]. Up to two-thirds of SCAD patients have FMD, [7, 9] a non-inflammatory, non-atherosclerotic syndrome, which leads to arterial stenosis, occlusions, aneurysms, dissections, and tortuosity [10]. The most affected arteries are the renal and carotid arteries [10]. There is no clear cause, but FMD is associated with a single-nucleotide variant of the PHACTR1-gene [9]. which has been associated with migraine headaches, FMD, and cervico-cerebral artery dissections [11]. Other causes of SCAD are much less frequent but can include connective tissue disorders, systemic inflammatory diseases, pregnancy-related SCAD, or hormone-associated SCAD [12].
In 3.5% of SCAD patients, there is a suggestive pathological genetic variant, mostly found in the genes associated with other syndromes such as Ehlers-Danlos, Loeys-Dietz, or polycystic kidney disease [13, 14]. A recent analysis of healthy controls, individuals with sporadic SCAD, and thirteen families with SCAD-affected patients revealed that common genetic variants (7 single-nucleotide variants) may predispose to SCAD [15].
SCAD is associated with the peripartum period and progesterone and estrogen therapy [16]. These hormones may cause changes in the vascular function and structure. Progesterone is hypothesized to increase the deposition of non-collagen proteins and estrogen, decreasing elastin and collagen deposition, resulting in weakening of the vessel wall [17, 18]. Pregnancy-related SCAD occurs between early pregnancy and 18 months postpartum, with the highest incidence within 6 weeks after delivery. Pregnancy-related SCAD constitutes 5–17% of all SCAD cases [19]. Increased cardiac output and circulating volume, and acute hemodynamic changes all increase the chance of SCAD [20].
Of the traditional risk factors for atherosclerosis, only hypertension is associated with the occurrence of SCAD [19]. Approximately 30% of SCAD patients have hypertension, which—in part—may be related to the concurrent presence of renovascular FMD [21].
Classification of SCADThe current classification [22,23,24] in four groups is as follows (Fig. 2):
1.Multiple radiolucent lumina.
2.Diffuse stenosis of varying severity and length, which may be bordered by normal artery segments proximal and distal to the IMH (type 2A) or may extend to the apical tip of the artery (type 2B).
3.Focal or tubular stenosis (typically < 20 mm) that mimics atherosclerosis and requires intracoronary imaging to confirm the diagnosis.
4.Total distal occlusion of the coronary vessel or other occlusions not meeting the criteria for types 1 to 3.
Fig. 2
Four different subtypes of SCAD by Adlam et al. [24]. Panel A: Type 1 SCAD, panel B: Type 2A SCAD, panel C: Type 2B SCAD, panel D: Type 3 SCAD, panel E: Type 4 SCAD, and panel F: Intermediate Type 1/2 SCAD
Fig. 3
SCAD management algorithm. Adapted from Saw et al. [1] SCAD spontaneous coronary artery dissection, LAD left anterior descending artery, PCI percutaneous coronary intervention, IABP intra aortic balloon pump, ECMO extracorporeal membrane oxygenation, LVAD left ventricular assist device, ICD: implantable cardioverter defibrillator, CABG coronary artery bypass grafting
Type 2 is the most frequently observed type of SCAD (± 60%).
PrevalenceThe exact prevalence of SCAD is unknown, due to underreporting of this cause of ACS [1, 25]. Most reports acknowledge SCAD as the cause of ACS in up to 4% of ACS cases, and in 0.5% as a cause of sudden cardiac death. In women under 50 years of age, SCAD is reported to be the cause of ACS in 22–43% of cases [21]. SCAD is rarely observed in patients younger than 25 or older than 80 years.
Signs and symptomsThe clinical presentation of SCAD patients is similar to that of ACS, with symptoms of chest pain with radiation, nausea, and vomiting [21, 26]. In 25–50% of cases, ST-segment elevation can be found on the electrocardiogram. Up to 90% of SCAD patients present with ACS, approximately half of patients present with ST-segment elevation MI (STEMI), and about half with non-ST-elevation ACS [27]. Emotions, physical stressors, but also drugs such as amphetamines and cocaine, childbirth and Valsalva maneuver could trigger SCAD. Nine percent of patients present with ventricular tachycardia/fibrillation [21]. Incidence of cardiogenic shock has been reported between 1.2% and 15.9% of the cases, with a higher percentage in peripartum SCAD (20–24%). These peripartum patients are reported to be younger and more likely to have connective tissue disorders than patients without cardiogenic shock.
Diagnostics and acute treatmentLaboratory testing can show elevated troponin levels. Coronary angiography remains the diagnostic tool of first choice [24]. Recent publications have reported computed tomography coronary angiography (CCTA) as a non-invasive alternative technique for invasive angiography that might be preferable over angiography in stable patients without STEMI or rise of serum troponin level or worsening chest pain because of less chance of complications related to the coronary angiography [28, 29]. However, sufficient spatial and temporal resolution is needed for adequate assessment of SCAD on CCTA [30].
It remains challenging to recognize SCAD, as it can mimic atherosclerotic disease or vasospastic angina [22]. Coronary artery spasm may resemble type 2 SCAD on invasive angiography. Administration of intracoronary nitroglycerin can help discriminate between the two entities, as coronary artery spasm usually resolves with nitroglycerin. Type 3 SCAD can look like focal atherosclerosis. In these cases, optical coherence tomography (OCT) or intravascular ultrasound (IVUS) can allow for better insight into the cause of the ACS [2]. Though OCT use should be performed by experienced operators, since contrast injections can worsen vessel occlusion. The left anterior descending artery, particularly in the mid or distal section of the coronary artery, is affected in about 50%; the circumflex coronary artery in about 30%; and the right coronary artery in about 25%. Multivessel location occurs in about 15%, and the left main coronary artery is affected in about 4% [21]. SCAD of the left main and left anterior descending artery (LAD) has been observed more frequently in shock patients [31]. Distal vessels are more commonly affected than the proximal vessels. In a propensity-matched analysis of 11 patients with SCAD and 11 healthy patients with coronary artery assessment with CCTA more tortuosity and a sharper angle between the LAD and the adjacent arterial branch was observed in the SCAD group [32].
In 70–97% of cases, a conservative approach results in complete healing of the vessel wall [33]. Only in patients with ongoing ischemia or cardiogenic shock should revascularization be considered (Fig. 3, [34]). Percutaneous coronary intervention (PCI) is associated with more complications and less angiographic success as compared with PCI for atherosclerotic lesions. Unintended wiring of the false lumen may occur, and balloon dilatation and/or stent placement in the false lumen can lead to propagation of hematoma and vessel occlusion requiring emergent coronary artery bypass grafting (CABG). Moreover, after healing of the IMH stent, malposition can lead to increased risk of stent thrombosis. CABG is technically challenging in dissected vessels; it is a temporizing measure and long-term graft patency is a concern [16]. A scientific statement from the American Heart Association states that prolonged hospitalization of 3 to 5 days for monitoring of the hemodynamics and ischemia (risk of dissection extension or new recurrent SCAD) in patients is justified as part of the conservative treatment strategy [2]. The 2023 European Society of Cardiology (ESC) guidelines for the management of acute coronary syndromes do not give recommendations for the duration of monitoring in-hospital for SCAD patients [35].
Clinical outcomesIn-hospital recurrent myocardial infarction occurs in 1.9% of conservatively treated patients and 17.9% of patients undergoing PCI during hospitalization [36]. Post-discharge major adverse cardiac event (MACE, consisting of death, recurrent acute myocardial infarction, unplanned revascularization, stroke/transient ischemic attack, and congestive heart failure) rates were reported in approximately 3% within 30 days in the non-PCI group and 26.4% in the PCI-treated group [36]. The recurrence rate for SCAD is 10–20% within 3 years [21, 37, 38]. In 75–90% of the recurrent cases, the dissection is observed in another coronary segment. Hypertension is associated with a higher recurrence of SCAD [39]. Moreover, patients with pregnancy-related SCAD have worse clinical outcomes than patients with non-pregnancy-related SCAD. One in seven patients with pregnancy-related SCAD experiences a new SCAD during a subsequent pregnancy [20, 40].
Long-term outcomes have been described in the largest SCAD registry from Canada, including 750 patients, which showed a mortality rate of 0.8%, recurrent myocardial infarction in 9.9% and major adverse cardiac events in 14.0% during 3‑year follow-up [36]. Congestive heart failure was reported in 1.9% of patients and severe ventricular arrhythmia in 4.4% of patients at 3‑year follow-up [36].
Follow-up and long-term treatmentThe 2023 ESC guidelines for the management of acute coronary syndromes recommend, in the absence of randomized controlled trials in SCAD patients, they receive the same pharmacological therapy as other ACS patients [35]. Moreover, SCAD patients with left ventricular dysfunction should be treated according to standard heart failure guidelines [41], and those receiving stents should be treated according to guidelines for PCI management. Based on observed longitudinal associations in registry data, the use of aspirin and beta-blockers is recommended.
The DISCO (DIssezioni Spontanee COronariche) registry showed that dual-antiplatelet therapy was associated with higher adverse cardiac events compared to single antiplatelet therapy, surprisingly driven by higher numbers of non-fatal MI and unplanned PCI. It is important to note that the DISCO trial was a relatively small retrospective cohort with differences between the groups (e.g., more type I SCAD) [42]. Lifelong beta-blocker therapy, if tolerated, can be justified based on a retrospective study in which its use was associated with lower rates of SCAD recurrence [43]. Cardiac rehabilitation should be considered in all patients, and special emphasis should be placed on assessing mental health in patients after SCAD [44,45,46]. Large regional and global variations in treatment of SCAD patients have been observed, with regard to medication prescriptions and FMD screening [41]. Currently, no guideline recommendations are available to patients with peripartum SCAD and following pregnancies. Though a viewpoint written by Tweet et al. stated that women of childbearing age after SCAD should be counseled to avoid future pregnancy [47]. The authors based this advice on the high recurrence rates in SCAD patients, lack of prediction models to predict who is at risk of recurrence, and due to the fact that the clinical course of pregnancy and postpartum SCAD is more severe than other SCAD [47]. As this advice has a great impact on the lives of SCAD patients, we suggest that shared decision making should be the aim of pregnancy counseling.
Patients should be screened at the outpatient clinic for the presence of FMD. In the Netherlands this is preferably done by an internal medicine doctor in a specialized FMD center. Screening is mostly performed with CT angiography to detect stenosis of the arteries, such as the carotid and renal arteries. Genetic testing for FMD is not performed routinely because of the lack of clinical implications. Follow-up of FMD consists of strict blood pressure management [10].
Comments (0)