
Remember me



In 2018, head and neck cancer (HNC) was the seventh most common cancer worldwide.1 In the United States, it accounts for 3% of all cancers and over 1.5% of cancer deaths.2 In Taiwan, it ranked seventh in incidence and fifth in mortality in 2020.3 It is approximately 2 to 4 times more common in men than in women worldwide and increases with age, especially after the age of 50.4,5 However, according to the 2021 Cancer Registry Annual Report in Taiwan, the incidence rate of oral cavity, oropharynx, hypopharynx, and lip cancer in men is about 8 to 10 times higher than in women.6 Currently, its treatment plan helps determine the expected treatment path. Its patients mainly receive surgical treatment in the early stages, and radiotherapy and chemotherapy in advanced stages. When patients receive anticancer treatments, the side effects—severe mucositis, difficulty in opening the mouth, dry mouth, myelosuppression, pain, vomiting, malnutrition, and infection—that commonly occur can cause short, long, or even lifelong effects, depending on the type of treatment.
These patients may have difficulty in swallowing because of the disease, its treatment, or both, which can cause a significant burden of morbidity. Besides physical symptoms, they often have personal behavioral problems, including tobacco and alcohol dependence and complex psychosocial problems,7,8 which can affect their quality of life (QoL) and even cause them to refuse/interrupt treatment, thereby affecting its effectiveness, and their survival. While palliative care improves the QoL of patients and their families, facing disease-related challenges, whether physical, psychological, social, or spiritual, it is well known that it is particularly appropriate for patients with HNCs.7
Early palliative care (EPC) should be initiated early (ie, within 8 weeks of diagnosis).9,10 According to some treatment guidelines, patients with early or advanced-stage cancers should receive high-quality palliative care provided by the primary oncology team during initial diagnosis. Highly symptomatic patients should be referred to a co-care team for interdisciplinary palliative care.11–13 Studies in Western countries14–20 reveal that EPC improves advanced-stage cancer patients’ QoL, physical symptoms, communication with their physicians, emotional distress, patient satisfaction, end-of-life care quality, survival rates, and benefits caregivers.14,15,17,21–24 However, evidence shows that racial and ethnic disparities exist in accessing high-quality palliative or EPC, and clinical outcomes, such as symptom management and communication.25–27 In Eastern countries, its effectiveness and benefits among patients with early-stage HNCs are unclear. This study aimed to investigate the effects of EPC in improving symptoms, emotional distress, QoL, depressive symptoms, and anticancer treatment compliance in Taiwanese patients with early or advanced-stage HNCs.
2. METHODS 2.1. Study populationThe study was approved by the Ditmanson Medical Foundation Chia-Yi Christian Hospital’s ethics committee (approval number: CYCH-IRB-2020070). Those enrolled had to meet the following criteria: (a) stages I to IV HNC (within 8 weeks of a physician’s diagnosis based on radiological/histological information), (b) aged over 20 years and willing to cooperate, (c) having a HNC treatment plan, and (d) literate/able to communicate in Chinese and/or Taiwanese, and understand the questionnaire’s contents. Patients clinically diagnosed as comatose, having mood disorders/psychotic illness, or too weak/unwell to complete the survey, were excluded.
There are 393 patients diagnosed and treated with HNC at Taiwan’s Chia-Yi Christian Hospital from November 2020 to October 2022. We introduced this study to them and 93 patients agree to join this study. Most of 300 patients who refuse to joint this study due to they felt current multidisciplinary cancer treatments were satisfied and enough. Another reason they refuse to joint this study was impatient to complete four Multiple-symptom assessment tools (The Taiwan version of the MD Anderson Symptom Inventory [MDASI-T], The Chinese version of the Distress Thermometer [DT], The Chinese version of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 [EORTC QLQ-C30], and The Taiwan Chinese version of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Head and Neck 35 [EORTC QLQ-HN35]) in different four times.
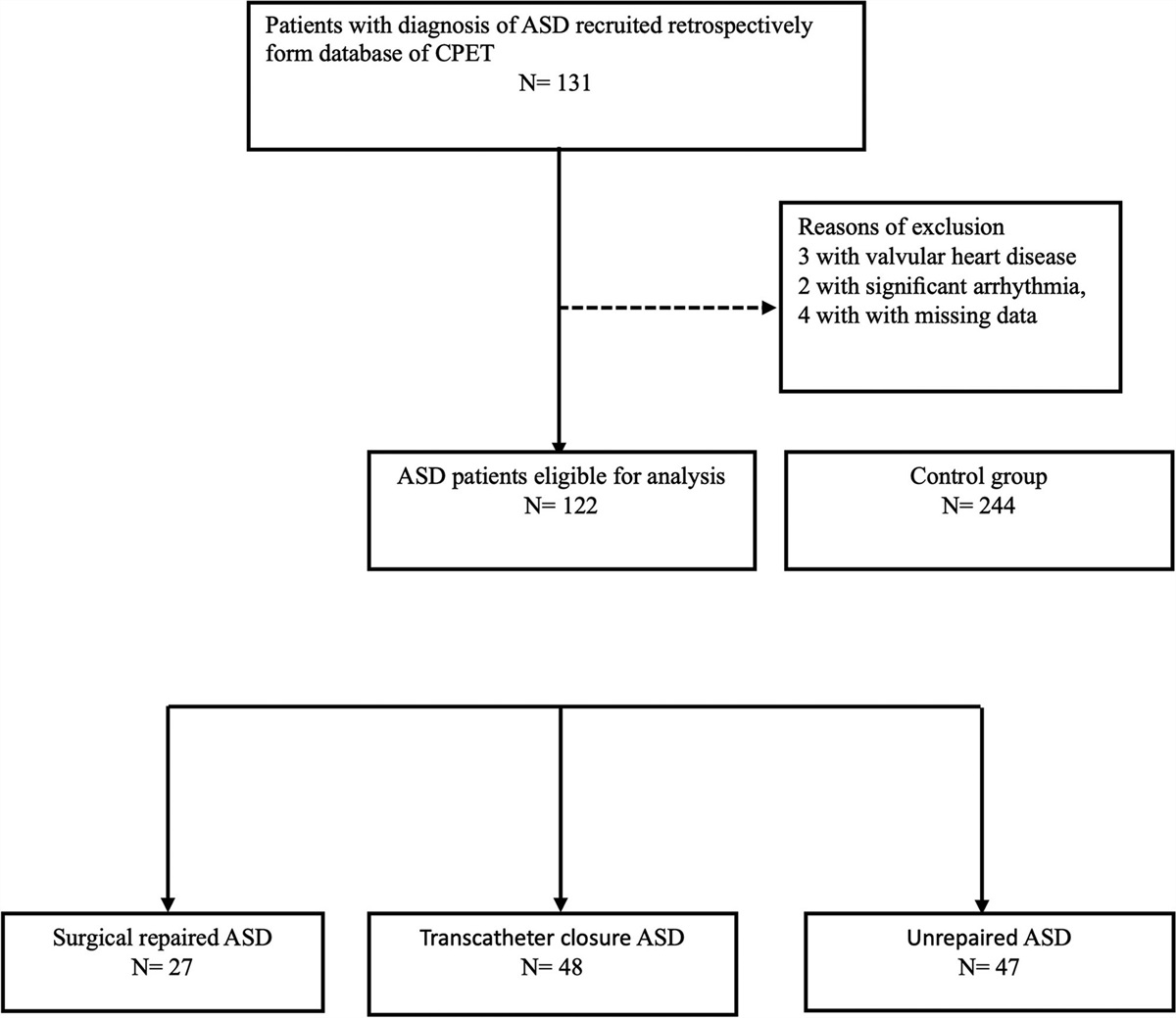
2.2. Study design and EPC interventionThe researcher explained the study’s content, purpose, and interventions to those meeting the acceptance criteria. After obtaining their consent and signature on the consent form, the oncology case manager, attending physician and/or EPC physician assessed their symptoms. The participants who were willing to receive EPC were assigned to the EPC group, and those unwilling were used as the standard group. Each group was subdivided into early (stages I-II) and advanced (stages III-IV), according to the physician’s diagnosis. The questionnaires were simultaneously administered four times to both groups: T0: before the EPC intervention; T1: a month after the intervention; T2: 3 months after the intervention; and T3: 12 months after T0 (Fig. 1).
 Fig. 1:
Fig. 1: Diagram displaying cohort recruitment and status of patients receiving EPC or standard at baseline, 1 mo (T1), 3 mo (T2), and 12 mo (T3). EPC = early palliative care; HNC = head and neck cancer.
2.3. EPC interventionOncology case managers and EPC physicians must complete an EPC education and training course. The team that assists in EPC includes clinical psychologists, social workers, nutritionists, rehabilitation therapists, pharmacists, religious teachers, hospice specialists, psychiatrists, medical oncologists, and surgical oncologists.
The oncology case manager visits each newly diagnosed HNC patient and provides relevant assessment and health education in nursing, nutrition, rehabilitation, and other aspects. The service includes patients in the EPC and standard groups. In the standard group, the patient’s attending physician evaluates whether it is necessary to consult relevant medical departments for multispecialty team treatment based on the patient’s condition assessment.
The original oncology team routinely questions patients about their symptoms and discomfort. Physicians tend to rely on their preferred habits or medical practices during these inquiries. As a result, there may be fewer questions compared to the “Consultation reconfirmation form.” For patients in the EPC group, in addition to the patient’s primary physician assessing the patient’s needs, another fully trained EPC physician conducts a systematic assessment of the patient’s condition. To avoid missing clinical assessments, EPC physicians must perform individual assessments based on the “Consultation reconfirmation form” including troubles related to cancer diagnosis and treatment; pain condition; emotional problems; gastrointestinal problems, respiratory problems, neurological problems, dermatological problems, and other clinical problems; nutrition, economics, spirituality, and other issues (Supplementary Fig. S1, https://links.lww.com/JCMA/A255). Based on the results of the assessment, the EPC physician needs to communicate with the original care team what items require ongoing monitoring. If treatment is necessary, the EPC physician can directly administer it or refer it to the original treatment team. If the assessment results require the assistance team described above, the EPC physician or the original treatment team can initiate a consultation mechanism. The oncology case manager and EPC physician establish goals and timelines for tracking the effectiveness of the patient issues listed above and engage in proactive tracking and follow-up (every 4 weeks over a 12-month period) (Fig. 1). If the participants rejected the questionnaire’s evaluation, subsequent EPC was discontinued (stop follow-up). The EPC will ask questions sequentially, following the “Consultation reconfirmation form”. If probed further, the patient will elaborate on their discomfort or consider if the symptoms queried by the doctor persist. This process aids the doctor in understanding the patient’s condition and potentially adjusting the medication.
2.4. Multiple-symptom assessment tools 2.4.1. The Taiwan version of the MD Anderson Symptom InventoryIt is reliable and valid, and mainly measures the severity of Taiwanese patients’ cancer-related symptoms and their interference with daily life. The Cronbach’s α was 0.89 and 0.94 for symptom severity and interference items, respectively; whereas test-retest reliability was 0.97 and 0.96 for the severity and interference composite scores, respectively.28
2.4.2. The Chinese version of the DTIt has been tested (Supplementary Fig. S2, https://links.lww.com/JCMA/A255) by psychiatrists using four cut-off points and the Hospital Anxiety and Depression Scale, and the results showed that its sensitivity for anxiety and depression screening was 98% with a specificity of 73%.29 It is a short, quick, and easy-to-interpret self-reporting tool developed by the National Comprehensive Cancer Network for psychological and emotional screening of cancer patients.30 To avoid excessive referrals owing to a lack of psychologists in the research field, a score of ≧5 is taken as the cut-off point, and subsequent referrals to psychologists or other EPC team members is carried out under the Patient Problem List case-by-case.
2.4.3. The Chinese version of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30Its version 3 was used to assess the physical health and QoL of patients with HNC. Its 30 items cover 15 domains: five function scales, nine symptom scales/items, and one global health/QoL scale.31 Sociodemographic data were analyzed descriptively. The calculated mean scores of the 15 EORTC QLQ-C30 subscales were transformed to a range between 0 and 100.32 A 10-point difference on a scale of 0 to 100 was considered clinically significant, and a greater than 20-point difference was considered a very significant change according to Osoba et al’s33 recommendations. Thus, high scores on the functional, global health status/QoL, and symptom scale/item represent high/healthy levels of functioning, QoL, and symptomatology/problems, respectively.
2.4.4. The Taiwan Chinese version of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Head and Neck 35This 35-item module34 incorporates seven multiple-item scales that assess symptoms of pain in the head and neck, swallowing ability, senses (taste/smell), speech, social eating, social contact, and sexuality; and six single-item scales, which survey the presence of symptomatic problems, associated with teeth, mouth opening, dry mouth, sticky saliva, coughing, and feeling ill. All the EORTC QLQ-HN35 scales range from 0 to 100, while 10-point differences are clinically relevant.35 A high score on the symptom scale indicates the presence of symptoms or problems. Osoba et al33 recommend considering a 10-point difference on a scale of 0 to 100 as clinically significant.
2.5. Statistical analysisAll analyses were performed using SPSS version 28.0 (SPSS Inc., Chicago, IL). The variables analyzed included basic demographic data, diagnosis, treatment modality, family social support, and daily living functions. The Mann-Whitney U test and Friedman test were used for nonparametric two-way analysis of variance (ANOVA) for ratio-related samples. It was used to test differences between the EPC and standard groups in terms of symptoms, psychological distress, and pretest scores on QoL. A paired t test was performed to compare the differences in QoL between T1, T2, T3, and T3 vs T0.
The generalized estimating equation was used to examine whether the physiological symptoms, emotional distress, and QoL of the EPC and standard groups were different postintervention, and after controlling for interference factors, for exploring differences between both groups, including the effect of improving physical symptoms, emotional distress, and QoL after a period of 1, 3, and 12 months of the intervention. p < 0.05 was considered statistically significant.
3. RESULTS 3.1. Participants’ characteristicsPatients were randomly assigned to two groups according to their preferences. Those who were willing to join became part of the EPC group, while the others were assigned to the control group. Early-stage and advanced-stage HNC are discussed separately, given that different treatment methods yield different side effects and symptoms for each stage. Ninety-three HNC patients were recruited and divided into the EPC (n = 69; early n = 23, advanced n = 46) and standard groups (n = 24; early n = 11, advanced n = 13). Their demographic and clinical characteristics are shown in Table 1. Early-stage HNC participants’ median age was 57 and 52 years in the standard and EPC groups, respectively, whereas advanced-stage participants’ median age was 54 years in both the groups. The standard and EPC groups’ participants were mostly male (100% vs 95.7%, p = 1.00, and 92.3% vs 91.3%, p = 1.00, respectively). Among early-stage HNC participants, in the standard group 90.9% had oral cancer, whereas in the EPC group 73.9%, 8.7%, 13%, and 4.3% had oral, oropharyngeal, hypopharyngeal, and nasopharyngeal carcinoma cancers, respectively. In the standard group, 100% underwent curative surgery, whereas in the EPC group, 78.3% underwent curative surgery, 8.7% radiotherapy, 8.7% chemotherapy, and 4.3% other surgeries. Among advanced-stage participants, in the standard group, 84.6% had oral cancer, whereas in the EPC group, 50%, 13%, 15.2%, and 21.7% had oral, oropharyngeal, hypopharyngeal, and nasopharyngeal carcinoma cancers, respectively. In the standard group, 53.8%, 23.1%, 15.4%, received chemotherapy, curative surgery, and radiotherapy with chemotherapy, respectively, while in the EPC group, 39.1%, 30.4%, and 28.3% received radiotherapy with chemotherapy, curative surgery, and chemotherapy, respectively (Table 1).
Table 1 - Patients characteristic Early (n = 34) Advanced (n = 59) Standard EPC Standard EPC No. % No. % p No. % No. % p Number 11 23 13 46 Age-median (Q1-Q3)a 57 (47-61) 52 (46-62) 0.640 54 (49-58) 54 (46-61) 0.754 Sex Male 11 100.0 22 95.7 1.000 12 92.3 42 91.3 1.000 Female 0 0.0 1 4.3 1 7.7 4 8.7 Education Junior high school or below 4 36.4 12 52.2 0.638 4 30.8 30 65.2 0.019 High school 7 63.6 10 43.5 8 61.5 16 34.8 College or above 0 0.0 1 4.3 1 7.7 0 0 Current marital status Single 3 27.3 7 30.4 1.000 3 23.1 19 41.3 0.334 Married 8 72.7 16 69.6 10 76.9 27 58.7 Religion No 0 0.0 9 39.1 0.002 3 23.1 13 28.3 0.239 Buddhism 4 36.4 1 4.3 2 15.4 1 2.2 Diffused religion 4 36.4 2 8.7 1 7.7 9 19.6 Christianity 0 0.0 0 0 1 7.7 1 2.2 Taoism 3 27.3 11 47.8 6 46.2 22 47.8 Full-time/part-time jobs No 1 9.1 6 26.1 0.384 5 38.5 13 28.3 0.509 Yes 10 90.9 17 73.9 8 61.5 33 71.7 Economic status (per month) <30,000 NTD 6 54.5 12 52.2 1.000 7 53.8 28 60.9 0.497 30,000-50,000 NTD 3 27.3 7 30.4 4 30.8 15 32.6 60,000-90,000 NTD 2 18.2 4 17.4 2 15.4 2 4.3 >100,000 NTD 0 0.0 0 0.0 0 0.0 1 2.2 Caregivers support Alive alone 1 9.1 0 0.0 0.324 1 7.7 6 13.0 1.000 Caregivers care 10 90.9 23 100.0 12 92.3 40 87.0 Diagnosis Oral cancer 10 90.9 17 73.9 0.869 11 84.6 23 50 0.212 Oropharyngeal cancer 0 0.0 2 8.7 1 7.7 6 13 Hypopharyngeal cancer 1 9.1 3 13 0 0.0 7 15.2 Nasopharyngeal carcinoma 0 0.0 1 4.3 1 7.7 10 21.7 Treatment Curative surgery 11 100.0 18 78.3 0.580 3 23.1 14 30.4 0.156 Chemotherapy 0 0.0 0 0 7 53.8 13 28.3 Radiotherapy 0 0.0 2 8.7 0 0.0 0 0.0 Radiotherapy with Chemotherapy 0 0.0 2 8.7 2 15.4 18 39.1 Other 0 0.0 1 4.3 1 7.7 1 2.2 Performance status ECOG: 0 8 72.7 20 87.0 0..363 11 84.6 28 60.9 0.243 ECOG: 1 3 27.3 3 13.0 1 7.7 15 32.6 ECOG: 2 0 0.0 0 0.0 1 7.7 2 4.3 ECOG: 3 0 0.0 0 0.0 0 0.0 1 2.2ECOG = eastern cooperative oncology group; EPC = early palliative care; TWD = new taiwan dollar .
aAge was tested by Mann-Whitney U test.
EPC doctors conduct individual assessments based on the “Consultation reconfirmation form”. The results show that 68.9% were troubles related to cancer diagnosis and treatment; 31.9% were pain condition; 4.9% were emotional problems; 18.7% were gastrointestinal problems, respiratory problems, neurological problems, dermatological problems, and other clinical problems; nutritional, economic, spiritual, and other issues 14.5%. After relevant treatments were given, the consultation improvements were evaluated according to MDASI-T, DT, EORTC QLQ-C30, and EORTC QLQ-HN35.
3.2. MDASI-T single symptom and interference severity item scoresTables 2 and 3 show the evolution of its scores over time for the two groups, and the number of forms completed at each time point. Among early-stage HNC patients who underwent EPC, the scores of the DT items gradually decreased with the time of EPC treatment (4 [2-5], 3 [2-4], 2.5 [1-5], and 1.5 [0-3], p = 0.002). The symptom scores of the EPC group reduced significantly for pain (p = 0.014), nausea (p = 0.033), and distress (p = 0.047), while those of the standard group were reduced significantly for dry mouth (p = 0.048) (Table 2). For patients with early-stage HNC, the “Consultation reconfirmation form” primarily addresses unresolved issues. The form assesses items such as pain, nausea, and discomfort, but it does not include symptoms like dry mouth. Despite this exclusion, patients’ symptoms have shown significant improvement compared to the standard group.
Table 2 - Evolution of DT and MDASI-T single symptom and interference severity item scores for early head and neck cancer patients over time Standard EPC T0
Comments (0)