
Remember me



Taiwan has the highest incidence and prevalence rates of end-stage kidney disease worldwide,1 probably because the Taiwan National Health Insurance system fully reimburses the cost for hemodialysis in almost 100% of their population.2 Additionally, the total number of patients requiring dialysis increased by 28.9% from 2010 to 2018, with most of the patients choosing hemodialysis as their initial dialysis modality (86.8% in 2010 and 90.6% in 2018).3 Previous reports have shown that the primary patency rate of either arteriovenous fistula (AVF) or arteriovenous graft (AVG) was not high and declined progressively, which remains a big challenge to clinicians and patients.2,4 Moreover, the prevalence is still as high as 12% even with early detection by ultrasound dilution technique reducing the per-patient thrombotic events.4 Thus, in addition to monitoring and prevention, early intervention of dysfunctional hemodialysis access is another important issue because the time to intervention is associated with higher technical success and may improve midterm patency.5–7
Traditionally, patients must visit an outpatient clinic (OPD) or emergency room (ER) from a hemodialysis center locally or in a hospital to seek help for obstructed hemodialysis vascular access. Subsequently, an interventionist, an empty catheterization room, and sufficient technicians and paramedical staff must be available to perform the intervention for the patients. Usually, communication at medical centers is time-consuming.8 Hence, departments and even clinics/hospitals must closely collaborate to facilitate quality improvement in percutaneous transluminal angioplasty (PTA) for dysfunctional or failed AVF/AVG. Therefore, we established a rapid intervention team (RIT) comprising case managers, peripheral interventionists, cardiovascular surgeons, and catheterization laboratory technicians across departments, clinics, and hospitals in 2019. Herein, we evaluated the feasibility, performance of quality improvement, and outcome of the implementation of an “RIT strategy.” We hypothesized that the implementation of the “RIT strategy” was feasible, would improve the quality of intervention, and provide better clinical outcomes for AVF/AVG dysfunction or failure.
2. METHODS 2.1. Study population and inclusion criteriaWe retrospectively enrolled consecutive patients aged >20 years who underwent PTA for AVF or AVG over the upper extremities at National Cheng Kung University Hospital, a tertiary referral center in southern Taiwan, from February 1, 2017 to December 31, 2022. We excluded patients who underwent PTA during admission because of the scope and aim of the current study. The patients were categorized into two groups: the RIT and control groups, based on whether they were served and managed by case managers of the RIT before PTA. This study adhered to the principles of the Declaration of Helsinki and was approved by the Human Research and Ethics Committee of the National Cheng Kung University Hospital (Identifier: A-ER-111-601). Informed consent was waived due to the retrospective nature of the study design.
2.2. RIT strategyThe RIT system was introduced in September 2019 at our hospital. Case managers function as the pivot of this RIT system. All the requests of management for occluded AVF/AVG were recommended to the case managers who were on call 24 hours daily. We had previously visited each dialysis clinic around Tainan City to establish a medical league comprising 22 dialysis clinics. The dialysis clinics and the case managers were connected via telephones and communication software. The patients could also connect with case managers personally or through the clinics. The case managers were preferably technicians working in the catheterization room, who could therefore provide real-time information regarding room availability. All interventionists and cardiovascular surgeons at RIT should provide their schedules to case managers to facilitate matching available doctors and reserving space.
When the case manager acknowledged a new case, the fastest available physician and nearby room were rapidly allocated, and the patient was notified of the appointment time and site. Interventions were mostly performed as outpatient procedures to reduce the unnecessary management sequence.
2.3. Time to interventionThe definition of time to intervention is diverse, depending on patient source. For OPD patients, it was defined as the time elapsed from check-in at the counter in our catheterization laboratory to the patient being placed on the catheterization table. For ER patients, it was defined as the time elapsed from ER registration to the patients being placed on the table. For patients referred from dialysis rooms or clinics, it was defined as the time elapse from dysfunctional AVF/AVG recorded to the patient being placed on a table.
2.4. Clinical outcomesElectronic medical records were reviewed to obtain baseline characteristics and clinical outcomes. The primary endpoints were double-lumen insertion and a composite outcome involving permanent catheter insertion, and the need for recreation due to poor AVF/AVG function. The secondary endpoint was all-cause mortality. The rates of double-lumen catheter insertion and permanent catheter insertion or shunt recreation 3 days before and after dialysis access dysfunction were reviewed from electronic medical records. We also documented the cumulative survival of both groups. The enrolled patients were followed up until March 31, 2023.
2.5. Statistical analysisSPSS version 21.0 (IBM, Armonk, NY) was used for statistical analysis. Categorical variables were expressed as numbers or percentages. Continuous data were presented as means ± SDs or median (interquartile range), as appropriate. Comparisons were conducted using the chi-square test with Fisher exact test and either Student’s t test or Wilcoxon rank sum test for categorical and continuous variables, respectively. Continuous variables in multiple periods were compared using one-way analysis of variance. A Kaplan-Meier survival curve using the Cox proportional hazard method was used to compare the cumulative survival of the primary composite endpoint between both groups. Statistical significance was determined at p < 0.05.
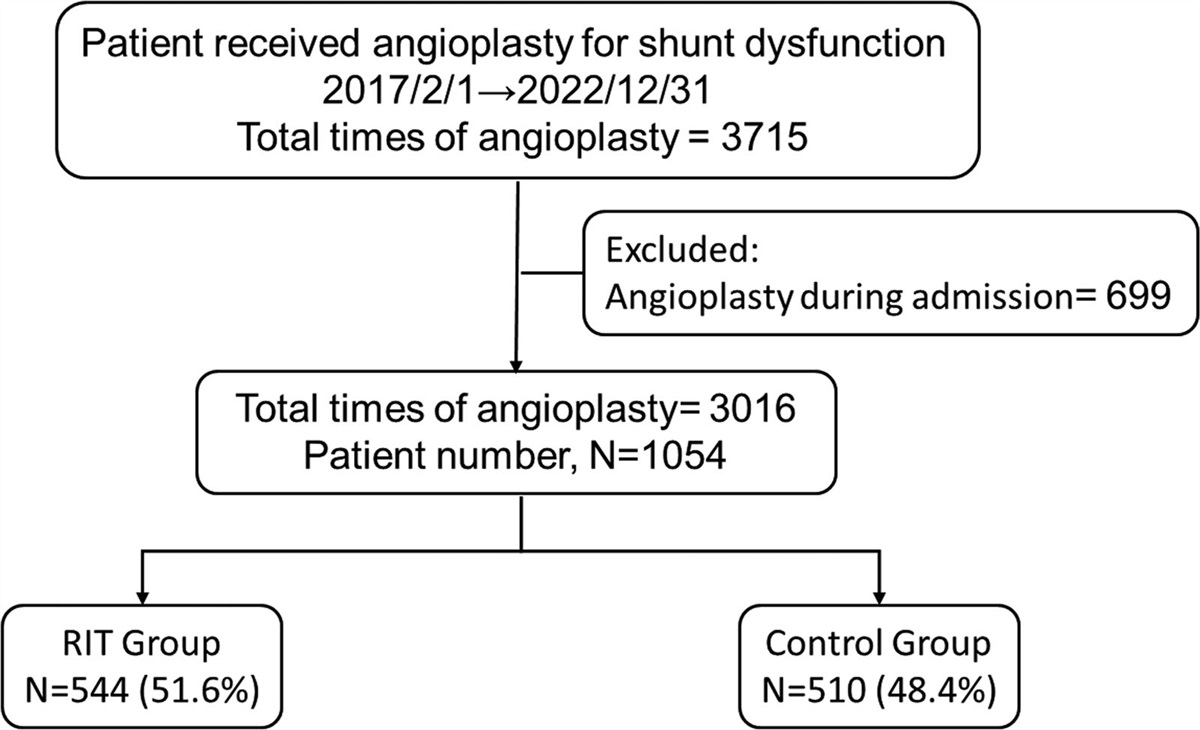
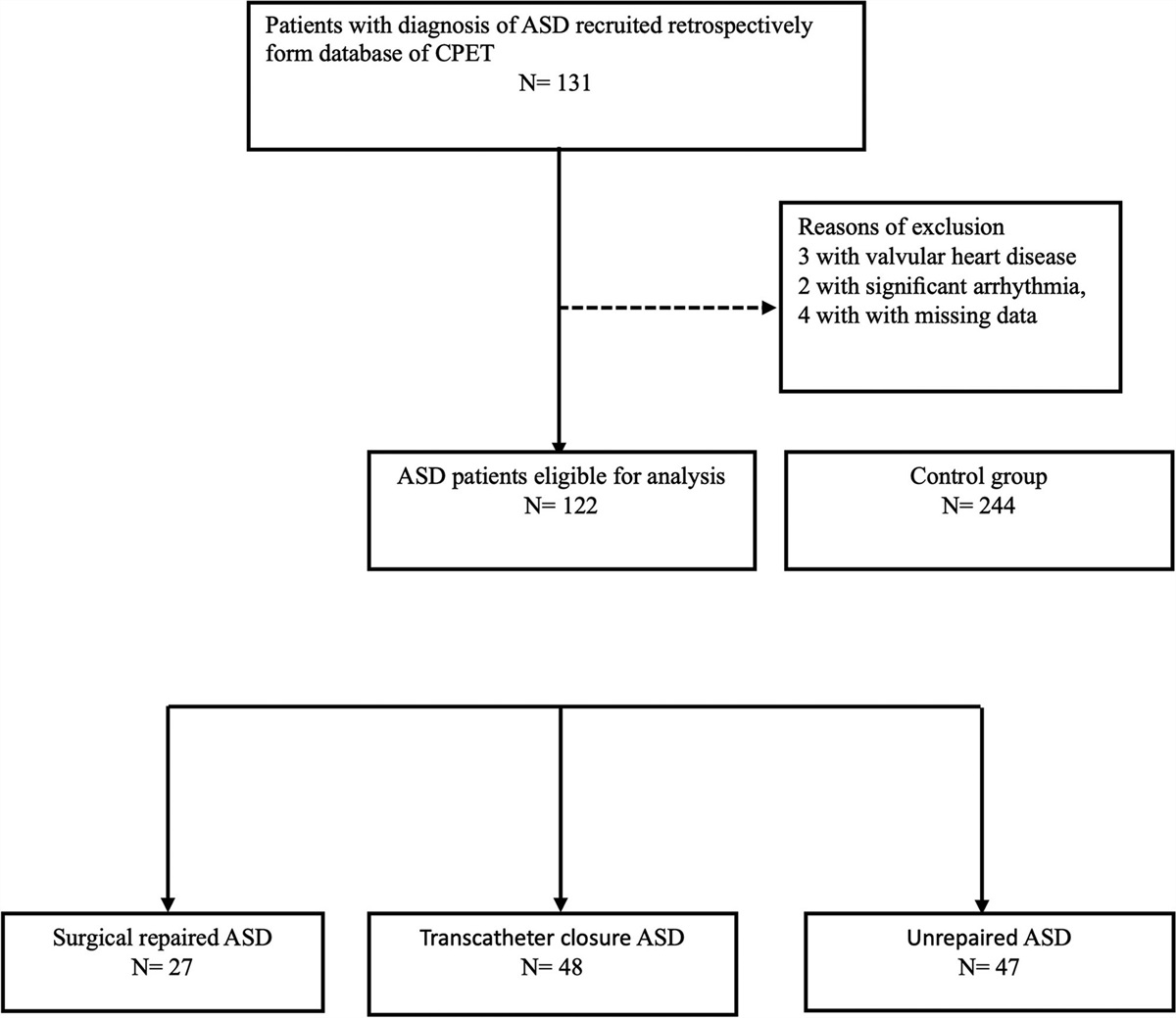
3. RESULTSThe current study consecutively enrolled 1054 patients, with a mean age of 67 ± 12 years, and 53% were men. Of these, 544 (51.6%) and 510 (48.4%) patients were in the RIT and control groups, respectively (Fig. 1). Table 1 shows the baseline characteristics of both groups. The background characteristics were almost matched between both groups except for a lower prevalence of diabetes mellitus and a higher prevalence of coronary artery disease in the RIT group.
Table 1 - Baseline characteristics between both groups Overall RIT Control (n = 1054) (n = 544) (n = 510) p Age, y 67 ± 12 67 ± 12 67 ± 13 0.82 Sex (male) 553 (53%) 292 (54%) 261 (51%) 0.42 Body mass index, kg/m2 24 ± 4 24 ± 4 24 ± 4 0.49 Diabetes mellitus 505 (48%) 237 (44%) 268 (53%) <0.01 Dyslipidemia 522 (50%) 267 (49%) 255 (50%) 0.77 Hypertension 675 (64%) 330 (61%) 345 (68%) 0.02 Old stroke 108 (10%) 51 (9%) 57 (11%) 0.34 Coronary artery disease 254 (24%) 152 (28%) 102 (20%) <0.01 Atrial fibrillation 153 (15%) 73 (14%) 80 (14%) 0.86 Heart failure 265 (25%) 142 (26%) 123 (24%) 0.46 Peripheral artery disease 81 (8%) 46 (9%) 35 (7%) 0.33 Cancer 177 (17%) 80 (15%) 97 (19%) 0.06 Left ventricular ejection fraction, % 64 ± 12 63 ± 13 65 ± 11 0.05Data are presented as mean ± SD or n (%).
RIT = rapid intervention team.
 Fig. 1:
Fig. 1: Flow diagram of the study cohort. RIT = rapid intervention team.
The number of cases significantly increased annually after the RIT strategy was implemented, even during the COVID-19 pandemic (Fig. 2). The annual number of PTA for dysfunctional AVF/AVG performed by medical interventionists increased from 97 in 2018 to 535 in 2022. Meanwhile, the number of PTAs performed by cardiovascular surgeons increased from 117 in 2018 to 293 in 2022. Therefore, the annual total number of PTAs for dysfunctional AVF/AVG increased significantly from 216 to 828 during this period.
 Fig. 2:
Fig. 2: Number of patients who received PTA for hemodialysis access from 2017 to 2022. The highlighted box (gray) represents the time interval when “rapid intervention team strategy” existed. CV = cardiologist; CVS = cardiovascular surgeon; PTA = percutaneous transluminal angioplasty.
Before 2020, no patients requiring PTA for dysfunctional AVF/AVG visited the operating room or catheterization laboratory through the OPD at our hospital. The time to intervention in patients through the ER significantly decreased (p for trend <0.001). The time to intervention in patients through the OPD did not significantly increase during the COVID-19 pandemic (30 ± 37 minutes in 2020 to 41 ± 43 minutes in 2022) (Fig. 3). The time to intervention for patients referred from dialysis rooms showed significant improvement from 12 ± 10 hours (before 2019) to 3.4 ± 2.8 hours (after 2019) (p < 0.01) after the RIT strategy was implemented (Table 2).
Table 2 - Time to intervention among patients from different sources Years 2017 2018 2019 2020 2021 2022 Emergency room: door to surgery/on-table CVS, min 382 ± 449 334 ± 335 271 ± 152 258 ± 149 282 ± 144 231 ± 117 CV, min N/A 91 ± 83 140 ± 94 132 ± 60 Outpatient appointment: check-in to the on-table CV, min N/A 30 ± 37 26 ± 28 41 ± 43 Dialysis room: dysfunction to surgery/on-table (h) 22 ± 16 12 ± 6 8 ± 7 4.1 ± 3.5 3.4 ± 3.3 3.0 ± 1.9Data are presented as mean ± SD.
CV = cardiologist; CVS = cardiovascular surgeon; N/A = not available.
 Fig. 3:
Fig. 3: A, Time to intervention for patients from ER. B, Time to intervention for patients from ER and OPD. The highlighted box (gray) represents the time interval when “rapid intervention team strategy” existed. ER = emergency room; OPD = outpatient clinic.
Overall, 7.2% of the patients were lost to follow-up, and 1.8% of the patients underwent permanent catheter or double-lumen catheter implantation and an arteriovenous shunt recreation within 3 days of shunt dysfunction during the follow-up period. The use of a double-lumen catheter for temporary dialysis access within 3 days of vascular access dysfunction was significantly lower in the RIT group (1% vs 6%, p < 0.01) (Table 3). Moreover, permanent catheter implant or shunt recreation was also significantly lower in the RIT group (1% vs 28%, p < 0.01).
Table 3 - Management within 3 d for patients with dysfunctional hemodialysis access RIT Control p (n = 544) (n = 510) Double-lumen insertion 7 (1%) 31 (6%) <0.01 Permanent catheter implantation or arteriovenous shunt recreation 3 (1%) 142 (28%) <0.01Data are presented as n (%).
RIT = rapid intervention team.
The mortality rate among patients who received the RIT strategy was 5.1% during a mean follow-up of 2.3 ± 1.4 years. The cumulative survival rate between the RIT strategy and control groups was not statistically significant (p = 0.16). (Fig. 4).
 Fig. 4:
Fig. 4: Kaplan-Meier survival curves of the rapid intervention team strategy and traditional groups (control).
4. DISCUSSIONTo the best of our knowledge, this is the first study to use the RIT strategy and team cooperation to improve the number of PTAs, accelerate time to intervention, and reduce temporary or permanent catheter implantation and shunt recreation for arteriovenous shunt dysfunction or failure in patients undergoing hemodialysis through ER, OPD, or dialysis clinics, even during the COVID-19 pandemic.
Consulting cardiologists in the emergency department is time-consuming. First, the cardiologists should take time to finish their clinical work, contact technicians in the catheter laboratory, and seek available rooms while cardiologists are directly consulted. Routine schedules during the daytime in either the catheterization laboratory or the operating room at a tertiary referral center led to limited availability of manpower and vacant rooms for intervention. In addition, during the COVID-19 pandemic, the policy of a rapid test for COVID-19 infection before invasive procedures could probably delay the procedure schedule. Our data showed that with the help of a case manager, the complicated process and time-consuming workload from consultation could be avoided, thereby shortening waiting time. The time to intervention after the RIT strategy was implemented at <2 to 3 hours was much better than guideline recommendations, indicating salvaging an obstructed dialysis access as early as possible, ideally within 48 hours.9,10 The time to intervention for patients through ER or OPD, or referred from dialysis clinics was not prolonged during the COVID-19 pandemic when COVID-19 rapid test and other additional examinations should be performed before arrival to the catheter room in the current study. The time to intervention even decreased among dialysis clinic-referred patients. Together, the RIT strategy is feasible and efficient.
With this multidisciplinary strategy, the case managers help to accelerate communication between different medical departments, thereby reducing the time to intervention and increasing patients’ willingness to visit hemodialysis clinics or refer to our hospital, thereby increasing the number of PTAs performed. The RIT strategy is a win-win situation not only for cardiologists and cardiovascular surgeons but also for patients.
With improved accessibility of the arteriovenous access intervention team, the need for double-lumen catheter insertion while dialysis access dysfunction occurred significantly decreased. The decreased recreation rate of vascular access might also be related to the improved accessibility of the vascular intervention team. This might theoretically improve the patient’s quality of life and reduce the risk of catheter-associated infection or complications with catheter insertion, although these measurements were not performed. Systematic reviews and randomized clinical trials reported that arteriovenous access had a high abandonment rate, ranging from 13.9% to 21%.11–13 We had only 1% of arteriovenous shunts that were eventually abandoned and required surgical revision.
Although the RIT strategy reduced double-lumen catheter insertion during the short-term period, it theoretically may not directly impact long-term outcomes. Consequently, the mortality rate was not significantly decreased among patients receiving the RIT strategy. Nevertheless, less need for double-lumen catheter insertion might improve patients’ quality of life.
The annual cost of hemodialysis access dysfunction-related morbidity was more than 1 billion dollars annually in the USA in 1996 and had increased to 5 billion USD in 2013.14,15 Vascular access dysfunction leads to ER visits and admissions, potentially increasing the burden on the health care system. In our study, the patients were mainly delivered through the OPD with the RIT strategy. Brenner et al16 reported that the inpatient costs associated with the management of AV shunt dysfunction could be approximately five times higher than those associated with outpatient care. By bypassing the ER or through admission, the medical costs for these patients have decreased. This approach enhances the availability of dialysis access intervention, potentially reducing the overall cost of care for AV shunt dysfunction.
Our trial has limitations, including the retrospective nature of this trial, and most of our enrolled patients were managed by cardiologists. The relatively low number of double-lumen catheter insertions compared with the permanent catheter and shunt recreation might be related to the retrospective nature of this cohort. Furthermore, with only 5 years of follow-up and less data before the COVID-19 pandemic, further follow-up of these patients might provide more information on the benefits of the RIT strategy for malfunctioning arteriovenous accesses.
In conclusion, the implementation of the RIT strategy improves the quantity and quality of PTA for arteriovenous shunt dysfunction or failure in patients undergoing hemodialysis. A prospective randomized controlled trial should be conducted in the future.
ACKNOWLEDGMENTSThis work was supported by the grants from the National Cheng Kung University Hospital (NCKUH-11205001).
REFERENCES 1. Saran R, Robinson B, Abbott KC, Agodoa LY, Albertus P, Ayanian J, et al. US renal data system 2016 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis. 2017;69(3 Suppl 1):A7–8. 2. Chen CF, Chen FA, Lee TL, Liao LF, Chen CY, Tan AC, et al. Current status of dialysis and vascular access in Taiwan. J Vasc Access. 2019;20:368–73. 3. Lai TS, Hsu CC, Lin MH, Wu VC, Chen YM. Trends in the incidence and prevalence of end-stage kidney disease requiring dialysis in Taiwan: 2010-2018. J Formos Med Assoc. 2022;121(Suppl 1):S5–11. 4. Salman L, Rizvi A, Contreras G, Manning C, Feustel PJ, Machado I, et al. A multicenter randomized clinical trial of hemodialysis access blood flow surveillance compared to standard of care: the hemodialysis access surveillance evaluation (HASE) study. Kidney Int Rep. 2020;5:1937–44. 5. Hsieh MY, Lin L, Chen TY, Chen DM, Lee MH, Shen YF, et al. Timely thrombectomy can improve patency of hemodialysis arteriovenous fistulas. J Vasc Surg. 2018;67:1217–26. 6. Sadaghianloo N, Jean-Baptiste E, Gaid H, Islam MS, Robino C, Declemy S, et al. Early surgical thrombectomy improves salvage of thrombosed vascular accesses. J Vasc Surg. 2014;59:1377–84.e1. 7. Prologo JD, Minwell G, Kent J, Pirasteh A, Corn D. Effect of the time to intervention on the outcome of thrombosed dialysis access grafts managed percutaneously. Diagn Interv Radiol. 2014;20:143–6. 8. Asif A, Byers P, Vieira CF, Roth D. Developing a comprehensive diagnostic and interventional nephrology program at an academic center. Am J Kidney Dis. 2003;42:229–33. 9. Vascular Access Work G. Clinical practice guidelines for vascular access. Am J Kidney Dis. 2006;48(Suppl 1):S248–73. 10. Tordoir J, Canaud B, Haage P, Konner K, Basci A, Fouque D, et al. EBPG on vascular access. Nephrol Dial Transplant. 2007;22(Suppl 2):ii88–117. 11. Jeong S, Kwon H, Chang JW, Han Y, Kwon TW, Cho YP. Outcomes of arteriovenous access among cancer patients requiring chronic haemodialysis. BMC Nephrol. 2020;21:297. 12. Chang R, Alabi O, Mahajan A, Miller JS, Bhat KR, Mize BM, et al. Arteriovenous fistula aneurysmorrhaphy is associated with improved patency and decreased vascular access abandonment. J Vasc Surg. 2023;77:891–8.e1. 13. Solesky BC, Huber TS, Berceli SA. Patient-centric analysis of dialysis access outcomes. J Vasc Access. 2010;11:31–7. 14. Thamer M, Lee TC, Wasse H, Glickman MH, Qian J, Gottlieb D, et al. Medicare costs associated with arteriovenous fistulas among US hemodialysis patients. Am J Kidney Dis. 2018;72:10–8. 15. Roy-Chaudhury P, Kelly BS, Narayana A, Desai P, Melhem M, Munda R, et al. Hemodialysis vascular access dysfunction from basic biology to clinical intervention. Adv Ren Replace Ther. 2002;9:74–84. 16. Brenner L, Singh AK, Campbell D, Frei F, Winkelmayer WC. Associations between demographic factors and provider structures on cost and length of stay for hemodialysis patients with vascular access failure. Clin J Am Soc Nephrol. 2006;1:455–61.
Comments (0)