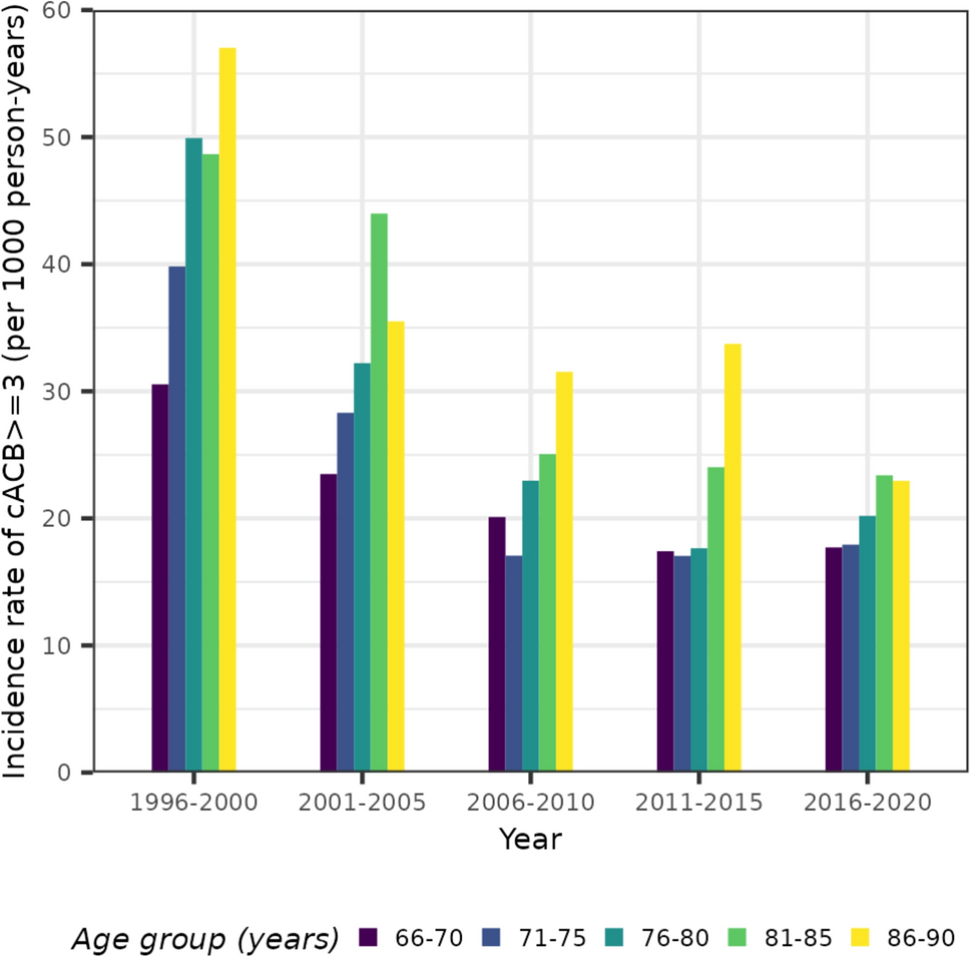
Drugs with anticholinergic activity are frequently prescribed to older persons, with a cumulative incidence of cACB ≥ 3 of 25% between 1996 and 2020. Comparing the community-dwelling participants over time and by age, the IR of a cACB ≥ 3 decreased significantly between 1996 and 2020 for all age groups. However, over time, participants aged 86–90 years remained to have the highest IR compared with participants aged 65–70 years. Participants aged 86–90 years had a 1.5 times higher rate of a cACB ≥ 3, even after adjusting for the episode. As these are patients with increased risk of falls, delirium, and cognitive impairment, this might therefore be of concern.
Several studies have described changes in the prevalence rates of the ACB. However, to our knowledge, this is the first study to describe the cumulative incidence and IRs of a cACB ≥ 3 according to the Anticholinergic Cognitive Burden scale. A few studies have described changes over time. So far, evidence has been mixed; three studies found a decrease in the prevalence [18,19,20], while two others found an increase in the prevalence [21, 22]. However, a possible peak of exposure to anticholinergics may have been around the year 2010 [18, 21, 22] and could explain these inconsistent results when studies only measured two time points. In addition, the prevalence in the studies varies greatly, ranging from 4.7–46%, perhaps due to differences in the used scoring scales and criteria for the anticholinergic drug burden exposure. Although some studies used the Anticholinergic Cognitive Burden scale, they only evaluated drugs with an ACB score of three. However, we assessed a total score of three or more, as this total score is considered clinically relevant [24].
To gain insight into the drugs that caused the high ACB, we identified the five most frequently used drugs with an ACB score equal to three. For the combined incidence of an amitriptyline or paroxetine prescription, the decline in incidence across time is similar to the trend seen for the incidence of cACB ≥ 3. Prescribers should consider nortriptyline as an alternative to amitriptyline and paroxetine. In vitro, nortriptyline has a lower anticholinergic activity than amitriptyline [25]. This could be the reason why nortriptyline has a lower score on some other anticholinergic score scales [26]. Thus, nortriptyline may be preferred over other tricyclic antidepressants to lower the risk of adverse effects due to anticholinergics [27].
A major problem in older people is urinary incontinence, and anticholinergics can help reduce the symptoms of it. A stationary trend was found for the spasmolytics oxybutynin, solifenacin, and tolterodine. Solifenacin has been on the Dutch market since 2004, which could explain the increase until 2010. To reduce the ACB of a patient, mirabegron, a spasmolytic without anticholinergic drug activity, can be considered [28, 29].
Generally, for both the treatment of depression and urine incontinence, nonpharmacological treatments are preferred. However, when nonpharmacological treatments are insufficient, pharmacotherapy can be prescribed. When pharmacotherapy is prescribed and drugs with similar efficacy are considered, drugs with the lowest anticholinergic burden should, in our opinion, be preferred.
There are several limitations to this study. First, we extracted pharmacy dispensing records only once every year. Thus, when a patient does not obtain the medication consistently, we could have an over- or underestimation of the magnitude of ACB, albeit this would lead to nondifferential misclassification. Second, we could not include over the counter (OTC) medication. Therefore, our findings may underestimate the incidence of cACB ≥ 3. Albeit, OTC medication is generally indicated for a short amount of time. Third, one of the major challenges lies in defining the anticholinergic medications and their burden. There is a lack of consensus on which is the best scale for scientific research or clinical practice. We chose the Anticholinergic Cognitive Burden Score scale as it is the scale that is modified by EPHOR and used in clinical practice in the Netherlands. Recently, a new ACB scale has been developed that is based on drug properties to determine the ACB, instead of expert-based opinions. However, it has not been clinically validated [30]. Contrary, the Anticholinergic Cognitive Burden Score scale is the most frequently validated expert-based anticholinergic scale for adverse effects [10]. We chose a cutoff value of three or more because the Anticholinergic Cognitive Burden Score scale considers it clinically relevant [11, 13]. In addition, we chose to supplement this scoring scale with the ACB scale by EPHOR because it is the scale that is used by clinicians in the Netherlands. Lastly, we note that we examined the incidence of a cACB ≥ 3. Therefore, we did not measure or account for the period of time a patient had a cACB ≥ 3. A frequent or less frequent user were both counted as a case and consequently censored. Thus, no conclusion can be drawn in regard to the length of use of anticholinergic drugs.
There are several strengths of this study. This study is one of a few to explore temporal trends of the ACB with data collected over a long follow-up period of 25 years and is the first to explore the incidence of the ACB over this timeframe. Furthermore, this is the first study to present data on the exposure of cACB ≥ 3. A cACB ≥ 3 is considered clinically relevant and is advised to be avoided when possible in the oldest of older adults, as these are the persons with increased risk of falls, delirium, and cognitive impairment [3, 11, 24]. Thus, our results give insight into the proportion of people who might have a relative contraindication for cACB ≥ 3.

Comments (0)