
Remember me



Schizophrenia is a psychiatric illness characterized by positive symptoms, negative symptoms, and cognitive dysfunction. Hippocampal dysfunction has been implicated in the pathophysiology of schizophrenia on the findings showing that the hippocampus is involved in hyperactive dopaminergic neurotransmission,1 and that psychotic symptoms are associated with neurological disorders, lesions, or electrical stimulation of certain hippocampal regions and adjacent structures.2,3
The hippocampus can be segmented into the head, body, and tail subregions along its longitudinal (anteroposterior) axis.4–6 Findings regarding the association of the reduction in hippocampal subregion volume with susceptibility to schizophrenia are inconsistent. Some reports have suggested that among patients with schizophrenia, volume reduction is more prominent in the anterior parts,7,8 whereas other studies have observed volume reduction in the mid- and posterior-regions of the hippocampus.9,10
Apart from its longitudinal segmentation, the hippocampus can be divided into distinct subfields on its transverse axis based on the basis of cytoarchitectural and magnetic resonance imaging (MRI) findings,11–14 such as the cornu ammonis (CA) 1-3, CA4, dentate gyrus (DG), and subiculum complex (the presubiculum, parasubiculum, and subiculum). These subfields play specific roles in cognitive processing, mood regulation, and neurological plasticity.14–16 Compared with HCs, patients with schizophrenia exhibited volume reductions in the CA1, CA2/3, DG/CA4, and subiculum, suggesting that the volume reduction is widespread over the hippocampal subfields in patients with schizophrenia.14–16
Antipsychotic drugs remain a major treatment for the positive symptoms of schizophrenia. Several studies have examined the relationship of hippocampal volumes and antipsychotic treatment outcome in schizophrenia. In patients with first-episode schizophrenia (FES), antipsychotic treatment was associated with reduced volumes of the bilateral whole hippocampal and several subfields (such as the bilateral molecular layers [MLs], granular cell layers of the DG and tails; left CA1 and CA3, and fimbria), but increased the subiculum volume.17,18 Bodnar et al19 showed decreased volumes over bilateral hippocampal tails were associated with inadequate symptomatic remission defined by the Remission in Schizophrenia Working Group (RSWG)20 in patients with FES after 12-month antipsychotic treatment. However, the association of symptomatic remission after antipsychotic treatment with volume changes in the hippocampal tail or other subdivisions has not been studied in patients with chronic schizophrenia.
The present study investigated volume differences in hippocampal subregions and subfields between patients with schizophrenia and HCs. In addition, we also investigated which of the hippocampal subregions and subfields was associated with RSWG-defined symptomatic remission in patients with chronic schizophrenia receiving antipsychotic treatment.
2. METHODS 2.1. ParticipantsWe recruited 31 unrelated patients with schizophrenia diagnosed per the criteria of the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) by two board-certified senior psychiatrists according to information obtained from clinical interviews with the patients and their families, clinical observations, and chart reviews. The age of the patients ranged from 20 to 65 years. We excluded patients who had a history of substance abuse (amphetamine, ketamine, 3,4-methylenedioxy-methamphetamine, opioids, or alcohol); other psychiatric illness (schizophreniform disorder, schizoaffective disorder, mood disorder, psychotic disorder due to general medical conditions, mental retardation, or dementia); and severe medical illness, including cardiovascular, hepatic, or renal diseases, poorly controlled hypertension, and diabetes mellitus. Women who were pregnant or breastfeeding were also excluded. We included 31 healthy controls (HCs) who had no symptoms or history of psychiatric illness through face-to-face interviews conducted by board-certified psychiatrists. All the participants were Han Chinese. The study followed the principles of the Declaration of Helsinki and was approved by the Ethics Review Committee of Taipei Veterans General Hospital, Taiwan. Before enrollment, the study aims and procedures were explained to the participants, and their written informed consent was obtained.
The patients in the schizophrenia group were stratified into remitted (SC-R) and nonremitted (SC-NR) groups according to symptomatic remission criteria for schizophrenia developed by the RSWG,20 which consist of two elements: time criteria (6 months) and symptom-based severity criteria. The symptom-based severity criteria encompass eight diagnostically relevant symptoms of schizophrenia from the Positive and Negative Syndrome Scale (PANSS-8): delusion (P1), conceptual disorganization (P2), hallucinatory behavior (P3), mannerisms/posturing (G5), unusual thought content (G9), blunted affect (N1), social withdrawal (N4), and lack of spontaneity (N6). Patients who score ≤3 points (mild symptom intensity) for ≥6 months on all the eight core items are considered to have symptomatic remission.20 The PANSS-8 has been validated in both clinical trials and clinical practice.21,22 All the patients in the schizophrenia group were followed up monthly for ≥6 months, during which the class and daily dose of prescribed antipsychotics were maintained. Symptomatic remission was determined by the severity scores for each item in the PANSS-8 at the sixth month of antipsychotic treatment.
2.2. MRI acquisitionStructural brain MRI data were collected using a 1.5-T GE Scanner Excite-II system (GE Medical Systems, Milwaukee, WI). T1-weighted images were acquired using the following parameters: spoiled gradient-echo sequence; repetition time (TR), 8.54 millisecond; echo time (TE), 1.836 millisecond; inversion time (TI), 400 millisecond; flip angle, 15°; matrix size, 256 × 256; field of view (FOV), 260 mm; 124 axial slices with 1.5-mm slice thickness; and resolution, 1.02 mm × 1.02 mm × 1.5 mm.
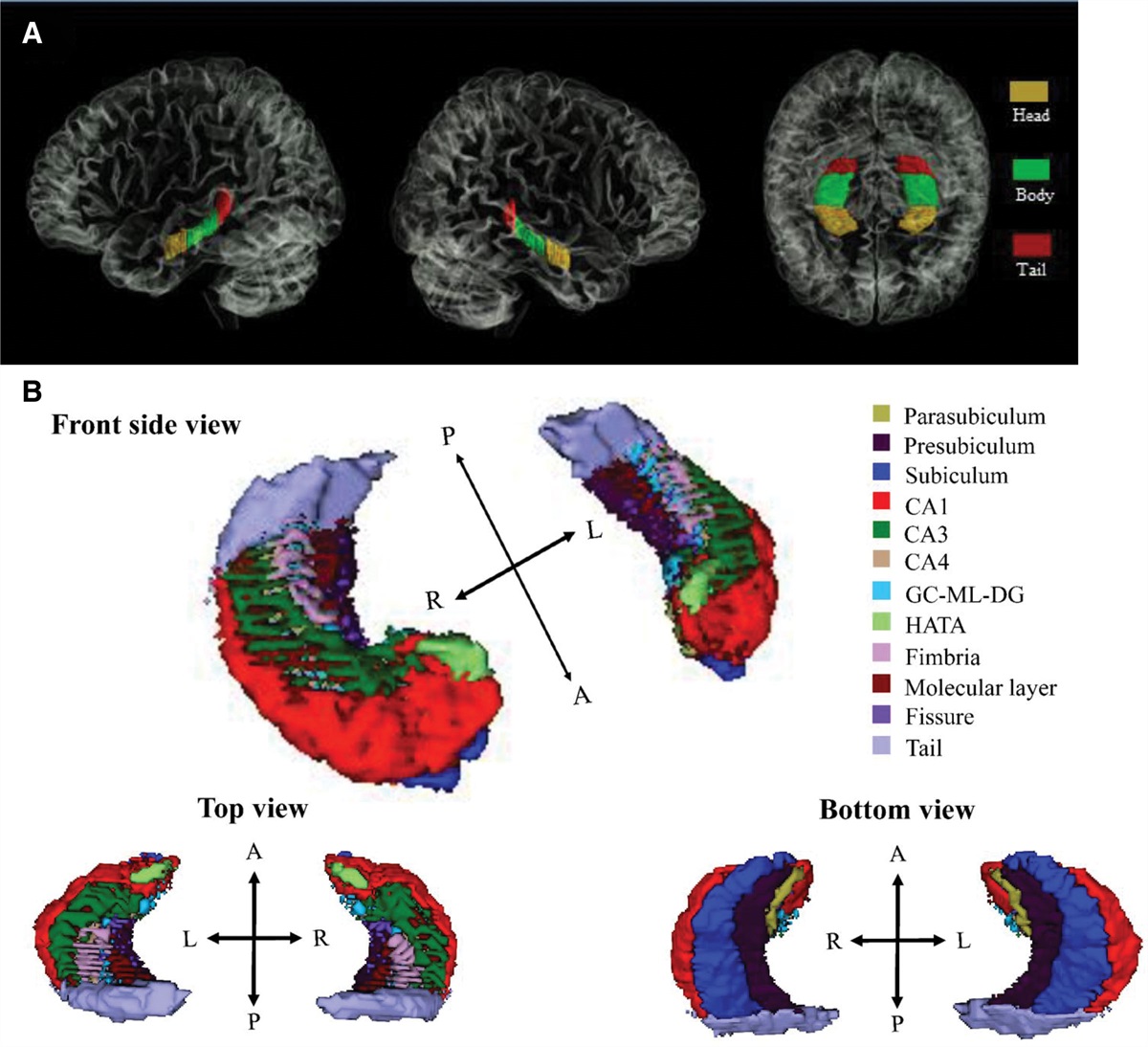
2.3. Measurement of subregion volumes along the hippocampal longitudinal axisManual hippocampal tracing was performed on the T1-weighted image by using PMOD 3.0 software (https://www.pmod.com/web/). Tracing was mainly performed on the coronal plane and the axial and sagittal planes to determine boundaries when necessary. The volume was measured from the most posterior slice of the hippocampal tail to the most anterior limit of the hippocampal head, and the hippocampus was segmented into three subregions (head, body, and tail) along the anteroposterior axis (Fig. 1A). For hippocampal tracing, we followed methods and landmarks described in a previous study.5 All measurements were performed by a single rater (WCH), and the intrarater reliability was examined at 1-week intervals. The intrarater reliability and intraclass correlation coefficients for hippocampal subregion segmentation were 0.98 and 0.99 for the right/left head, 0.99 and 0.98 for the right/left body, and 0.90 and 0.96 for the right/left hippocampal tail volume, respectively.
 Fig. 1:
Fig. 1: Hippocampal segmentation. A, Manual hippocampus tracing. The hippocampus was segmented along the anteroposterior axis in the three subregions: head, body, and tail. B, Automated hippocampal segmentation (3D view). The hippocampus was segmented into 12 subfields: parasubiculum, presubiculum, subiculum, CA1, CA3, CA4, GC-ML-DG, molecular layer, HATA, fimbria, tail, and fissure. CA = cornu ammonis; GC-ML-DG = granule cell (GC) and molecular layer (ML) of the dentate gyrus (DG); HATA = hippocampus—amygdala-transition area.
2.4. Measurement of subfield volumes along the hippocampal transverse axisAn automatic procedure implemented in the FreeSurfer 7.0 software package (Massachusetts General Hospital, Boston, MA; https://surfer.nmr.mgh.harvard.edu/fswiki/ReleaseNotes) was used to measure the volume of the hippocampal subfield in T1 imaging. With the automated method, both the hippocampi of each patient were segmented into 12 subfields: parasubiculum, presubiculum, subiculum, CA1, CA3, CA4, granule cell (GC), and ML of the DG (GC-ML-DG), ML, hippocampus–amygdala transition area (HATA), fimbria, tail, and fissure (Fig. 1B). In this automated segmentation tool, a single computational atlas of the hippocampal formation is constructed using a Bayesian algorithm with labels from in vivo and ex vivo data. The resulting atlas then can be used to automatically segment the hippocampal subfields in structural MRI images. The technical details for automated segmentation and volume quantification for the eight hippocampal subfields were described in a previous study.23
2.5. Statistical analysesStatistical analyses were performed using SPSS (version 21; SPSS, Chicago, IL). Categorical variables were compared between groups by using the Chi-square test (Fisher’s exact test if necessary), and continuous variables were compared using the two-tailed independent t test or one-way analysis of variance. A series of multivariate analyses of covariance (MANCOVAs) were performed to determine differences in the mean volumes of the hippocampal subregions or subfields between groups. In the MANCOVA, the hippocampal subregions or subfields were included as dependent variables and the groups were included as independent variables. Other variables, specifically age, years of education received, sex, and estimated total intracranial volume (eTIV), which may differ significantly between groups, were included as covariates. Once the multivariate null hypothesis was rejected, the main group effect on a specific subregion or subfield volume was analyzed by performing univariate analysis of covariance (ANCOVA) after controlling for the effects of the covariates. For all univariate ANCOVA analyses, Benjamini-Hochberg-adjusted (corrected) p < 0.05 was considered statistically significant to account for multiple comparisons (https://tools.carbocation.com/FDR).
3. RESULTS 3.1. Demographic and clinical characteristicsTable 1 lists the clinical and demographic characteristics of the HCs and patients with schizophrenia. The patients with schizophrenia were treated with the following antipsychotic drugs: aripiprazole (N = 10), risperidone (N = 8), ziprasidone (N = 2), paliperidone (N = 3), amisulpride (N = 4), olanzapine (N = 1), and clozapine (N = 3). The HCs had more mean education years received than the SC-NR (post hoc Bonferroni p = 0.015). The SC-NR group had significantly more men, fewer education years, and higher total scores in the PANSS-8 than the SC-R group (Table 1, all p < 0.05).
Table 1 - Demographic and clinical characteristics of patients with schizophrenia and healthy controls Statistical analysis, F, t, or χ2aContinuous data are presented as mean ± SD.
χ2 = Pearson Chi-square value; CPZ = chlorpromazine equivalent dose; df = degree of freedom; eTIV = estimated total intracranial volume; F = female; HCs = healthy controls; M = male; n.a. = not applicable; PANSS-8 = the eight-item version of the Positive and Negative Syndrome Scale; SC = schizophrenia; SC-NR = nonremitted schizophrenia; SC-R = remitted schizophrenia.
aAnalysis of variance or independent t test for continuous data, and χ2 analysis or Fisher’s exact test for categorical data.
bData in the parentheses indicate the corresponding information of SC-NR and SC-R, respectively.
The left/right whole hippocampal volumes were 2.79 ± 0.51/3.01 ± 0.51 cm3 in the patients with schizophrenia and 3.44 ± 0.48/3.59 ± 0.54 cm3 in the HCs. Compared with the HCs, the patients with schizophrenia had a significantly smaller hippocampus bilaterally after age, sex, education years, and eTIV were controlled for and corrected multiple comparisons (left hippocampus: corrected p < 0.001; right hippocampus, corrected p < 0.01).
Table 2 lists the volumes of hippocampal subregions and subfields in the patients with schizophrenia and HCs. In the MANCOVA, a significant main group effect was noted on the volume of hippocampal subregions (Pillai’s trace = 0.453, F = 7.51, p < 0.001) and subfields (Pillai’s trace = 0.601, F = 2.32, p = 0.01) between the HCs and patients with schizophrenia. The bilateral head and tail subregions were significantly smaller in the patients with schizophrenia than in the HCs, as determined through follow-up ANCOVA (Fig. 2A, Table 2, all corrected p < 0.05). Regarding the hippocampal subfields, follow-up ANCOVAs indicated that the volumes of the left (L.) subiculum, CA1, CA3, CA4, GC-ML-DG, ML, HATA, and tail and right (R.) parasubiculum, CA1, CA3, CA4, GC-ML-DG, ML, and tail of the patients with schizophrenia were significantly smaller than those of the HCs (Fig. 2B, Table 2, all corrected p < 0.05).
Table 2 - Hippocampal subdivision volumes of patients with schizophrenia and healthy controls Orientation Side Subregion/subfield SC, N = 31 HCs, N = 31 p a Corrected p b Longitudinal, mm3 Left Head 1345.8 ± 321.5 1606.8 ± 339.3 0.003 0.006 Body 972.3 ± 284.5 1080.7 ± 290.0 0.143 Tail 467.6 ± 160.0 753.6 ± 215.1 2.0e−07 1.2e-06 Right Head 1481.6 ± 328.3 1849.0 ± 411.0 0.0003 0.0009 Body 1020.7 ± 424.0 1105.8 ± 331.3 0.382 Tail 511.6 ± 166.8 638.4 ± 186.2 0.006 0.009 Transverse, mm3 Left Parasubiculum 133.6 ± 13.1 137.1 ± 14.6 0.3233 Presubiculum 298.5 ± 44.1 310.8 ± 41.0 0.2602 Subiculum 430.0 ± 43.7 457.7 ± 48.5 0.0217 0.040 CA1 621.6 ± 67.3 680.4 ± 82.7 0.0032 0.0097 CA3 209.1 ± 29.7 231.1 ± 29.7 0.0050 0.0133 CA4 264.4 ± 27.9 288.1 ± 30.1 0.0021 0.0082 GC-ML-DG 289.9 ± 31.1 317.0 ± 32.9 0.0015 0.0117 Molecular layer 545.2 ± 56.1 594.4 ± 61.1 0.0016 0.0077 HATA 57.8 ± 7.7 63.3 ± 10.1 0.0191 0.0383 Fimbria 85.6 ± 18.9 84.5 ± 15.8 0.7713 Tail 547.1 ± 92.8 618.6 ± 88.5 0.0029 0.0100 Fissure 140.6 ± 21.8 132.9 ± 22.4 0.1754 Right Parasubiculum 53.2 ± 8.4 59.2 ± 11.7 0.0232 0.0398 Presubiculum 281.3 ± 34.1 296.7 ± 34.8 0.0825 Subiculum 438.9 ± 46.2 462.8 ± 52.0 0.0599 CA1 658.1 ± 79.0 727.6 ± 76.7 0.0008 0.0203 CA3 233.6 ± 30.3 251.0 ± 31.7 0.0313 0.0500 CA4 264.5 ± 29.9 283.1 ± 29.2 0.0162 0.0353 GC-ML-DG 306.6 ± 34.0 328.3 ± 33.8 0.0145 0.0348 Molecular layer 572.3 ± 61.1 623.7 ± 60.5 0.0015 0.0091 HATA 59.0 ± 9.6 63.4 ± 9.9 0.0811 Fimbria 83.1 ± 20.4 84.8 ± 15.5 0.7256 Tail 576.4 ± 76.4 644.5 ± 76.6 0.0009 0.0104 Fissure 147.1 ± 27.6 145.6 ± 23.4 0.8078Continuous data in the cells are presented as mean ± SD. Bold values indicate p < 0.05.
ANCOVA = analysis of covariance; CA = cornu ammonis; GC-ML-DG = granule cell (GC) and molecular layer (ML) of the dentate gyrus (DG); HATA = hippocampus–amygdala transition area; HCs = healthy controls; SC = schizophrenia.
ap Value of follow-up post hoc ANCOVAs.
bCorrected p value after correction for multiple comparisons with the Benjamini-Hochberg approach.
 Fig. 2:
Fig. 2: Hippocampal subdivisional volumes that were significantly different in patients with schizophrenia and healthy controls. A, Hippocampal subregions. B, Hippocampal subfields. (# corrected p = 0.05; * corrected p < 0.05; ** corrected p < 0.01; *** corrected p < 0.001). HCs = healthy controls; L. = left; R. = right; SC = schizophrenia.
3.3. Volume differences in hippocampal subregions and subfields between the SC-NR, SC-R, and HCsAfter the education years were controlled for, a significant main group effect was observed on the volume of the subregions (Table 3, Pillai’s trace = 0.553, F = 3.444, p < 0.001) and subfields (Pillai’s trace = 1.154, F = 2.046, p = 0.003) between the SC-NR, SC-R, and HCs.
Table 3 - Comparisons for the hippocampal subdivision volumes between patients with nonremitted and remitted schizophrenia and healthy controls Orientation Side Subregion/subfield SC-NR, N = 14 (a) SC-R, N = 17 (b) HCs, N = 31 (c) p a Corrected p b Longitudinal, mm3 Left Head 1305.0 ± 322.0 1379.4 ± 326.9 1606.8 ± 331.3 0.025, a < c, b < c 0.037 Body 875.7 ± 279.6 1057.8 ± 270.9 1080.7 ± 290.0 0.096 Tail 467.7 ± 186.2 468.2 ± 140.7 753.6 ± 215.0 2.6e-6, a < c, b < c 1.8e−5 Right Head 1403.6 ± 230.4 1545.9 ± 386.2 1849.0 ± 411.3 0.002, a < c, b < c 0.006 Body 1120.7 ± 561.3 928.2 ± 255.1 1105.9 ± 331.3 0.270 Tail 498 ± 176.9 522.3 ± 162.7 638.4 ± 186.2 0.017, a < c, b < c 0.034 Transverse, mm3 Left Parasubiculum 138.3 ± 11.9 129.7 ± 13.0 137.1 ± 14.6 0.2473 Presubiculum 313.9 ± 53.6 285.8 ± 30.5 310.8 ± 41.0 0.2006 Subiculum 436.1 ± 41.4 428.0 ± 46.2 457.7 ± 48.5 0.0688 CA1 622.9 ± 62.5 620.5 ± 72.9 680.4 ± 82.7 0.0250 CA3 213.0 ± 26.5 205.8 ± 32.5 231.1 ± 29.7 0.0190 CA4 267.3 ± 27.8 262.0 ± 28.5 288.1 ± 30.1 0.0222 GC-ML-DG 293.6 ± 31.6 286.9 ± 31.2 317.0 ± 32.9 0.0152 Molecular layer 550.0 ± 54.2 541.1 ± 58.9 594.4 ± 61.1 0.0138 HATA 57.4 ± 8.1 58.1 ± 7.6 63.3 ± 10.1 0.1234 Fimbria 86.5 ± 14.9 85.2 ± 22.1 84.5 ± 15.8 0.9868 Hippocampal_tail 501.3 ± 89.5 584.8 ± 79.4 618.6 ± 88.5 0.0010, a < b, a < c 0.012 Hippocampal-fissure 145.5 ± 20.1 136.7 ± 23.1 132.9 ± 22.3 0.3853 Right Parasubiculum 54.3 ± 7.7 52.2 ± 8.9 59.2 ± 11.7 0.0729 Presubiculum 284.9 ± 42.3 278.3 ± 26.6 296.7 ± 34.8 0.3275 Subiculum 448.7 ± 46.8 430.8 ± 45.5 462.8 ± 52.0 0.1870
Comments (0)