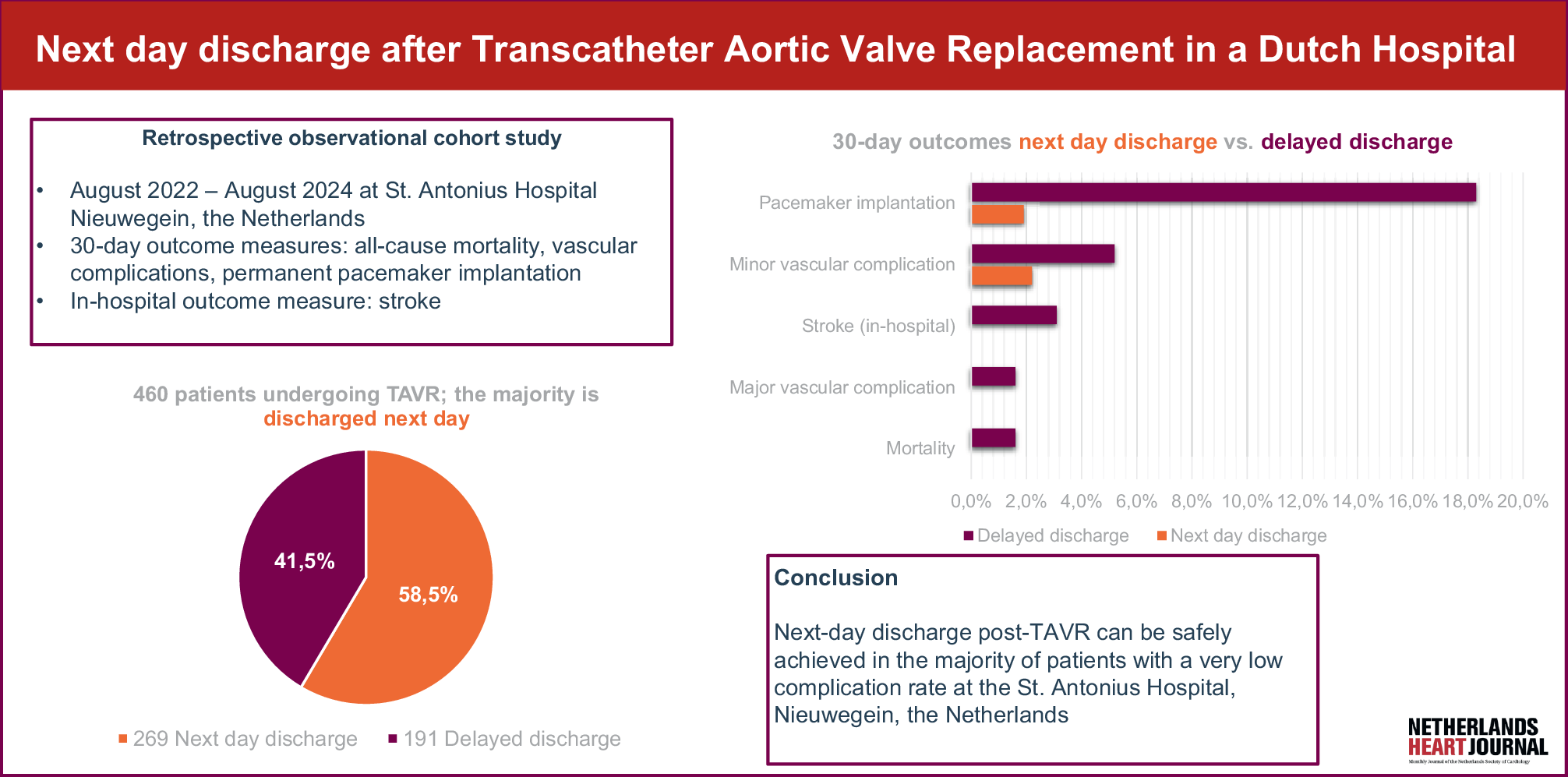
Previous studies identified NDD following TAVR as a safe strategy [6, 13,14,15]. As no Dutch data on NDD after TAVR exist from any hospital in the Netherlands, we evaluated its real-world effect on feasibility, timing, and short-term outcomes.
This study found low post-discharge complication and mortality rates in the NDD group. NDD was achieved in 269 (58.5%) patients. NDD rates vary across studies. Some report higher rates (72% [13], 80% [14]), but excluded patients with pre-existing RBBB, prolonged PR interval, AV block [13], or inadequate social support or mental stability [14]. In this study, NDD was the intended strategy for all TAVR patients, which may have contributed to a lower NDD rate.
The study population differed in three baseline variables. The NDD group included significantly fewer females compared to the DD group (36.4 and 47.1% respectively). Previous studies confirm that female sex is a negative predictor of NDD [13], as females often experience more bleeding and more vascular complications post-TAVR [16]. However, no sex-based differences in vascular complications were observed in this study.
Patients in the NDD group were less frail, with a median EFS score of 2.0 compared to 3.0 in the DD group. This aligns with findings by Holierook et al., which linked higher frailty scores to prolonged hospital stay [17]. Unlike other NDD safety studies [13, 14], we did not preselect based on social support, which is reflected in the EFS score and may explain group differences.
More patients in the DD group (13.1% versus 4.1% respectively) had a pre-existing RBBB. RBBB is a well-known predictor for the need of a PPI after TAVR [18], which may have caused a longer hospital stay in the DD group.
In this study, no cases of 30-day mortality were found in the NDD group. The overall 30-day mortality rate in this study was 0.7%, which is comparable to the findings of Eaves et al. [13]. Both studies reported no cases of mortality in the NDD group and found no significant difference between the two groups.
The incidence of PPI within 30 days post-TAVR was low in the NDD group (1.9%). PPI rates with NDD after TAVR ranged from 0 to 15.5% in the meta-analysis of Gupta et al. [6]. The occurrence of conduction disorders during or after TAVR often requires prolonged ECG monitoring or sometimes PPI, reflected in a higher rate of PPI in the DD group (18.3%), p < 0.001. Similar trends were reported in other studies [6, 13, 19].
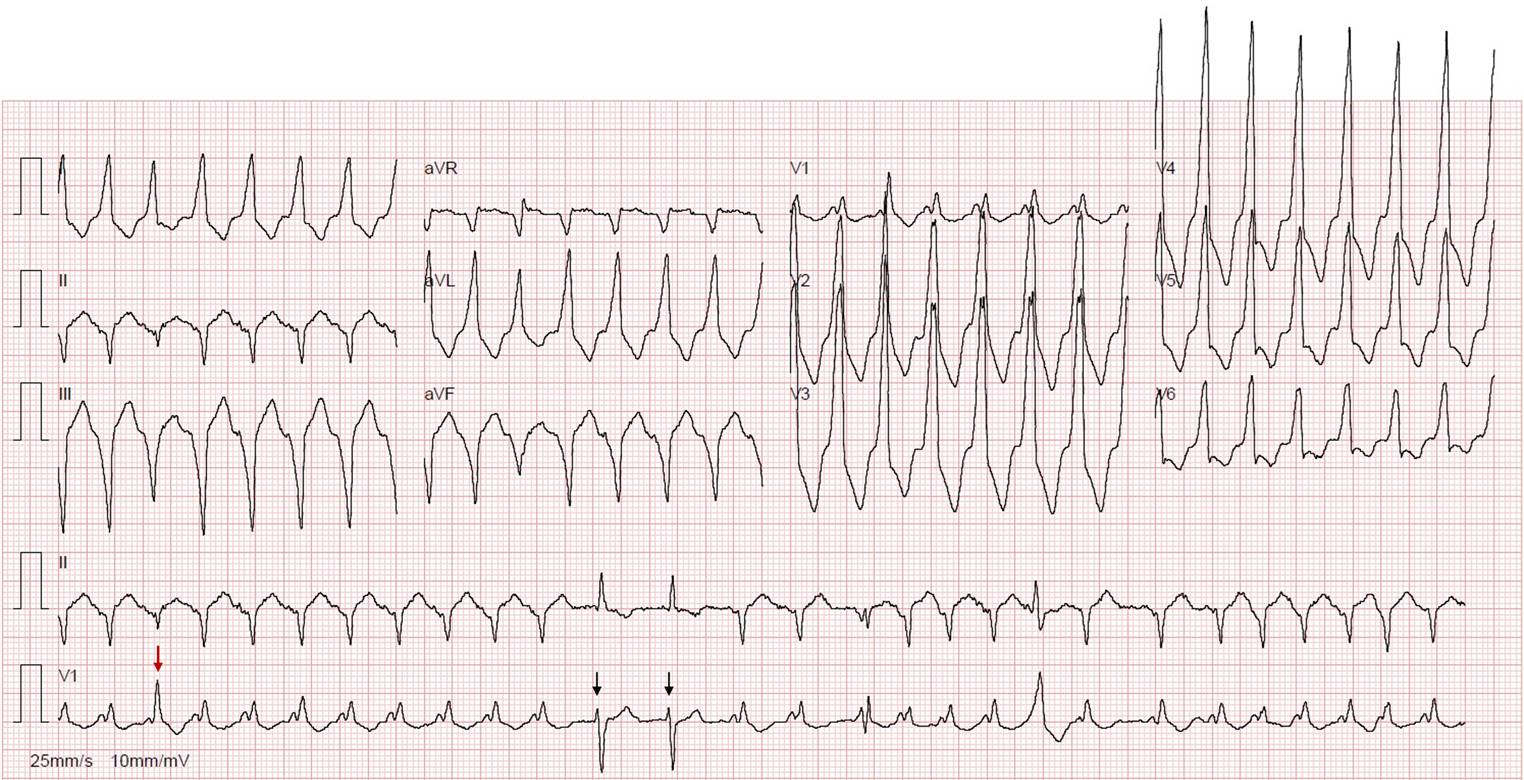
Patients were readmitted with complaints of bradycardia, dizziness, and hypotension, most commonly due to 3rd degree AV block. All patients in the NDD group who received a permanent pacemaker were readmitted to the hospital between one and seven days post-discharge. Patients were discharged following the ESC guidelines on cardiac pacing and resynchronisation therapy 2021 [10], except for one patient. This patient showed a new LBBB with a QRS duration exceeding 150 ms after TAVR and, therefore, should have been monitored longer. However, the patient was readmitted with symptoms of bradycardia seven days after discharge, suggesting that 48 h of prolonged monitoring would not necessarily have altered the outcome.
Additionally, the rate of vascular complications was low in the NDD group. Respectively, 0.0 and 2.2% major and minor vascular complications occurred in the NDD group. The rates were higher in the DD group with 1.6 and 5.2% major- and minor vascular complications, respectively (p = 0.02). Especially major, but also minor vascular complications could be a reason for additional intervention and prolonged hospital stay. Two studies reported similar findings regarding differences in vascular complications between the groups [6, 13]. In contrast, the study of Ordoñez et al. found no difference in major vascular complications between both groups (p = 0.32) [19], and Eaves et al. found 1.5% major vascular complications in the NDD group [13].
In the NDD group, there were no patients with in-hospital stroke, whereas six patients (3.1%) had a stroke in the DD group (p = 0.004). Other studies found no significant difference in stroke. However, this outcome was measured at 30 days instead of in-hospital [6, 13, 19].
In summary, this study’s findings align with previous research. The low post-discharge complication rates in the NDD group in this study are consistent with expectations, as complications such as PPI, vascular complications, and stroke require prolonged observation or additional interventions during the post-TAVR hospital stay.
In our opinion, these findings likely apply to other Dutch TAVR-implanting hospitals, as both international and current data support the feasibility and safety of NDD. The results of this study did not prompt any changes to the discharge protocol.
The main limitation of this study is its single-centre, retrospective design. Second, bias may have been introduced because patients were selected for NDD by different physicians. However, all physicians followed the European guidelines and the aim of this study was to assess the practices in a real-life Dutch hospital setting.
Further research should explore factors contributing to prolonged hospital stay, including the timing of complication onset. Understanding the reasons behind prolonged hospitalisation could further optimise post-TAVR discharge protocols. Home monitoring to detect any arrhythmias and conduction disturbances could be explored.


Comments (0)