
Remember me



Atrial septal defect (ASD) is a prevalent congenital heart disease (CHD) with an estimated birth prevalence of 1.43 per 1000 live births. The expected survival rate into adulthood for individuals with ASD is high, at 97%. Typically, patients with ASD remain asymptomatic during the early stages of life; however, the majority of cases with mild or no apparent symptoms go undetected until later in life.1–3
Moderate to large defects can lead to complications such as heart failure, arrhythmias, thromboembolism, or pulmonary hypertension, which can increase the risk of morbidity and mortality, so close monitoring of patients with ASD is crucial to detect and manage these potential complications in a timely manner.4,5
The treatment of ASD depends on the size, location, and symptoms associated with the defect. Small ASDs may not require treatment and may close on their own over time, while moderate to large defects may require intervention, particularly if there are symptoms such as shortness of breath, fatigue, or exercise intolerance. Surgical repair and transcatheter closure are the two main treatment options for ASD.5,6
With timely diagnosis and appropriate management, the prognosis for patients with ASD is generally favorable, with most individuals achieving normal life expectancy and quality of life; nevertheless, most existing studies measure outcomes based on morbidity rates such as atrial arrhythmias and heart failure rather than functionally assessing physical capacity after the procedure.7,8
Cardiopulmonary exercise testing (CPET) is widely recognized as the gold standard for evaluating exercise capacity in a clinical setting. This noninvasive method provides dynamic, objective measurements that can be used for diagnostic, prognostic, and evaluative purposes.9–11
Despite patients with ASD subjectively reporting acceptable exercise tolerance, objective measures reveal a decrease in exercise capacity. In adult patients with ASD, the reduced exercise capacity has been shown to negatively impact multiple domains of perceived health status,12–14 although few studies have evaluated cardiopulmonary function in children with ASD, with a conspicuous lack of emphasis on the preadolescent population. This age group is particularly important as children in this range often engage in physical education classes and daily physical activities.
This study represents the largest sample population in the current research, encompassing a total of 122 children with ASD, to evaluate cardiopulmonary functional capacity through the implementation of CPET, and to investigate whether variations in treatment may impact their cardiopulmonary function, focusing on Taiwanese ASD children. The findings of this study hold potential implications for early intervention of cardiopulmonary rehabilitation.
2. METHODS 2.1. Patient selection and data collectionThis study is a retrospective cohort study that examined data obtained from a single medical center in Taiwan over a period spanning January 2016 to December 2022. Children between 4 and 18 years of age who were referred to the pediatric cardiology outpatient clinic for ASD follow-up were recruited. The study included participants who had undergone treatment for ASD with either surgically repaired ASDs, transcatheter closure ASDs, or unrepaired ASDs previously determined to be hemodynamically insignificant by echocardiography or cardiac catheterization. Exclusion criteria encompassed individuals with other CHDs (eg, ventricular septal defect, patent ductus arteriosus), a current or historical presence of significant arrhythmia, moderate to severe valvular heart disease, or pulmonary disease.
The control participants in this study were carefully matched to the study group at a 1:2 ratio by propensity scores with covariates including age, gender, and body mass index (BMI). They were referred to the pediatric cardiology outpatient clinic due to chest pain or dyspnea on exertion. Comprehensive examinations including physical assessments conducted by pediatricians, symptom-limited CPET, echocardiography, and 12-lead electrocardiography were performed to rule out any specific diseases. This research adhered to the ethical principles outlined in the Helsinki Declaration and was approved by the Institutional Review Board of Kaohsiung Veterans General Hospital (approval number: VGHKS17-CT11-11).
2.2. Cardiopulmonary exercise testingSymptom-limited exercise testing was used in this study to assess the participants’ exercise capacity. The testing apparatus consisted of a treadmill, a flow module, a gas analyzer, and an electrocardiographic monitor (Metamax 3B; Cortex Biophysik GmbH Co., Leipzig, Germany). An experienced physiatrist with over 15 years of expertise in CPET (K.-L.L.) supervised the entire procedure. Before the treadmill exercise test, each participant underwent a familiarization session to acquaint themselves with the testing procedures and equipment. The purpose and nature of the testing were explained to the participants and their families, and informed consent was obtained (verbal consent from participants and written consent from family members). All participants followed the Bruce ramp protocol, recommended by the American College of Sports Medicine (ACSM), during the exercise testing. The test was concluded when participants reported unbearable subjective symptoms, could no longer continue, or reached the ACSM-defined maximal effort criterion.15 During the testing, oxygen consumption (VO2) and carbon dioxide production (VCO2) were measured using the breath-by-breath method. Simultaneously, minute ventilation (VE), blood pressure, and heart rate were also recorded. Furthermore, we assessed the VO2 at the anaerobic threshold (AT) representing aerobic capacity with AT determined by VE/VO2 and VE/VCO2 methods.16 Peak VO2 was defined as the highest level of oxygen uptake achieved during maximal exercise. Peak exercise was determined based on the fulfillment of at least two out of the following three conditions: (1) respiratory gas exchange ratio (RER) >1.1, calculated as VCO2/VO2; (2) heart rate >85% of the age-predicted maximum; or (3) participant’s refusal to continue the test due to exhaustion, despite receiving strong verbal encouragement.17,18
2.3. Pulmonary function testAll participants underwent spirometry-based pulmonary function tests while at rest. Measurements of forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), and maximal voluntary ventilation (MVV) were obtained. The predicted values for each spirometric measure were determined using reference equations specific to healthy children in Taiwan.19
2.4. Statistical analysesContinuous data were expressed as mean ± SD, and categorical variables were presented as absolute numbers or percentages, while the Kolmogorov-Smirnov test was used to determine if continuous variables followed normal distribution. Baseline characteristics and cardiopulmonary exercise parameters between the study and control populations were compared by independent t test and one-way analysis of variance (ANOVA) with post hoc Scheffe’s test for continuous variables if they conformed to normal distribution; Kruskal-Wallis test with post hoc Dunn test was performed if continuous variables did not conform to normal distribution; and Chi-square test was used to compare the categorical variables. A pre-specified two-sided α of 0.05 and 95% CIs were used to determine statistical significance. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
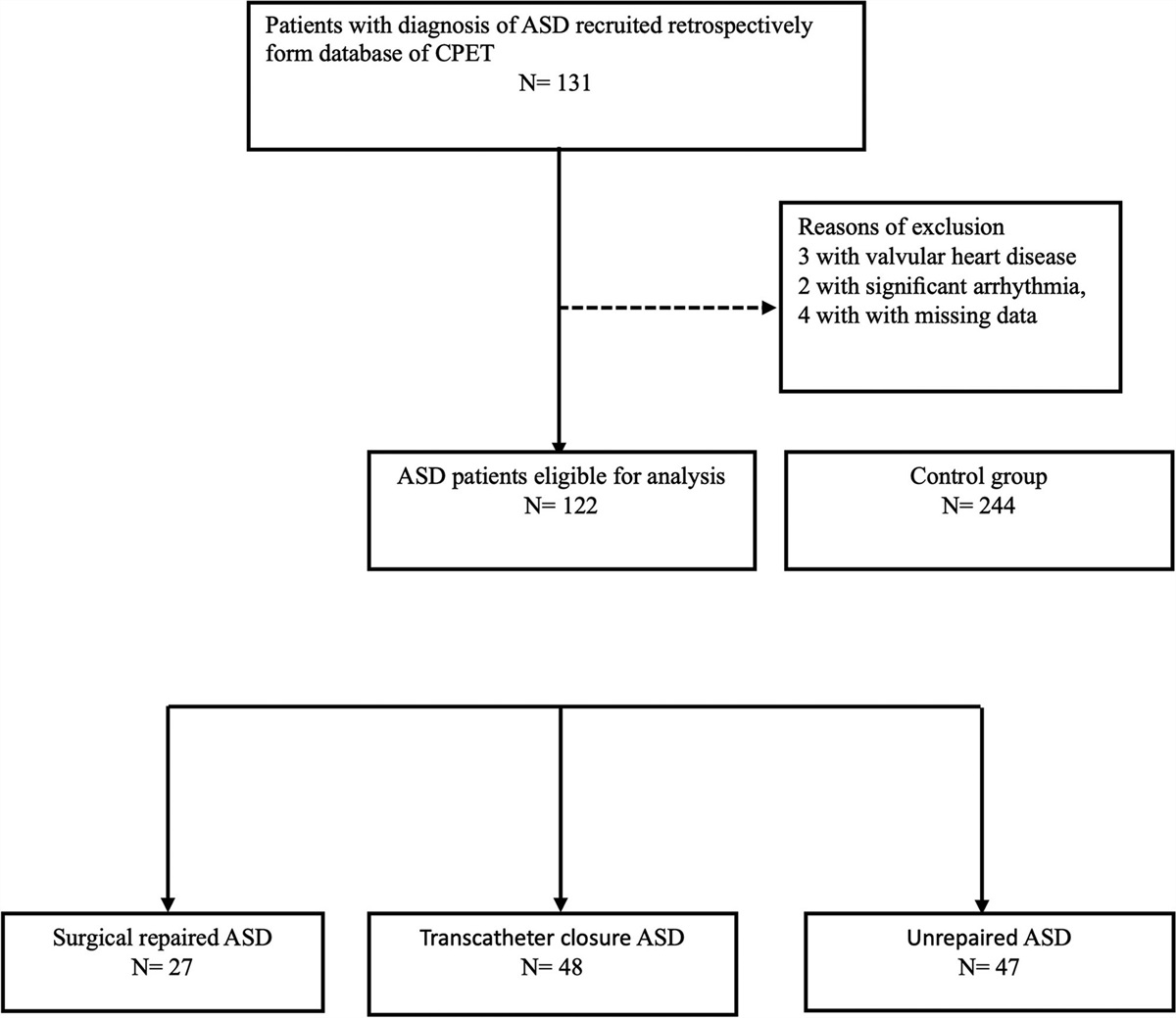
3. RESULTSIn total, 131 patients met the inclusion criteria. Among them, three patients had valvular heart disease, two patients presented with significant arrhythmia, and four patients with missing data were excluded, so the final analysis recruited 122 participants with ASD; additionally, 244 age-, sex-, and BMI-matched healthy participants were recruited as the control group (Fig. 1).
 Fig. 1:
Fig. 1: Flowchart illustrating the inclusion process of patient selection.
Table 1 shows the demographic characteristics of the control and ASD groups. The average age of all ASD children was 11.66 ± 3.58 years, with 42.6% being boys. There were no significant differences in gender, age, body weight, height, BMI, resting blood pressure, and resting heart rate between the two groups.
Table 1 - Demographic characteristics of the ASD and control groups ASD (n = 122) Normal (n = 244) p Age, mean (±SD), y 11.66 (±3.58) 11.58 (±3.53) 0.843 Age, category 4-9 39 (32.0%) 78 (32.0%) 0.965 10-13 41 (33.6%) 79 (32.4%) 14+ 42 (34.4%) 87 (35.7%) Sex, n (%) Male 52 (42.6%) 102 (41.8%) 0.881 Female 70 (57.4%) 142 (58.2%) Height, mean (±SD), cm 145.30 (±17.95) 147.30 (±18.96) 0.342 Body weight, mean (±SD), kg 42.43 (±17.78) 42.46 (±15.89) 0.984 BMI, mean (±SD), kg/m2 19.19 (±4.49) 18.97 (±4.48) 0.657 Resting SBP (±SD), mmHg 109.40 (±15.15) 108.60 (±15.62) 0.653 Resting DBP (±SD), mmHg 63.48 (±9.29) 65.16 (±9.22) 0.103 Resting HR (±SD), bpm 88.16 (±13.69) 87.74 (±14.18) 0.784BMI= body mass index; DBP= diastolic blood pressure; HR= heart rate; SBP= systolic blood pressure.
When comparing the pulmonary function test results between the ASD group and the control group, no statistically significant differences were observed (Table 2) with none of the participants in either group meeting the clinical criteria for restrictive or obstructive lung disease. In terms of exercise test performance, the findings revealed significantly lower values in MET and VO2 (both p = 0.012) at the anaerobic threshold (AT) in the ASD group compared to the control group. Additionally, the ASD group exhibited lower peak MET, peak VO2 (p < 0.001), and peak VE (p = 0.028) compared to the control group (Table 2).
Table 2 - Performance of pulmonary function test and exercise tests of control and ASD groups ASD (n = 122) Normal (n = 244) p Performance of pulmonary function test FVC (±SD), L 2.38 (±0.99) 2.48 (±1.04) 0.351 FVCP (±SD), % 98.18 (±23.99) 99.74 (±21.22) 0.549 FEV1 (±SD), L 2.17 (±1.13) 2.46 (±2.69) 0.146 FEV1P (±SD), % 100.40 (±28.07) 100.50 (±24.40) 0.982 FEV1/FVC (±SD), % 88.49 (±10.33) 88.77 (±8.74) 0.794 MVV (±SD) L/min 52.31 (±24.03) 57.51 (±25.52) 0.061 MVVP (±SD) 110.10 (±52.79) 104.40 (±52.80) 0.340 Performance of exercise test AT MET (±SD) 6.48 (±1.68) 6.94 (±1.46) 0.012 a AT VO2, mL/kg/min 22.70 (±5.90) 24.29 (±5.10) 0.012 a AT HR (±SD), bpm 142.10 (±13.83) 143.80 (±12.39) 0.258 Peak MET (±SD) 9.31 (±2.25) 10.70 (±9.09) <0.001 a Peak VO2, mL/kg/min 32.57 (±7.86) 37.45 (±31.82) <0.001 a Peak HR (±SD), bpm 177.70 (±15.08) 178.90 (±10.50) 0.941 Peak VE (±SD), L/min 39.73 (±16.64) 42.40 (±14.98) 0.028 a Peak RER (±SD) 1.19 (±0.10) 1.20 (±0.09) 0.493 Peak SBP (±SD), mmHg 157.80 (±31.78) 161.50 (±31.95) 0.249 Peak DBP (±SD), mmHg 86.01 (±22.86) 82.27 (±18.37) 0.319Bold values indicates P value <0.005.
AT = anaerobic threshold; DBP = diastolic blood pressure; FEV1 = forced expiratory volume in 1 s; FEV1P = percentage of predicted forced expiratory volume in 1 s; FVC = forced vital capacity; FVCP = percentage of predicted forced vital capacity; HR = heart rate; MET = metabolic equivalent; MVV = maximal voluntary ventilation; MVVP = percentage of maximal voluntary ventilation; RER = respiratory exchange ratio; SBP = systolic blood pressure; VE = minute ventilation.
ap < 0.05.
We conducted a subgroup analysis to evaluate the performance of both pulmonary function tests and exercise tests in children with surgically closed ASD, transcatheter-closed ASD, and unrepaired ASD (Table 3). There were 27 patients with surgically closed ASDs, 48 patients with transcatheter-closed ASDs, and 47 patients with follow-up unrepaired ASD. No significant differences were observed in the performance of cardiopulmonary exercise tests among all these groups nor were significant differences found in subgroup analysis of the pulmonary function test.
Table 3 - Performance of pulmonary function test of surgically closed ASDs, transcatheter-closed ASDs and unrepaired ASDs Surgically closed (n = 27) Transcatheter closed (n = 48) Unrepaired (n = 47) p Performance of pulmonary function test FVC (±SD), L 2.59 (±1.17) 2.24 (±0.89) 2.40 (±0.97) 0.336 FVCP (±SD), % 101.90 (±27.37) 97.96 (±24.90) 96.15 (±20.98) 0.643 FEV1 (±SD), L 2.25 (±0.97) 2.02 (±0.83) 2.28 (±1.45) 0.487 FEV1P (±SD), % 101.70 (±29.40) 102.10 (±31.36) 97.92 (±23.78) 0.770 FEV1/FVC (±SD), % 87.65 (±11.42) 90.07 (±7.80) 87.34 (±11.84) 0.393 MVV (±SD), L/min 52.18 (±20.06) 48.35 (±21.56) 56.42 (±27.97) 0.263 MVVP (±SD) 109.10 (±47.75) 106.80 (±52.62) 113.90 (±56.34) 0.806 Performance of exercise test AT MET (±SD) 6.11 (±1.65) 6.59 (±1.71) 6.59 (±1.68) 0.441 AT VO2, mL/kg/min 21.39 (±5.79) 23.06 (±6.00) 23.07 (±5.87) 0.441 AT HR (±SD), bpm 137.90 (±13.44) 143.90 (±15.70) 142.70 (±11.62) 0.135 Peak MET (±SD) 8.57 (±1.55) 9.35 (±2.47) 9.68 (±2.28) 0.126 Peak VO2, mL/kg/min 30.01 (±5.42) 32.73 (±8.66) 33.88 (±7.98) 0.126 Peak HR (±SD), bpm 173.70 (±13.74) 176.60 (±18.65) 181.20 (±10.61) 0.053 Peak VE (±SD), L/min 41.48 (±16.83) 38.89 (±16.17) 39.57 (±17.28) 0.668 Peak RER (±SD) 1.17 (±0.07) 1.20 (±0.10) 1.21 (±0.11) 0.435 Peak SBP (±SD), mmHg 160.50 (±26.48) 157.00 (±29.92) 157.10 (±36.60) 0.615 Peak DBP (±SD), mmHg 84.70 (±25.10) 87.15 (±23.51) 85.60 (±21.25) 0.824AT = anaerobic threshold; DBP = diastolic blood pressure; FEV1 = forced expiratory volume in 1 s; FEV1P = percentage of predicted forced expiratory volume in 1 s; FVC = forced vital capacity; FVCP = percentage of predicted forced vital capacity; HR = heart rate; MET = metabolic equivalent; MVV = maximal voluntary ventilation; MVVP = percentage of maximal voluntary ventilation; RER = respiratory exchange ratio; SBP = systolic blood pressure; VE = minute ventilation.
This retrospective study conducted at a single-center aimed to investigate the exercise capacity as cardiopulmonary function of children with ASDs using a graded treadmill exercise test. Our observations revealed lower peak minute ventilation, exercise capacity, and aerobic capacity among Taiwanese children with ASDs. Notably, our study focused specifically on Asian children, particularly a significant proportion of them being below 12 years of age, distinguishing it from previous investigations that primarily involved Western adult Caucasians. The present study included a larger sample population, providing robust evidence to support the observation that children with ASD exhibit significantly impaired exercise capacity compared to control subjects. Remarkably, this impaired exercise capacity was consistently observed across ASD patients who underwent surgical closure, transcatheter closure, or remained unrepaired, with no statistically significant differences observed among these subgroups.
Emerging evidence indicates that individuals with congenital ASDs may encounter cardiac and/or pulmonary abnormalities later in life. These findings highlight the importance of regular follow-up by CHD specialists from childhood to adulthood for children with ASDs. Such comprehensive and continued monitoring is crucial in mitigating the severity of complications and improving long-term prognosis in this patient population.20,21
Peak VO2, a critical parameter for assessing exercise capacity, serves as a valuable prognostic indicator in individuals with CHD. It aids in predicting unfavorable outcomes, including hospitalization and all-cause mortality, when an RER above 1.0 is attained. CHD patients with a peak VO2 level below 15.5 mL/kg/min exhibit an increased risk of hospitalization or death (hazard ratio: 2.9; p < 0.0001) and mortality alone (hazard ratio: 5.6; p = 0.02) compared to those with higher peak VO2 values (>15.5 mL/kg/min).22,23
Several studies have reported that individuals with both surgically repaired and transcatheter-closed ASDs exhibit compromised exercise capacity compared to appropriately matched control subjects. Importantly, this impairment in exercise capacity does not seem to improve with advancing age but rather continues to decline over time.12,24 In our study, significantly diminished exercise capacity as indicated by lower peak VO2 assessed by graded symptom-limited exercise testing was found in ASD children, either in surgically closed, transcatheter closure, or unrepaired status. In previous studies, ASD patients have impaired exercise capacity and declined peak VO2 that is often at 50% to 60% of predicted values in healthy controls12,25–27; even in asymptomatic patients having minor reduction in peak oxygen consumption.28 Besides, other CPET parameters including VE/VCO2 slope, MET or VO2 at AT, RER, pulse oximetry, VE/VO2, and VE/CO2 are considered abnormal among ASD patients.12,24,29
Moreover, Pfammatter et al27 found that there were no significant differences between normal children and ASD patients with regard to pulmonary function parameters; additionally, in ASD patients, no significant difference was found in pulmonary function obtained preoperatively compared with the reevaluation after closing of the shunt, which is comparable to our findings. In our study, a larger group of patients with surgically repaired, transcatheter closure and small open defects were included and analyzed, which is different from the earlier experiences within this field.
We observed a noteworthy decrease in VO2 at the AT in children with ASDs. An important consideration during exercise testing is the tendency of patients with CHD to resist pushing themselves to their limits. However, the AT serves as a reliable indicator of the actual disparity in oxygen uptake between ASD patients and control subjects, as it is independent of maximal effort.30 This finding underscores the exercise intolerance and premature attainment of the VO2 level at which cardiovascular insufficiency arises in ASD children, hindering their ability to meet tissue oxygen requirements.
The pathophysiology behind the lower oxygen uptake in ASD patients remains unclear, which might be based on both cardiac and pulmonary factors. However, cardiac factors could play a dominant role according to our results. One study comparing open ASD patients with healthy controls disclosed that the right ventricular (RV) workload is higher at peak exercise due to an additional increase in mean pulmonary arterial pressure (mPAP).31 Also, increasing RV strain and strain rate were found in another controlled study.32 Besides, after ASD closure, increase in LV torsion and decline in global RV longitudinal (GRVL) being a sensitive and stable indicator of RV function were considered evidence of RV overload in ASD patients.33
In subgroup analysis, our findings suggested that lung function and CPET test results are comparable among children with surgically closed ASD, transcatheter-closed ASD, and unrepaired ASD. Both surgical and percutaneous closure methods are effective interventions for ASD with similar mortality rates, and almost 85% to 90% of all secundum ASD can be closed by using a transcatheter approach,34–36 although less evidence has directly compared catheter and surgical ASD closure in terms of CPET parameter. An observational study revealed a higher decreased VE/VCO2 slope in ASD patients after catheter closure than surgical closure at 1-year follow-up, while echocardiographic parameters did not differ significantly.37 We consider advanced and matured techniques of catheterization as one of the reasons of similar results in CPET tests among surgically closed and transcatheter-closed groups, while comparable results noted among repaired and unrepaired groups might be due to advanced intervention techniques and milder symptoms in unrepaired ASD patients. Additionally, a study has demonstrated that following ASD closure, increase in LV torsion and decline in GRVL being a sensitive and stable indicator of RV function were considered evidence of RV overload in ASD patients.33 Such observations provide a plausible explanation for the diminished exercise capacity and compromised cardiopulmonary performance observed after ASD repair. Further studies should be conducted to examine the CPET performance in ASD children with different interventions to differentiate the etiology.
Patients with ASD who considered themselves asymptomatic had 11% less maximal oxygen consumption than their predicted value.28,38 All ages in patients with CHD were encouraged to apply regular exercise intervention, which improved peak VO and work rate significantly.28,38 The results of our study have important implications for children with ASD, particularly those within the age group involved in physical education classes and daily physical activities. The observed significantly impaired exercise capacity in ASD children, regardless of their treatment status (surgical closure, transcatheter closure, or remaining unrepaired), highlights the critical need for early detection and cardiopulmonary interventions. These findings emphasize the importance of implementing timely rehabilitation to improve exercise capacity and overall cardiopulmonary function in children with ASD.
The current study possesses certain limitations. First, it is essential to recognize that this study is based on a single-center retrospective design, and although our study encompassed the largest sample size in this particular domain, the use of a single-center population might restrict the external validity required to support widespread changes in clinical practice. Second, the lack of data pertaining to patients’ exercise participation and self-rated fitness impeded the ability to analyze correlations between lower exercise capacity and levels of physical activity or self-estimated physical function; consequently, the possibility cannot be excluded that lower exercise capacity in the ASD groups could be attributed to reduced levels of physical activity or self-perceived physical deconditioning. Third, the absence of collected echocardiographic data including parameters such as Qp/Qs and pulmonary artery pressure limits our ability to assess how structural factors might have influenced exercise capacity; as a result, the precise pathophysiology underlying these findings remains to be elucidated through the accumulation of additional evidence. Future studies focusing on children with ASD should consider recording echocardiographic and electrocardiographic parameters as well as using more robust measurements such as Swan-Ganz catheterization.
In conclusion, this study revealed that Taiwanese children with ASD had significantly lower exercise capacity as well as cardiopulmonary performance than healthy children of the same age, although no significant differences were observed in the performance of cardiopulmonary exercise tests and the pulmonary function test among the surgically closed ASD group, transcatheter-closed ASD group, and unrepaired ASD group. These findings emphasize the importance of implementing timely rehabilitation to improve exercise capacity and overall cardiopulmonary function in children with ASD.
ACKNOWLEDGMENTSWe are grateful to all participants in this study. We sincerely acknowledge The Department of Pediatrics of the Kaohsiung Veterans General Hospital (KSVGH) for their kind patient referral.
REFERENCES 1. Dave KS, Pakrashi BC, Wooler GH, Ionescu MI. Atrial septal defect in adults. Clinical and hemodynamic results of surgery. Am J Cardiol. 1973;31:7–13. 2. Feldt RH, Avasthey P, Yoshimasu F, Kurland LT, Titus JL. Incidence of congenital heart disease in children born to residents of Olmsted County, Minnesota, 1950-1969. Mayo Clin Proc. 1971;46:794–9. 3. Reybrouck T, Mertens L. Physical performance and physical activity in grown-up congenital heart disease. Eur J Cardiovasc Prev Rehabil. 2005;12:498–502. 4. Kedia G, Tobis J, Lee MS. Patent foramen ovale: clinical manifestations and treatment. Rev Cardiovasc Med. 2008;9:168–73. 5. Webb G, Gatzoulis MA. Atrial septal defects in the adult: recent progress and overview. Circulation. 2006;114:1645–53. 6. Horvath KA, Burke RP, Collins JJ Jr, Cohn LH. Surgical treatment of adult atrial septal defect: early and long-term results. J Am Coll Cardiol. 1992;20:1156–9. 7. Brida M, Chessa M, Celermajer D, Li W, Geva T, Khairy P, et al. Atrial septal defect in adulthood: a new paradigm for congenital heart disease. Eur Heart J. 2022;43:2660–71. 8. Nielsen AKM, Ellesoe SG, Larsen LA, Hjortdal V, Nyboe C. Comparison of outcome in patients with familial versus spontaneous atrial septal defect. Am J Cardiol. 2022;173:128–31. 9. Shephard RJ, Allen C, Benade AJ, Davies CT, Di Prampero PE, Hedman R, et al. The maximum oxygen intake. An international reference standard of cardiorespiratory fitness. Bull World Health Organ. 1968;38:757–64. 10. American Thoracic S and American College of Chest P. ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2003;167:211–77. 11. Takken T, Bongers BC, van Brussel M, Haapala EA, Hulzebos EHJ. Cardiopulmonary exercise testing in pediatrics. Ann Am Thorac Soc. 2017;14:S123–8. 12. Van De Bruaene A, Buys R, Vanhees L, Delcroix M, Moons P, Budts W. Cardiopulmonary exercise testing and SF-36 in patients with atrial septal defect type secundum. J Cardiopulm Rehabil Prev. 2011;31:308–15. 13. Suchon E, Tracz W, Podolec P, Tomkiewicz-Pajak L. Cardiopulmonary capacity and hemodynamic changes in adults with atrial septal defect. Przegl Lek. 2008;65:177–9. 14. Takaya Y, Taniguchi M, Akagi T, Nobusada S, Kusano K, Ito H, et al. Long-term effects of transcatheter closure of atrial septal defect on cardiac remodeling and exercise capacity in patients older than 40 years with a reduction in cardiopulmonary function. J Interv Cardiol. 2013;26:195–9. 15. Pescatello LS. ACSM’s guidelines for exercise testing and prescription. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2014. 16. Washington RL. Cardiorespiratory testing: anaerobic threshold/respiratory threshold. Pediatr Cardiol. 1999;20:12–5; discussion 16. 17. Figueroa-Colon R, Hunter GR, Mayo MS, Aldridge RA, Goran MI, Weinsier RL. Reliability of treadmill measures and criteria to determine VO2max in prepubertal girls. Med Sci Sports Exerc. 2000;32:865–9. 18. Yu CCW, McManus AM, Au CT, So HK, Chan A, Sung RYT, et al. Appropriate scaling approach for evaluating peak VO2 development in Southern Chinese 8 to 16 years old. PLoS One. 2019;14:e0213674. 19. Chang SM, Tsai HJ, Tzeng JY, Yeh KW, Chen LC, Lai SH, et al. Reference equations for spirometry in healthy Asian children aged 5 to 18 years in Taiwan. World Allergy Organ J. 2019;12:100074. 20. Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS, Colman JM, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;73:e81–e192. 21. Baumgartner H, De Backer J, Babu-Narayan SV, Budts W, Chessa M, Diller GP, et al.; ESC Scientific Document Group. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J. 2021;42:563–645. 22. Diller GP, Dimopoulos K, Okonko D, Li W, Babu-Narayan SV, Broberg CS, et al. Exercise intolerance in adult congenital heart disease: comparative severity, correlates, and prognostic implication. Circulation. 2005;112:828–35. 23. Johnson JT, Yetman AT. Cardiopulmonary exercise testing in adults with congenital heart disease. Prog Pediat Cardiol. 2012;34:47–52. 24. Amedro P, Guillaumont S, Bredy C, Matecki S, Gavotto A. Atrial septal defect and exercise capacity: value of cardio-pulmonary exercise test in assessment and follow-up. J Thorac Dis. 2018;10:S2864–73. 25. Geva T, Martins JD, Wald RM. Atrial septal defects. Lancet. 2014;383:1921–32. 26. Giardini A, Donti A, Formigari R, Specchia S, Prandstraller D, Bronzetti G, et al. Determinants of cardiopulmonary functional improvement after transcatheter atrial septal defect closure in asymptomatic adults. J Am Coll Cardiol. 2004;43:1886–91. 27. Pfammatter JP, Zanolari M, Schibler A. Cardiopulmonary exercise parameters in children with atrial septal defect and increased pulmonary blood flow: short-term effects of defect closure. Acta Paediatr. 2002;91:65–70. 28. Brochu MC, Baril JF, Dore A, Juneau M, De Guise P, Mercier LA. Improvement in exercise capacity in asymptomatic and mildly symptomatic adults after atrial septal defect percutaneous closure. Circulation. 2002;106:1821–6. 29. Kempny A, Dimopoulos K, Uebing A, Moceri P, Swan L, Gatzoulis MA, et al. Reference values for exercise limitations among adults with congenital heart disease. Relation to activities of daily life—single centre experience and review of published data. Eur Heart J. 2012;33:1386–96. 30. Medicine ACoS. ACSM’s guidelines for exercise testing and prescription. Pennsylvania, USA: Lippincott Williams & Wilkins; 2013. 31. Van De Bruaene A, De Meester P, Buys R, Vanhees L, Delcroix M, Voigt JU, et al. Right ventricular load and function during exercise in patients with open and closed atrial septal defect type secundum. Eur J Prev Cardiol. 2013;20:597–604. 32. Baydar O, Oktay V, Sinan UY, Cakal S, Cakal B, Coskun U, et al. Strain analysis during exercise in patients with asymptomatic atrial septal defect. Echocardiogr. 2014;31:1239–44. 33. Kim JY, Yun BS, Lee S, Jung SY, Choi JY, Kim NK. Changes in strain pattern and exercise capacity after transcatheter closure of atrial septal defects. Korean Circ J. 2017;47:245–53. 34. Chambault AL, Olsen K, Brown LJ, Mellor SL, Sorathia N, Thomas AE, et al. Transcatheter versus surgical closure of atrial septal defects: a systematic review and meta-analysis of clinical outcomes. Cardiol Young. 2022
Comments (0)