This study evaluated the changes in reporting NDO-related terms and clustering of reports associated with maternal VPA exposure and NDOs in offspring. The number of ICSRs related to NDOs increased over time, particularly after 2010, with a broader range of terms being used to describe NDOs. This trend was observed for both VPA and the comparator AEDs. The proportion of NDO-related clusters of reports among all identified clusters has remained stable over time.
Although key scientific publication on VPA-related NDOs preceded a small rise in reported cases, the extent to which these developments contributed to the observed increase remains unclear. No acute change in the trend of reporting was observed following the selected regulatory decisions. The influence of key publications and international regulatory guidelines appears to be limited, suggesting that reporting may rely more on peer-established practices and follow developments in the clinical field, among which there is widening of diagnostic criteria.
An increase in the number of reports can have various causes. It might reflect a genuine rise in incidents within the population, but it cannot be ruled out that reports are submitted in batches by a contributing country and subsequently uploaded to VigiBase. In such cases, the increase would appear suddenly and within a single month. Changes in reporting behaviour, however, are generally expected to occur over a longer period.
4.1 Methodological Considerations
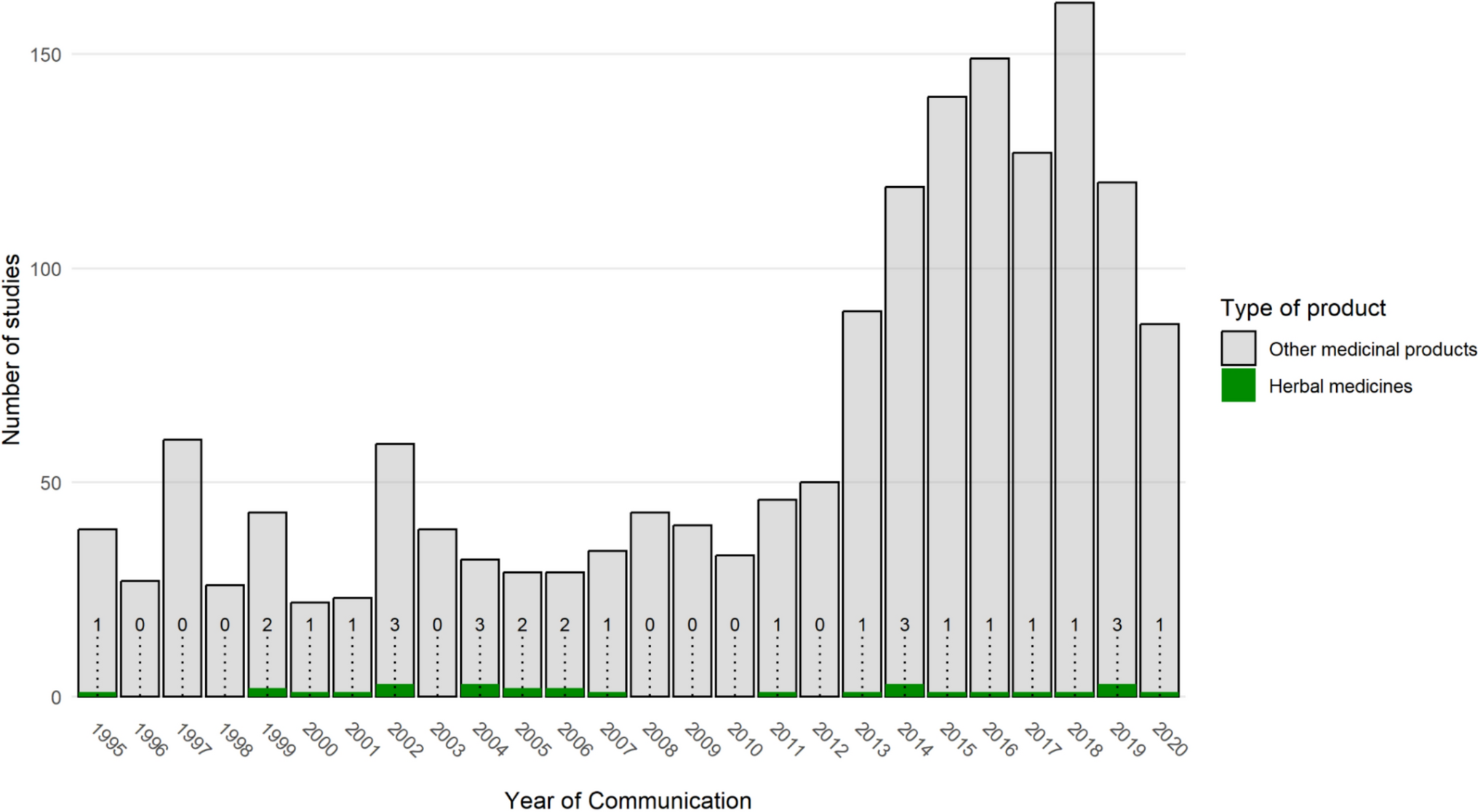
The spontaneous reporting system serves as a primary signal-generating tool and remains the most critical early warning tool for identifying previously unknown and rare ADRs in non-pregnant populations [37]. To date, it has not proven itself in teratogen signal detection. Although the first publications on developmental impairment were already published in the late 1980s (23), the number of ICSRs on NDOs following foetal AED exposure stayed relatively low till around 2010.
The number of ICSRs should ideally be interpreted in the context of their usage. Unfortunately, study drug utilisation data for AEDs were not available. It is likely that VPA prescriptions have declined over time, with pregnant women being switched to alternative AEDs. In the UK, repeated cross-sectional analyses from 2004 to 2018 showed a decrease in the prevalence of use of VPA during pregnancy [38]. Unfortunately, we did not have data on the number of ICSRs relative to the number of users of VPA on a global scale.
Neurodevelopmental outcomes are almost never apparent at birth but suspected by the age of 2–3 years and usually diagnosed at school age, especially for conditions that manifest later in life, such as autism or disorders in speech, language and learning development. Reporting of NDOs is therefore partly dependent on the timing of the diagnosis. An increase in reported cases could also be linked to a past rise in the use of VPA, with the diagnosis only being made at a later stage.
The study was conducted to gain insight into the differences in reporting the number and nature of symptoms related to NDOs, particularly in relation to key regulatory decisions and publications. A descriptive approach was chosen instead of a statistical test. The latter, such as an interrupted time series analysis, relies on fixed points in time, yet it is uncertain when any effects on the number and nature of reports, in relation to these key moments, would be observable. Neurodevelopmental outcomes encompass a broad range of conditions that affect the development of the nervous system. It is important to note that the selected terms do not comprehensively represent the full spectrum of conditions that fall under neurodevelopmental outcomes. While for mapping changes in NDO reporting we had specified PTs in advance to keep the outcome of the analysis manageable, this was not the case for the cluster analysis, for which an open-ended approach was adopted so as not to guide the choice based on clinical insight.
Both LTG and CBZ were used as comparator drugs because, as opposed to VPA, regulatory measures were taken for neither. As shown in Table T4 of the ESM, reporting NDO between CBZ and LTG was comparable, and results were therefore combined.
While a clinical condition might be documented as a well-defined diagnosis, it could also appear as a combination of multiple symptoms. A cluster analysis enables the identification of groups of ICSRs within a data set that show a close resemblance in respect of the reported PTs; for example co-reported events. Even if these symptoms are not recognised and reported as a single clinical entity, a cluster analysis can potentially identify them based on similarities between reports. The clustering of the reports in this study is based on statistical patterns of reported events and was conducted at four different points in time. For this reason, it was assessed manually whether these clusters also represented clinically relevant AEs related to NDOs. It seemed that for clusters identified more recently in time, more reports contributed, and reported PTs seems to be more closely related. None of the clusters revealed a combination of PTs solely related to NDOs, which is expected, given that ICSRs often include reports of various AEs and that teratogens often interrupt typical developmental processes of a range of bodily organs. Even within clusters, PTs that belong together sometimes could be distinguished. An example is cluster 2014-1 that encompassed both related events to central nervous system disorders such as “neural tube defect” or “spina bifida” as well as congenital heart defects such as “Congenital cardiovascular anomaly” or “Heart disease congenital”. Our assessment showed that while related reports can be logically grouped, a further clinical evaluation is needed to interpret the content of the identified clusters.
There was “substantial agreement” among the three reviewers in determining whether evidence of NDOs or morphological abnormalities was present in the identified clusters. The lower interrater agreement for the “Other disorder” cluster may be partly because of its less well-defined nature, allowing for multiple interpretations. This contrasts with the clearer definitions of the categories NDO and “morphological disorder”.
4.2 Evolution of the Term NDO
Previously, the PT “Developmental Delay” was commonly used to describe a range of neurodevelopmental issues. However, with the introduction of more specific terms to differentiate conditions within the neurodevelopmental spectrum, the use of this broader term may have declined. Additionally, as children grow older, the general label “Developmental Delay” tends to be replaced with more precise diagnoses, contributing to improved accuracy.
The way NDOs manifest can change throughout life. While some conditions may be diagnosed at a young age, their associated symptoms may only fully emerge later. This can also contribute to the variation in reported symptoms, which is partly influenced by the development of the NDO over time and reporting the diversity of its associated symptoms. With studies on NDO providing a more detailed understanding of the condition, the nature of reported AEs may have also evolved over time. In addition, the diagnostic process was improved [39]. The publication of the DSM-5 in 2013 further increased awareness as the term “Neurodevelopmental Disorders’’ had not been included in previous editions of the DSM [40, 41]. Among the major changes of the DSM-5 is that some disorders have been merged together, placing them within a spectrum, including autism spectrum disorder [42].
The change in the reporting of NDOs is also reflected in the results of the cluster analysis. The number of reports underlying each cluster varied significantly, from as few as 9 to as many as over 600. As the total number of reports increases, larger clusters are highlighted as seen in Table 1. This is because of an increase in the number of ICSRs that reflects a larger and more diverse dataset, encompassing a broader range of symptoms, patient characteristics and other factors. The relative number of clusters related to NDOs appears to be stable over time. In 2009, two out of eight (25%) and in 2023, 6 out of 21 (28%) of the clusters relate to NDOs. Because of the emergence of more specific terms related to NDOs, the variety of MedDRA® PTs in the clusters identified from 2018 and 2023 increased.
4.3 Notoriety Bias
Particularly in the early years, the relationship between VPA and NDOs may not have been widely recognised. It cannot be ruled out that, after the relationship became known, there was an increase in the number of reported cases. A similar effect was observed with the association between dolutegravir and neural tube defects, where all cases in VigiBase were reported after the safety signal on neural tube defects was highlighted by the media [43]. Over the years, the association between VPA and NDOs has often raised media attention, potentially leading to notoriety bias. An example is media attention in the UK that occurred around 2010 following a law suit [44, 45]. While the number of reports increased after both the publication of Adab et al. [16] in 2004 and that of Meador et al. in 2009 [19], attributing this risk solely to a publication is difficult for various reasons. First, earlier case reports and studies already focused on the relationship between the use of AEDs during pregnancy and cognitive difficulties in offspring [15, 23], although a greater awareness may have caused an earlier recognition and reporting of a broader range of terms related to NDOs.
Second, some NDO-related events occur immediately after in utero exposure to VPA, while other events can only be identified and thus reported, later in life. In addition, an increased attention to the VPA–NDO association may have changed prescribing practices and the switching of pregnant women to alternative convulsant medications. Furthermore, the restrictions in use and the risk minimisation measures might have resulted in fewer exposures. Therefore, the ultimate effect of the increasing awareness of this association is difficult to predict.
In October 2014, the VPA–NDO signal was raised by the EMA followed by new restrictions and the establishment of a pregnancy prevention programme in 2018 [25, 26]. Although an increase in AEs in subsequent years can be observed, a relationship with these European regulatory measures is difficult to establish. Healthcare professionals may have already been informed about this association through publications or professional organisations, which could have lessened the impact of a regulatory decision. In contrast, it is likely that consumer awareness primarily depended on media coverage of the regulatory actions. Following the regulatory decision in May 2018, a public hearing was held at the EMA [46]. Although it is plausible that this may have contributed to an increase in the number of reports gradually over time, no acute peak in reporting was observed.
Notoriety bias likely extended beyond VPA to other AEDs and medications. The marked increase in the number of reports for both VPA and comparator AEDs might suggest that the VPA–NDO signal may have prompted similar attention for NDOs with other AEDs rather than being specific to VPA alone. Indeed, our findings reveal that similar patterns in reported AEs (Figs. 1, 2) are observed with both VPA and the comparator drugs LTG and CBZ, although it cannot be ruled out that co-reporting of other AEDs may have played a role as well. This “ripple effect” has been previously described and occurs when an alert about a safety concern increases reports of similar issues in other products within the same class [10].
4.4 Strengths and Limitations
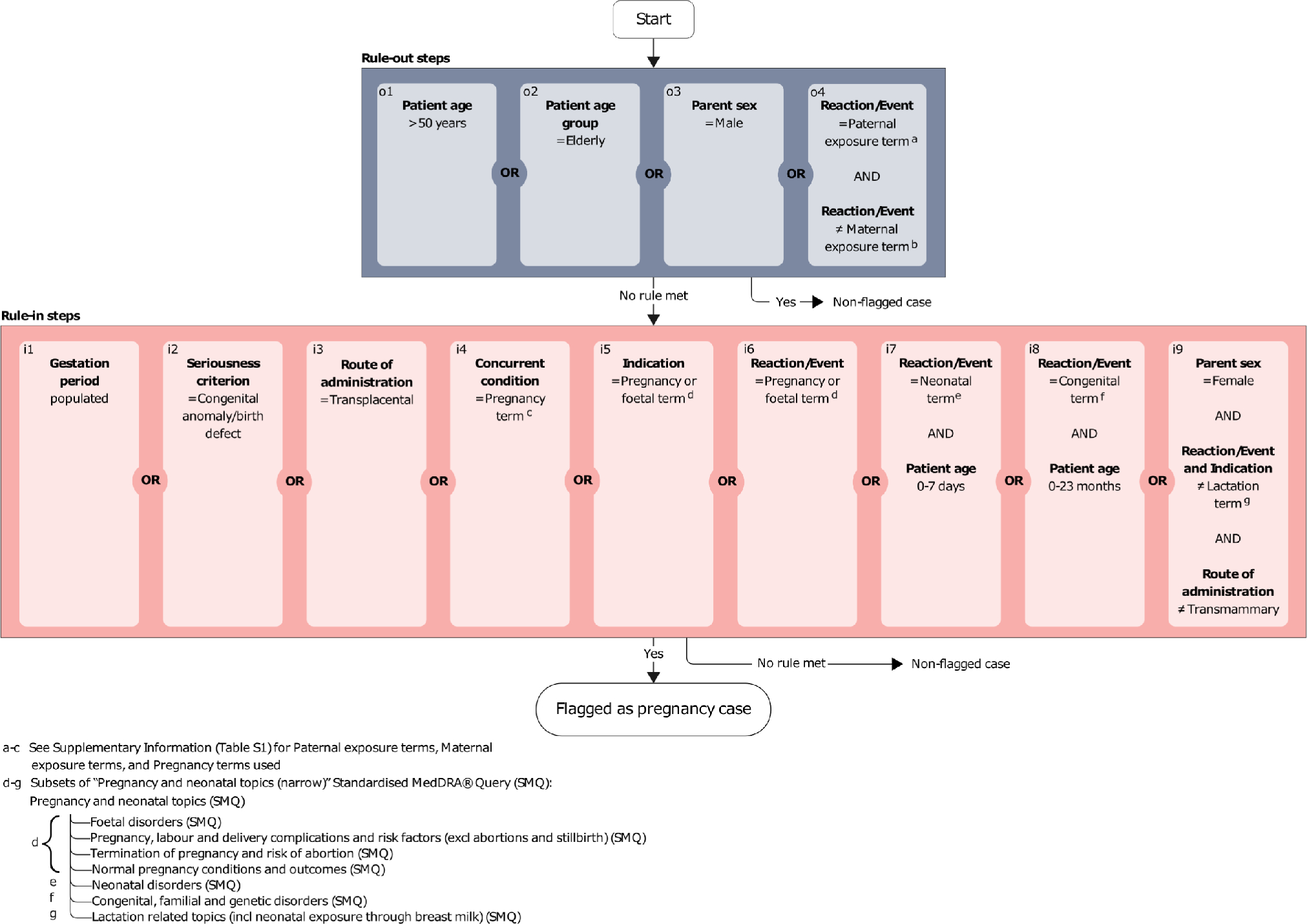
A key strength of our study is that the data used were collected from VigiBase containing over 34 million reports from more than 150 countries, among which 350,000 reports identified by the pregnancy algorithm. This study is one of the first studies in which a recently developed pregnancy algorithm was used to identify ICSRs describing exposures during pregnancy [47]. This allowed us to visualise reporting trends and patterns on NDOs related to the use of AEDs during pregnancy.
Our study also had some limitations. Reports in VigiBase come from a variety of sources, including healthcare professionals and consumers. A medical diagnosis is not always provided in the reports, and the strength of the causal relationship cannot always be determined. Since 2000, the number of reports by consumers has increased. It is known that the reported information between consumers and healthcare professionals may differ [48, 49]. In this study, we did not stratify by the source of reports, given the varying differences in the proportion of reports from healthcare professionals and consumers over time.
Although the analysis was based on drugs labelled as suspected or interacting by the reporter, it cannot be ruled out that concomitant use of AEDs may have influenced the reporting of NDOs. In 8.4% of the VPA reports, it is known that LTG or CBZ were co-reported, and in 33.6% of the CBZ/LTG reports, VPA was also used. As concomitant medications may not always be fully documented in the ICSRs, the actual figures of concomitant use may be higher. We did not apply exclusion because it is not certain whether this would have resulted in groups where no co-reporting was involved.
It is possible that older ICSRs were coded with the WHO Adverse Reaction Terminology, which may have influenced the variety of terms one could choose from. The MedDRA® terminology was developed in the late 1990s and gradually implemented worldwide [50]. However, the majority of changes in reporting occurred after 2009 and we expect the impact of coding with another terminology than MedDRA® to be limited.
The use of spontaneous data does not allow calculating an incidence rate of the AEs or make a comparison between medicinal products, owing to the unknown extent of underreporting and the lack of available prescription data [51]. Differences in reporting rates between VPA and the comparator drugs therefore do not necessarily reflect the incidence of the AEs in the population. This also made it challenging to account for changes in reporting NDOs over time because of shifts in prescribing patterns or varying levels of awareness by patients and healthcare professionals.
In this study, global reports were used, but the regulatory decisions analysed are specific to Europe. However, we expect that significant changes in the number of ICSRs within the European Union would have been reflected in the overall dataset.
A cluster analysis allows for the identification of groups of reports with similar patterns of reported terms. It should be noted that reporting of AEs in VigiBase may depend on other factors considered in this analysis, such as the reporting date or geographical region. For example, the use of the term “Developmental Delay” has been used less frequently relative to other terms in recent years in our study. Similarly, a specific diagnosis might be reported more often in one country compared to another. Unfortunately, we were not able to take this information into account in the cluster analysis. Another point of attention is that inherent to the method applied, only reports mentioning multiple PTs were considered in the cluster analysis and other factors such as comorbidity and concomitant medication could not be considered in the vigiGroup analysis.
Finally, a cluster analysis was conducted exclusively for VPA and not for the comparator drugs. The approach was exploratory and descriptive in nature. A previous study using the same method had shown that clusters tended to be relatively large, and comparisons were somewhat subjective, making it challenging to compare outcomes across different AEDs.[31]
4.5 Implications for Future Research
The way in which AEs are described and coded in ICSRs may evolve over time. This is not only applicable to NDOs and AEDs, but also to other AEs. Similarly, syndromes comprising multiple symptoms or diverse manifestations may be reported differently as time progresses. Several factors could contribute to these changes, such as differences in reporters’ backgrounds, changes in media coverage and increasing awareness, and the age of the individual at time of diagnosis, all of which can affect how AEs are documented over time. Additionally, the introduction of standardised definitions, such as those in the DSM-5, or the development of national and international guidelines for diagnosing and treating various conditions, may play a role in shaping AE reporting and may impact signal detection. Therefore, it is essential to understand how AE information has been reported, coded and stored in databases over the years and to conduct targeted research in this area.
The information available in ICSRs is often not detailed enough to accurately assess NDOs related to AEDs. Therefore, additional methods should be employed to obtain more specific information on the nature and development of these outcomes.

Comments (0)