
Remember me



Even though the incidence of differentiated thyroid cancer (DTC) continues to increase, it is mostly associated with favorable outcomes.1–4 The majority of DTC histological type is papillary thyroid cancer, followed by follicular thyroid carcinoma.1 Surgical resection, possibly with or without radioiodine therapy, is the standard treatment for most DTCs.5 Several systems have been developed to better establish the prognostic factors of importance in patients with DTC. These include the metastasis, age, completeness of resection, invasion, and size system, and the American Joint Committee on Cancer (AJCC) TNM staging system.3,5,6 However, the TNM staging criteria do not incorporate the completeness of resection and are unable to accurately predict the risk of recurrence.5,7 Subsequently, the American Thyroid Association (ATA) developed and revised a risk of recurrence stratification system, which stratifies patients into low, intermittent, and high-risk according to their clinicopathological and molecular features. This is done to better predict recurrence risk in patients with DTC after initial treatment. In this system, incomplete tumor resection is one of the defining features of the high-risk group, with an escalated risk of recurrence or persistent disease compared with low- and intermittent-risk groups.5
To better evaluate postoperative radioactive iodine (RAI) therapy, not just after initial treatment, but continuously during follow-up, the response to therapy reclassification (RTR) system was developed. It is now widely applied to dynamically estimate the risk of disease recurrence after thyroidectomy and postoperative RAI therapy, as stated in the 2015 ATA DTC management guidelines.5 Various studies have validated this risk assessment tool, including Tuttle et al.7 The results of a study by Shen et al. further supported the use of this risk stratification system in Chinese patients with well-DTC.8
Notwithstanding, the compromised outcomes of incomplete resection with gross margin positivity, also known as R2 resection, in patients with DTC is well-recognized.9,10 The disparities in treatment responses and outcomes among patients with gross residual disease are not well-studied. In our study, we aimed to identify the factors associated with positive macroscopic surgical margins and examined the clinical applicability of the RTR system in patients with gross positive margins. The parameters that discriminated the treatment responses and recurrence-free survival (RFS) among these patients were determined.
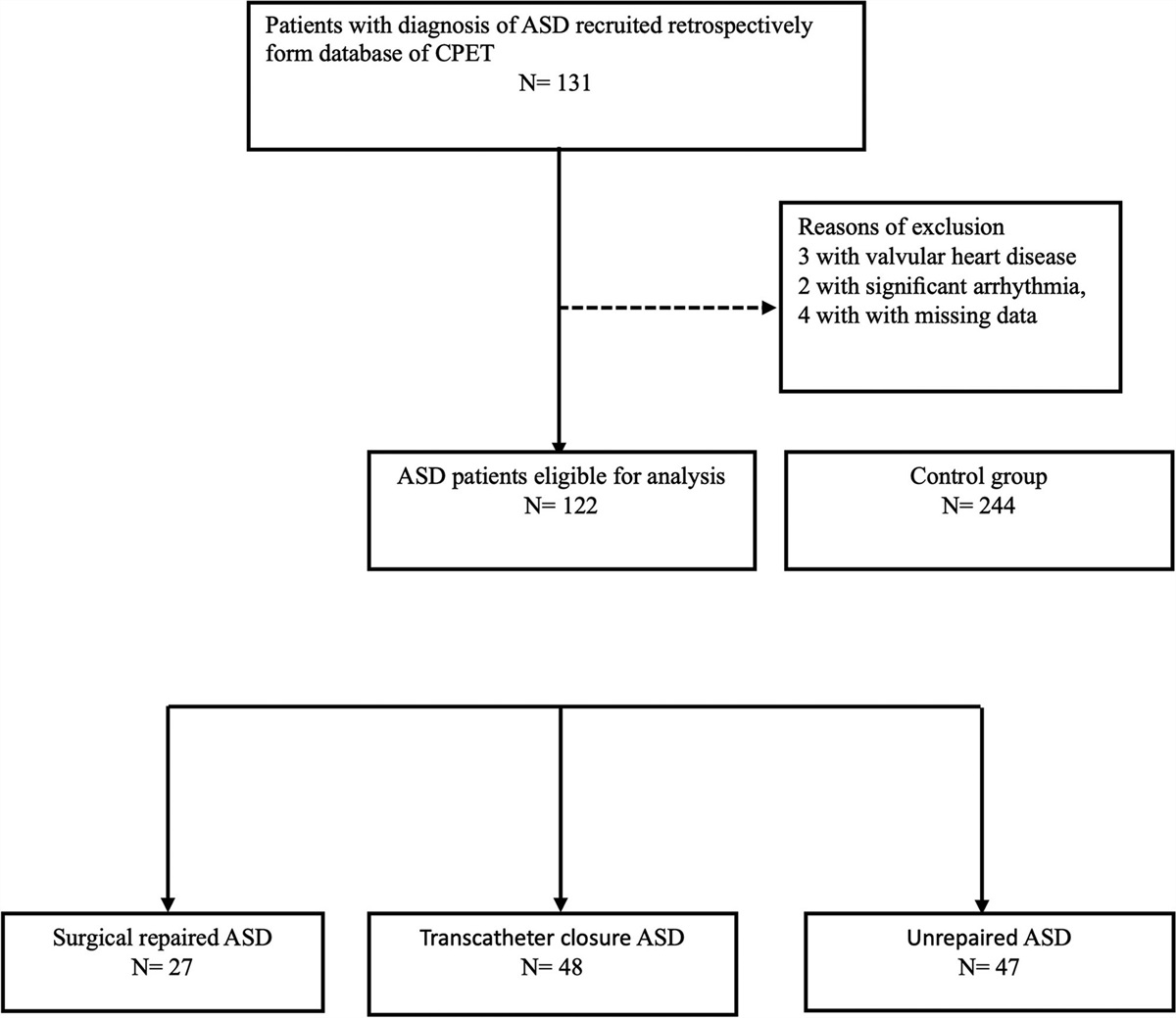
2. METHODSWe reviewed our institutional database of 1,247 patients with thyroid cancer who underwent surgery between January 2013 and July 2018 at the Kaohsiung Chang Gung Memorial Hospital. These patients were followed up until December 2019. A total of 242 DTC patients with tumor extension beyond the thyroid capsule were included. Patients with DTC without extrathyroidal extension, nonDTC, with distant metastasis, with prior treatment at other hospitals, who were lost to follow-up, or had treatment termination due to personal preferences were excluded (Fig. 1). This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital (IRB No.: 201801481B0C501). The included patients were grouped according to their surgical margins into either negative surgical, microscopically positive margins (R0/R1), or gross residual disease (R2) after surgical resection of thyroid cancer. The patients with R2 resection were further classified into two groups according to their treatment response: excellent and nonexcellent. The nonexcellent response group comprised patients with incomplete or indeterminate structural, biochemical, or indeterminate responses.5,7 The responses to treatment were assessed approximately 1 year after initial thyroidectomy and postoperative RAI therapy. An excellent response was defined as no clinical, biochemical, or structural evidence of disease. A biochemical incomplete response included patients with abnormal thyroglobulin (Tg) or increasing antithyroglobulin antibody (TgAb) levels but with negative findings on imaging. A structural incomplete response included patients with structural evidence of disease identified by imaging. Patients with an indeterminate response included those with stable or decreasing TgAb levels without imaging evidence of disease.5
 Fig. 1:
Fig. 1: Flow diagram of the inclusion and exclusion criteria of patients enrolled in this study.
The operation and pathology reports were reviewed to confirm the completeness of surgical resections. The patients were staged or restaged according to the AJCC 8th edition, including those previously staged using the AJCC 7th edition.11 The following data were collected and analyzed: age, sex, extent of extrathyroidal extension (ETE), TNM staging (AJCC 8th), extent of thyroidectomy and neck dissection, cumulative dose of postoperative RAI therapy, postoperative TSH-stimulating thyroglobulin (TSH-Tg) levels measured before ablation, 3- to 6-month post-RAI Tg levels, TgAb levels, and postoperative radiation therapy. The 5-year local recurrence-free survival (LRFS) and distant recurrence-free survival (DRFS) were compared between patient groups. Disease recurrence consisted of local and distant recurrence, and location of metastasis were determined based on evidence of structural abnormality detected by imaging studies or fine-needle aspiration biopsy. Local recurrence included thyroid bed and neck lymph node recurrence.9
The IBM Statistical Package for Social Science (SPSS) Statistics version 25.0 for Windows (IBM Incorporated, Armonk, NY, USA) was utilized for the analysis. Variables between R0/R1 versus R2 patients with an excellent vs. nonexcellent response were compared using Fisher’s exact tests, Pearson’s x2 tests, and the Mann–Whitney U Test. RFP was calculated using the Kaplan–Meier method and compared between patient groups using the log-rank test. p <0.05 was considered statistically significant.
3. RESULTSThe mean follow-up duration was 45.3 months (2.9–81.8 months). The median age of the 242 patients with ETE was 53 years (interquartile range, 44–61 years); 182 patients (75.2%) were female. Among the 242 patients, 207 (85.5%) were found to have either negative surgical or microscopically positive margins (R0/R1), and 35 (14.5%) patients had gross residual disease after surgery (R2). The patients with R2 resection had more advanced cancer (stage III/IV 42.9% vs. 2.4%, p < 0.001), all of whom underwent total thyroidectomy and received a higher cumulative dose of radioactive iodine therapy (median: 150 mCi vs. 100 mCi in R0/R1 group, p < 0.001; Table 1).
Table 1 - The parameters and outcomes of patients with R0/R1 compared to R2 resection Parameter Total R0+R1 resection R2 resection p n (%) 242 207(85.5%) 35(14.5%) Female sex 182(75.2%) 158(76.3%) 24(68.6%) 0.326 Age at diagnosis (years) [median (interquartile range)] 53 (44–61) 53 (43-60) 56 (47–62) 0.112 Tumor histopathology Papillary thyroid carcinoma 240(99.2%) 205(99.0%) 35(100%) 1.000 Follicular carcinoma 2(0.8%) 2(1.0%) 0 Staging (AJCC/TNM 8th) I or II 222(91.7%) 202(97.6%) 20(57.1%) <0.001 III or IV 20(8.3%) 5(2.4%) 15(42.9%) Total thyroidectomy 220(90.9%) 185(89.4%) 35 (100%) 0.051 Radioactive iodine therapy 224(92.6%) 189(91.3%) 35 (100%) 0.084 Cumulative dose (median [interquartile range] [mCi]) 102 (100–140) 100 (100–120) 150 (120–220) <0.001 Treatment response Excellent 172(71.1%) 156(75.4%) 16(45.7%) 0.002 Structural incomplete 15(6.2%) 10(4.8%) 5(14.3%) Biochemical incomplete 49(20.2%) 36(17.4%) 13(37.1%) Indeterminate 6(2.5%) 5(2.4%) 1(2.9%) Recurrencea Yes 24 (9.9%) 13(6.3%) 11(31.4%) <0.001 Local regional recurrence 23(9.5%) 12(5.8%) 11(31.4%) <0.001 Distant recurrence 5(2.1%) 2(1.0%) 3(8.6%) 0.023 No 218(90.1%) 194(93.7%) 24(68.6%)aThe cases of recurrence included local regional recurrence and distant recurrence.
# Some cases had both local regional and distant recurrence.
AJCC=American Joint Committee on Cancer; TNM=tumor, node, metastasis (TNM) staging system
Regarding treatment outcomes, fewer patients with R2 resection margins achieved an excellent response (45.7% vs. 75.4%). A higher proportion of these patients had structurally (14.3% vs. 4.8%) and biochemically incomplete response (37.1% vs. 17.4%) to treatment (p = 0.002). There was a higher local and distant recurrence rate among patients with R2 resection (31.4% vs. 5.8% p < 0.001 and 8.6% vs. 1.0%, p = 0.023, respectively) compared with those with R0 or R1 resection (Table 1).
Among the 35 patients with R2 resection, 15 (42.9%) achieved an excellent response, while 20 (57.1%) achieved a nonexcellent response. There were no differences in age, sex, tumor size, RAI accumulated dose, administration of radiation therapy, or the extent of extrathyroidal extension (ETE) between the excellent and nonexcellent response groups. A statistically significant difference was observed in the extent of neck dissection, TSH-Tg level, post-RAI Tg level, nodal status, and recurrence between the two groups (Table 2). The characteristics of the R2 group recurrent cases were listed in supplementary table 1 https://links.lww.com/JCMA/A248.
Table 2 - Comparing the parameters and outcomes of R2 resection with excellent and nonexcellent response R2 resection Number(N) Excellent response Nonexcellent response p Number 35 15(42.9%) 20(57.1%) Age < 55 15(42.9%) 7(46.7%) 8(40.0%) 0.693 ≥ 55 20(57.1%) 8(53.3%) 12(60.0%) Sex 35 Female 24(68.6%) 11(73.3%) 13(65.0%) 1.000 Male 11(31.4%) 4(26.7%) 7(35.0%) Total thyroidectomy 35 15(42.8%) 20(57.1%) Neck dissection None 3(8.6%) 3(20.0%) 0 <0.001 Central 21(60.0%) 12(80.0%) 9(45.0%) Central + Lateral 11(31.4%) 0 11(55.0%) Cumulative dose of RAI therapy(mCi) <30 0 0 0 0.429 30-99 1(2.9%) 1(6.7%) 0 ≥100 34(97.1%) 14(93.3%) 20(100%) Postoperative stimulated Tg(ng/mL) <1 4(11.4%) 3(20.0%) 1(5.0%) <0.001 1-10 10(28.6%) 8(53.3%) 2(10.0%) >10 21(60.0%) 4(26.7%) 17(85.0%) Post-RAI Tg(ng/mL) <0.2 19(54.3%) 12(80.0%) 7(35.0%) 0.008 ≥ 0.2 16(45.7%) 3(20.0%) 13(65.0%) TgAb No 32(91.4%) 15(100%) 17(85.0%) 0.244 Yes 3(8.6%) 0 3(15.0%) EBRT No 31(88.6%) 14(93.3%) 17(85.0%) 0.619 Yes 4(11.4%) 1(6.7%) 3(15.0%) pT size ≤4cm 29(82.9%) 13(86.7%) 16(80.0%) 0.680 >4cm 6(17.1%) 2(13.3%) 4(20.0%) Extrathyroidal Extension (ETE) T3b 8(22.9%) 6(40.0%) 2(10.0%) 0.051 T4a/t4b 27(77.1%) 9(60.0%) 18(90.0%) pN status N0/NX 15(42.9%) 11(73.3%) 4(20.0%) <0.001 N1a 10(28.6%) 4(26.7%) 6(30.0%) N1b 10(28.6%) 0 10(50.0%) Recurrencea Yes 11(31.4%) 1(6.7%) 10(50.0%) 0.009 Local regional recurrence 11(31.4%) 1(6.7%) 10(50.0%) 0.009 Distant recurrence 3(8.6%) 0 3(15.0%) 0.244 No 24(68.6%) 14(93.3%) 10(50.0%)aThe recurrence cases included local regional recurrence and distant recurrence.
# Some cases had both local regional and distant recurrence.
ERBT=External Beam Radiotherapy
Fig. 2 displays the extrathyroidal structures involved in the patients with R2 resection. The first three most common invaded sites in these patients were the RLNs (62.9%), muscles (42.9%), and trachea (42.9%) (Fig. 2). The invaded muscles included the strap, cricothyroid, and sternocleidomastoid muscles. Sixty percent of the patients with R2 resection with an excellent response had muscle invasion by a tumor. In contrast, the RLN was the most frequently invaded site among the nonexcellent responders. However, there was no significant difference in the distribution of the invasion sites between the excellent and nonexcellent groups in patients with R2 resection (p = 0.297; Fig. 2).
 Fig. 2:
Fig. 2: Distribution of extrathyroidal structures invaded by the tumor in R2 resected patients with excellent versus nonexcellent response. The overall number of patients with R2 resection was 35. The total number and percentages (number of patients with particular invasion site/35 × 100%) were presented at the top of each bar graph. The upper layer of bar graph (blue) represented number of R2 resected patients with excellent response. Lower layer of bar graph (gray) represented number of R2 resected patients with nonexcellent response. The invaded muscles included the strap, cricothyroid, and sternocleidomastoid muscles. No significant difference in the distribution of the invasion sites between the excellent and nonexcellent groups in the patients with R2 resection (p = 0.297).
The Kaplan–Meier curves for LRFS and DRFS of patients in (1) R0/R1 versus R2 groups, and (2) R2 excellent versus R2 nonexcellent response groups, are illustrated in Figs. 3 and 4, respectively. The 5-year LRFS and DRFS rates of R0/R1 versus R2 patients were 90.0% versus 66.3%, and 98.4% versus 90.7%, respectively (p < 0.001; Fig. 3A, B). In those with R2 resection with excellent response, the LRFS was significantly higher than in those patients with R2 resection who failed to achieve an excellent response (93.3% vs. 45.1%, p = 0.008; Fig. 4A). However, there was no significant difference in DRFS between the two R2 groups (100% vs. 83.3%, p = 0.112) (Fig. 4B).
 Fig. 3:
Fig. 3: Cumulative Kaplan–Meier curves of (A) 5-year LRFS; (B) 5-year DRFS for patients treated with resection stage R0 or R1 versus R2. R0 resection (red line) is defined as complete removal of tumor with negative surgical margin. R1 resection (red line) is defined as removal of tumor with remaining microscopically positive margin. R2 resection (blue line) is defined as gross residual disease after tumor resection. Local recurrence included thyroid bed and neck lymph node recurrence, and distant recurrence referred to recurrence other than local recurrence. Significant difference (p<0.001) for both LRFS and DRFS between these two groups were noted. DRFS = distant recurrence-free survival, LRFS = local recurrence-free survival.
 Fig. 4:
Fig. 4: Cumulative Kaplan–Meier curves of (A) 5-year LRFS; (b) 5-year DRFS for R2 resected patients with an excellent response (red line) versus nonexcellent response (blue line). Excellent response is defined as no clinical, biochemical, or structural evidence of disease. The nonexcellent response included patients with incomplete structural, incomplete biochemical, and indeterminate response. Significant difference of LRFS (p = 0.008) but not in DRFS (p = 0.112) were noted between these two groups. DRFS = distant recurrence-free survival, LRFS = local recurrence-free survival.
4. DISCUSSIONIn our study, compared with R0/R1 patients, the patients with R2 resection had more advanced thyroid cancer stages (stage III/IV, 42.9% vs. 2.4%, p < 0.001) and received higher cumulative RAI doses (median: 150 mCi vs. 100 mCi in R0/R1 group, p < 0.001). Few of these R2 patients achieved an excellent response (45.7% vs. 75.4%) and had a higher recurrence rate (local recurrence: 31.4% vs. 5.8%, p <0.001; distance recurrence: 8.6% vs. 1.0%, p=0.023) compared with R0 or R1 patients. Macroscopic margins or gross residual disease after total thyroidectomy for DTC are associated with poorer survival and a higher rate of disease recurrence.9,10 Patients with R2 resection, although not statistically significant, were older compared with patients with R0/R1 resection, with a median age above 55 years old. According to the AJCC grading system 8th edition, stage III and IV consists of patients aged older than 55 years old with gross ETE beyond the thyroid gland, apart from strap muscle invasion.11 In 2015, ATA also differentiated the thyroid cancer management guidelines, and patients with gross ETE and incomplete tumor resection were stratified as high risk for disease recurrence.5 A few studies also demonstrated the impact of operative margin status on disease recurrence. In a study by Radowsky et al, 19 out of 276 treated patients with macroscopically positive margins had significantly higher proportions of disease recurrence compared with patients with negative margins (29% vs. 4%, p = 0.01).12 Na et al13 found that positive operation margins rather than nerve preservation or resection affect tumor recurrence in patients with T4a papillary thyroid cancer and recurrent laryngeal nerve (RLN) involvement.
When the patients with gross residual disease were categorized based on their response to therapy, the nonexcellent responder had significantly higher recurrence rates than the patients with R2 resection with an excellent response (50.0% vs. 6.7%, p = 0.009). The results paralleled the general DTC population, where the patients with nonexcellent response demonstrated more detrimental outcomes.5 Among the patients with R2 resection, the extent of neck dissection was significantly greater in the nonexcellent group (p < 0.001), where more than 50% of cases had total thyroidectomy plus central and lateral lymph node dissection (LND), and none of them underwent solely total thyroidectomy. Indeed, there was a significantly higher number of nonexcellent responders in the R2 group with N1b status, indicating tumor invasion into lateral or/and mediastinal lymph node(s). Study by Lin et al14 found that lymph node metastasis was a bad prognostic factor of thyroid cancer with extrathyroidal extension, although the nodal status of lymph node involvement was not categorized in this study. Currently, no major guidelines recommend prophylactic LND;5,15 hence, thyroid resection with LND is usually therapeutic for lateral lymph node metastasis (LLNM). Ultrasound as a preoperative diagnostic tool has low sensitivity for detecting LLNM,16,17 which may persist after surgery and be later detected as recurrence. The advanced stage tumor with LLNM usually reflects an aggressive and extensive tumor infiltration in these patients. Moreover, total thyroidectomy with lateral LND is technically intricate and accompanied by a higher risk of surgical complications.2,17 These patients were thus more likely to be detected as having structurally or biochemically incomplete responses after 1 year.
The postoperative TSH-Tg level was significantly higher in the nonexcellent group compared with the excellent group among the R2 patients (p < 0.001). The postoperative TSH-Tg level obtained before RAI therapy is useful in predicting the prognosis of patients with DTC, where a higher level is correlated with an increased probability of recurrence or persistent disease.18,19 The high-risk group stratified by the ATA has greater postoperative TSH-Tg levels on average in comparison to the intermediate- and low-risk groups.20 Tg is produced by postsurgical residual follicular cells. Nevertheless, our results showed discrepancies in postoperative TSH-Tg levels among the patients with R2 resection. A higher proportion of these patients with postoperative TSH-Tg levels greater than 10 ng/mL fell into the nonexcellent response category after RAI therapy. Even though the value of postoperative TSH-Tg levels as a prognostic marker decreased with incomplete resection,19 it may still be useful in predicting the possibility of treatment failure or metastatic disease in patients with R2 resection.
Previous studies have shown RLN invasion in approximately 50% of the locally advanced cases.21 We found that, in patients with R2 resection, more than 50% of cases had RLN involvement, and most were nonexcellent responders. RLN infiltration with tumor can be either resected or preserved by shaving. The decision to select RLN sparing versus resection is made by considering the degree of nerve invasion (tumor adheres or encases the nerve), pre and postsurgical ramifications on vocal cord function, and the presence of other inoperable metastatic diseases,22 which in turn may affect the completeness of tumor resection. Although the strap muscle is the most common ETE site for thyroid cancer, it can be resected with less risk for adverse sequelae.21 Therefore, it is reasonable that a smaller proportion of R2 resections occurred in patients with only strap muscle invasion. In our study, muscle tissue was the second most invaded site after RLN, which often co-occurred with the invasion of other adjacent structures around the thyroid. Even so, muscle was the most frequent invasion site among the R2 excellent responder.
In conclusion, this was a single-centered, retrospective study, with a small sample size of patients (total: n = 242; R2 resected patients: n = 35) eligible to be studied and analyzed. The follow-up period was relatively short (average less than 5 years), given that the prognosis of thyroid cancer is generally good with a 5-year survival of greater than 95%.23 Therefore, a longer study duration and larger, multicentered populations of patients are needed to clarify long-term clinical outcomes and treatment responses of patients with R2 resection.
In differentiated thyroid carcinoma with extrathyroidal extension, gross residual disease is one of the important features associated with poorer treatment responses, and it is included in the high-risk category in the ATA system. When further analyzed in patients with R2 resection, the nonexcellent response group also had lower 5-year RFS compared with the excellent response group, where the former had more advanced tumor staging and required LLN dissection more frequently. Higher postoperative thyroglobulin level, higher post-RAI thyroglobulin level at 3- to 6-month follow-up and more advanced nodal status were factors contributing to their nonexcellent response hence a poorer prognosis. The RTR system can be applied to this population, studies on a larger scale and extended duration are required to further optimize the stratification of RFS and mortality among patients with R2 resection.
ACKNOWLEDGMENTSWe appreciated the Biostatistics Center, Kaohsiung Chang Gung Memorial Hospital for statistical data analysis. This study was funded by Chang Gung Memorial Hospital-Kaohsiung Medical Center, Kaohsiung, Taiwan (Contract No. CMRPG8L0321, CMRPG8M0611 and CMRPG8K0961).
APPENDIX A. SUPPLEMENTARY DATASupplementary data related to this article can be found at https://links.lww.com/JCMA/A248.
REFERENCES 1. Kitahara CM, Sosa JA. The changing incidence of thyroid cancer. Nat Rev Endocrinol. 2016;12:646–53. 2. Muller S, Senne M, Kirschniak A, Königsrainer A, Bares R, Falch C. Impact of surgical resection extension on outcome for primary well-differentiated thyroid cancer-a retrospective analysis. World J Surg Oncol. 2017;15:1–5. 3. Choi H, Kasaian K, Melck A, Ong K, Jones SJ, White A, et al. Papillary thyroid carcinoma: prognostic significance of cancer presentation. Am J Surg. 2015;210:298–301. 4. Schlumberger M, Leboulleux S. Current practice in patients with differentiated thyroid cancer. Nat Rev Endocrinol. 2021;17:176–88. 5. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26:1–133. 6. Cipriani NA. Prognostic parameters in differentiated thyroid carcinomas. Surgical Pathology Clinics. 2019;12:883–900. 7. Tuttle RM, Tala H, Shah J, Leboeuf R, Ghossein R, Gonen M, et al. Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation: using response to therapy variables to modify the initial risk estimates predicted by the new American Thyroid Association staging system. Thyroid. 2010;20:1341–9. 8. Shen FC, Hsieh CJ, Huang IC, Chang YH, Wang PW. Dynamic risk estimates of outcome in Chinese patients with well-differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation. Thyroid. 2017;27:531–6. 9. Wang LY, Nixon IJ, Patel SG, Palmer FL, Tuttle RM, Shaha A, et al. Operative management of locally advanced, differentiated thyroid cancer. Surgery. 2016;160:738–46. 10. Youngwirth LM, Adam MA, Scheri RP, Roman SA, Sosa JA. Patients treated at low-volume centers have higher rates of incomplete resection and compromised outcomes: analysis of 31,129 patients with papillary thyroid cancer. Ann Surg Oncol. 2016;23:403–9.
Comments (0)