It is known that there are sex differences in the rates of incidence of adverse reactions to diuretics, but the sex-specific effects of these drugs on patients’ physiological function have not been clarified. This is the first study to identify sex differences in the frequency of diuretic-associated electrolyte disturbances based on age and renal function using Japanese medical claims and health checkup data. The study included 67,135 patients who were taking diuretics and had eGFR data available. The largest proportion of patients prescribed diuretics were aged ≥75 years, followed by patients aged 65–74 years and non-elderly patients (Table 2). This finding probably reflects the fact that cardiac disease and hypertension are common in elderly patients and that use of diuretics is common in this age group. The chi-squared tests showed statistically significant differences in age distribution between men and women in all categories. However, the clinical relevance of this difference may be limited due to the large sample size, which can result in significant p-values even for small absolute differences.
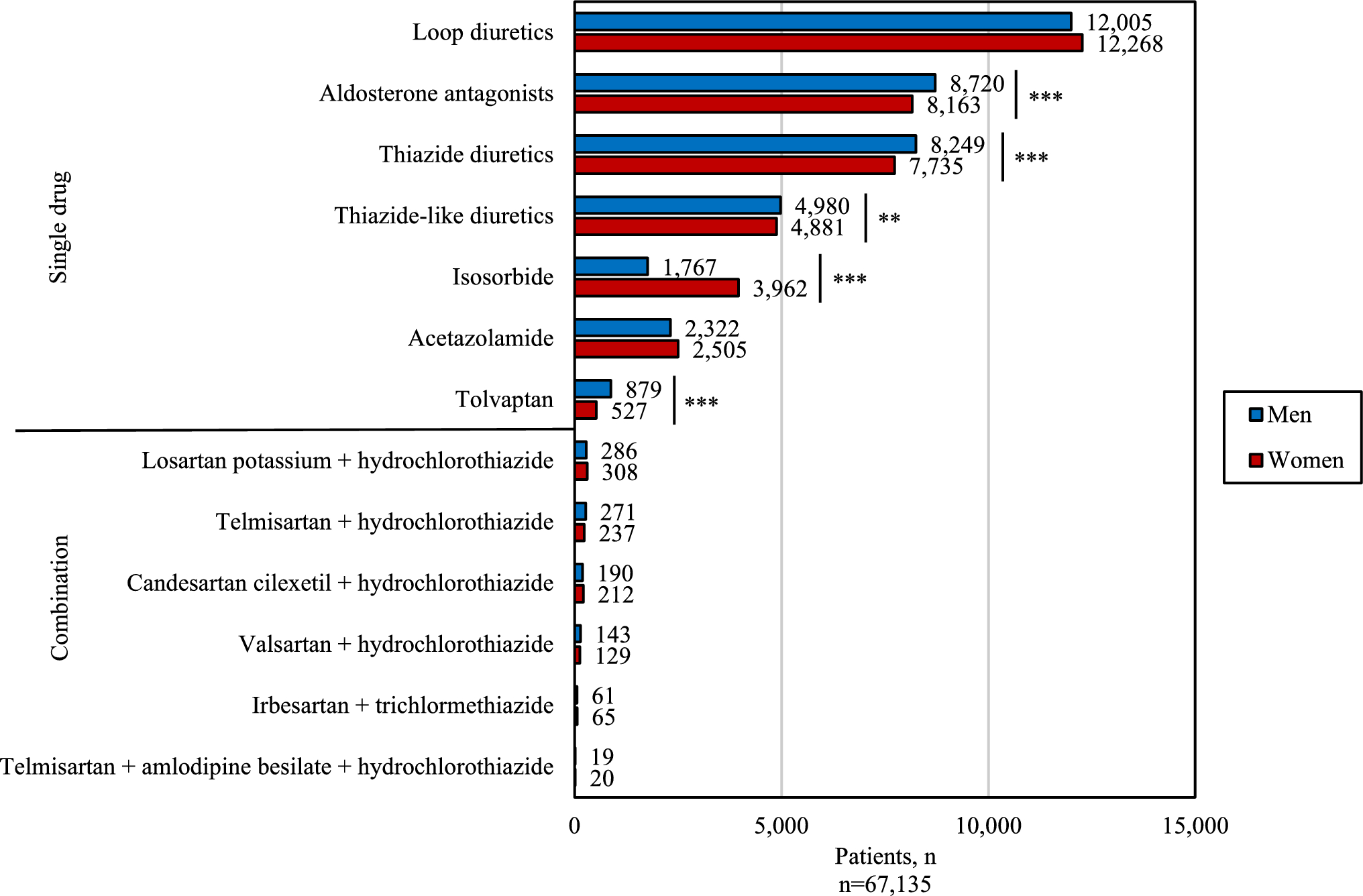
We found that aldosterone antagonists, thiazide diuretics, thiazide-like diuretics, and tolvaptan were prescribed more frequently in men (Fig. 1). According to a 2022 national survey, the percentage of people with systolic (highest) blood pressure of 140 mmHg or higher was 28.9% for men and 21.1% for women [34]. Therefore, it is possible that men are more susceptible to hypertension and therefore may have been using more diuretics. On the other hand, isosorbide, which is primarily used to treat Ménière’s disease, was prescribed more frequently in women. This finding probably reflects the high prevalence of Ménière’s disease among women in Japan [35]. In Japan, isosorbide is primarily prescribed for inner ear disorders such as Ménière’s disease and is classified under “diuretics” according to the Japanese standard commodity classification system. This differs from international classifications, such as in Europe, where isosorbide mononitrate and dinitrate are used as vasodilators for cardiovascular indications.
In our study, more patients were diagnosed with electrolyte disturbances as a result of potassium disturbances than because of sodium disturbances (Table 3). Further studies are needed to determine if there is a difference in the frequency of diagnosis of sodium and potassium disturbances in everyday clinical practice. Hyperosmolality and hypernatremia tended to be more common in men, while hypo-osmolality and hyponatremia tended to be more common in women, although the numbers were small, and these results were not significant. Furthermore, hyperkalemia was more common in men and hypokalemia was more common in women. Another study found that diuretic-induced hyponatremia and hypokalemia were common adverse events leading to hospitalization in women [23]. However, our study is the first to suggest that hyperkalemia may be more common in men.
Electrolyte disturbances are more likely to occur in the elderly (Fig. 2a), probably because physiological functions tend to deteriorate with advancing age. Potassium excretion is decreased in patients with renal disease, and in this study, the eGFR was much lower in patients who developed hyperkalemia than in those who did not independent of sex.
Loop diuretics are inherently likely to cause hypokalemia. However, when the data for patients who developed hyperkalemia and those who developed hypokalemia were compared (Fig. 3), the percentage of loop diuretics prescribed was similar in both groups. Analysis of the number and type of concomitant medications showed that 8717 of the 10,315 patients in this study who were prescribed two or more diuretics were prescribed loop diuretics. We found that loop diuretics were particularly likely to be prescribed with other types of diuretics. Therefore, the proportion of loop diuretics prescribed may have been similar for hyperkalemia and hypokalemia. However, although a loop diuretic may be prescribed to treat hyperkalemia [36], in this study, the first electrolyte disturbance that occurred during the period was analyzed for the drug that had been prescribed immediately prior to occurrence of the disturbance. Therefore, it is unlikely that loop diuretics prescribed for treatment of hyperkalemia are reflected in our results.
We found that hyperkalemia was more common in men than in women (Table 3). However, as shown in Fig. 3, there was no significant sex difference in the percentage of prescriptions. This finding suggests that hyperkalemia in men may be attributable to factors that are independent of diuretic classification. For example, chronic kidney disease is more likely to cause hyperkalemia as a result of reduced renal function, and previous studies have shown that chronic kidney disease is worse in men [37].
The ORs, 95% CIs, and p-values were analyzed for hyperkalemia and hypokalemia by age and eGFR category (Table 4). In general, as renal function declines, patients are more likely to develop hyperkalemia because potassium excretion is reduced as a result of a decreased glomerular filtration rate. Among patients aged ≥75 years, the odds of hypokalemia in women compared to men were significantly higher in the eGFR 60–30 and <30 mL/min/1.73 m2 groups. These findings suggest that particular caution is needed regarding diuretic-associated hypokalemia in elderly women with reduced renal function.
Figure 1 shows that 24,273 (36.2%) of the 67,135 patients in this study were taking loop diuretics, while Fig. 3 shows that approximately 60% of men and women who developed hyperkalemia or hypokalemia had been prescribed these drugs. These results indicate that loop diuretics are prescribed more frequently in patients with hyperkalemia and hypokalemia. Figure 4 shows that the proportion of loop diuretics prescribed increased to about 80% in patients aged ≥ 75 years with an eGFR of < 30 mL/min/1.73 m2. However, when compared with the total patient population, the percentage was similar indicating that the proportion of patients prescribed loop diuretics did not change with development of hyperkalemia or hypokalemia in those aged ≥ 75 years with an eGFR of < 30 mL/min/1.73 m2. Loop diuretics are less likely to cause hyperkalemia because of their mechanism of action, whereas aldosterone antagonists are less likely to cause hypokalemia. Nevertheless, agents with different mechanisms of action were prescribed for each potassium abnormality. This could reflect the fact that elderly patients often take multiple medications concomitantly, some of which may affect potassium balance. Furthermore, electrolyte disturbance is more likely to occur in elderly patients with impaired renal function. In addition, regardless of the type of diuretic, adverse reactions may be more likely to occur because of sex differences in pharmacokinetics. Several studies have reported that the organization and expression of renal transporters differ between male and female rats [38]. These differences, particularly in the regulation of sodium reabsorption along the nephron, may contribute to sex-specific susceptibility to the development of electrolyte disturbances.
This study had some limitations. First, we defined an electrolyte disturbance as an adverse reaction if the patient had taken a diuretic within the 14 days before diagnosis, considering the possibility that the patient took their remaining medication as well as the time needed for the medication to be eliminated from the body. However, this definition may not necessarily apply to all patients. We excluded intravenous diuretics, which are commonly used in hospitalized patients, in an effort to mimic the general population of diuretic users. Therefore, the possibility that information for patients with poor health status was overlooked cannot be excluded. The eGFR is calculated using the serum creatinine level, age, and sex and is defined as a laboratory indicator. The diagnostic criteria for chronic kidney disease include a decrease in eGFR, with diabetes mellitus as a risk factor [39]. Sex differences in the incidence of these diseases may influence the incidence of adverse reactions. In addition, we did not include comorbidities such as diabetes mellitus, heart failure, or chronic kidney disease in our analysis due to the difficulty in establishing a clear temporal relationship between their diagnosis and the occurrence of electrolyte disturbances. These comorbid conditions may independently contribute to the development of electrolyte disturbances regardless of diuretic use. Future research should aim to incorporate comorbidity profiles using data sources that allow for more temporally aligned diagnostic information. Furthermore, patients aged younger than 20 years were excluded because eGFR is a measure of renal function in patients aged older than 20 years. Electrolyte disturbances were identified based on diagnosis codes (ICD-10) in claims data (Table 1). As such, we could not assess the severity of these conditions at the time of diagnosis. This limits the clinical interpretability of our findings, especially in distinguishing between mild and life-threatening cases. Because the health checkup data from which the eGFR values were obtained are generally recorded once a year, it is possible that the most recent electrolyte disturbance was not linked to the eGFR value. It is possible that other concomitant medications besides diuretics may have been involved in renal function and electrolyte regulation. In this study, subgroup analyses, such as those based on specific diuretic classes or patient populations, including methods like propensity score matching, could not be conducted because the dataset included only patients who were prescribed diuretics. No untreated comparison group was available, limiting our ability to adjust for baseline characteristics between groups. Future studies incorporating both treated and untreated populations would enable more robust comparative analyses.
The observed sex differences in adverse event rates may also be partly attributable to the underrepresentation of women in randomized controlled trials, leading to limited generalizability of trial findings to female patients. Addressing this gap in future clinical research is crucial to ensure evidence-based pharmacotherapy across sexes.
In summary, the findings of this study suggest that it is important to be aware of hypokalemia as an adverse reaction when diuretics are used in elderly women with a low eGFR. Regular renal function tests and monitoring for early signs of electrolyte disturbances are necessary in these patients.

Comments (0)