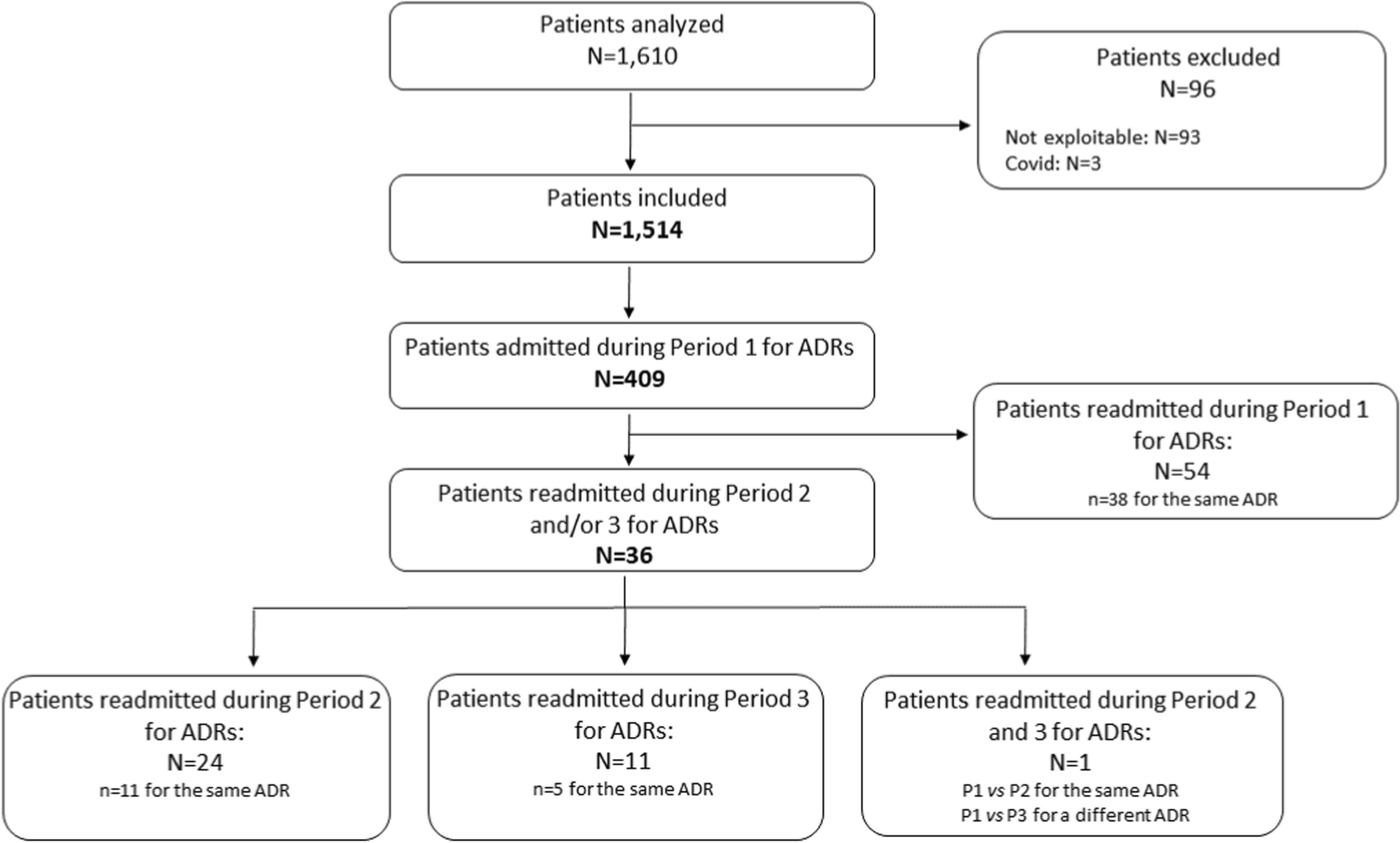
This study performed at TUH identified that one-third of NHRs admitted to the ED in 2019 were because of an ADR. This high rate could indicate the failure of the NHs to handle complex situations. Hospital admissions at the end of life are still too frequent in this setting. In our study, the proximity of NHs to a university hospital center could also have contribued to their transfer. Moreover, 8.8% of patients admitted for an ADR during this year were re-admitted during the next 2 years, half of whom for the same ADRs. Factors associated with ADR-related admissions were the number of drugs (with a population exposed to an average of six medications), previous ED admission (in the year before the index ED admission), and overweight.
According to a previous study conducted using the same method and at the same hospital, 15.7% of patients aged over 65 years admitted for ADRs in 2010 were re-admitted for ADRs within a year [15]. Zhang et al estimated that 17.7% of patients aged over 60 years were re-admitted for ADRs within 3 years [28]. The difference between our results and these studies could be owing to the management of some ADRs by general practitioners in NHs leading to fewer hospital admissions. However, to our knowledge, no data are available on the readmission rates of NHRs for ADRs. Through a 4-year prospective observational study, Cooper found that 15.7% of hospitalizations among NHRs were for ADRs with a recurrence rate of 8% for the same issue, similar to our results [29]. Our findings suggest that 3.9% of NHRs admitted during 2019 (estimated at 0.3 per 100 residents per month) for ADRs had a fatal outcome (i.e., ADRs assessed as the cause of death). Similarly, Ayani et al. estimated a fatal ADR rate of 0.3 per 100 resident-months in NHRs in Japan [30].
The most frequent ADRs leading to ED admission were falls, hemorrhagic events, and constipation. Ayani et al. also reported similar results identifying neuropsychiatric events as the most frequent, followed by falls due to neuropsychotropic drugs, gastrointestinal events, constipation, and hemorrhagic events [30]. Cooper et al. found that falls in NHRs were mainly due to psychotropic drugs, digoxin overdose, and insulin-related hypoglycemia. The differences observed compared with this latter study may be explained by changes in the therapeutic regimens of NHRs, including less use of digoxin and a better management of insulin [29]. In our study, falls leading to ED admission were the most frequent ADRs. However, this type of adverse event in older persons remains multifactorial and could be related to environmental factors, visual deficits, cognitive decline, balance disturbance, and several drugs that could contribute to falls through various mechanisms (hypoglycemia, muscle weakness, hypotension) [31]. A cross-sectional study based on US Medicare data showed that the incidence of falls was higher among medication users (10.3%) compared to people with no history of medication use (5.4%) [32]. Oya et al. reported that over half of falls in NHRs in Japan were associated with psychotropic drugs [33]. Cox et al found a three-fold increase of fall incidence among NHRs in the Netherlands was associated with psychotropic drug use [34]. Kojima et al. also reported that polypharmacy rather than comorbidities was associated with fall risk [35]. Finally, Zhou et al. suggested that almost half of cases of drug-induced falls in older patients recorded in the US Food and Drug Administration Adverse Event Reporting System was related to psychotropic drug use [31].
Concerning suspected drugs as the factor contributing or leading to ED admission, psychotropic drugs were the most frequently implicated in our study, which could lead to falls (e.g., benzodiazepine derivatives and antidepressants), followed by antithrombotic drugs leading to hemorrhagic events (e.g., anticoagulants and antiplatelet drugs), and opioids leading to fecaloma/constipation. The association between benzodiazepine exposure and falls and hip fractures has been well established for years [36, 37]. Among benzodiazepines involved in falls, oxazepam was the most frequently reported (73%) despite being the recommended benzodiazepine for older patients when necessary and for short-term treatment. In medical records, the date of initial prescription was not available, but the notion of “a long-term treatment” was often mentioned. Couret et al. also suggested an increase in the lack of association of laxatives with opioids similar to our study. They also highlighted a worsening of adherence to recommendations regarding the duration of a prescription, which may be explained by the frailty and severity of psychobehavioral disorders in NHRs [38]. Inappropriate benzodiazepines (bromazepam and clorazepate) are still prescribed in older patients. Regarding hemorrhagic ADRs related to antithrombotic agents, assessing their appropriateness remains challenging owing to the presence of cardiovascular risk factors in this frail population. Opioid-related constipation and/or fecaloma should be considered as “partially avoidable” as the use of laxatives is recommended for long-term opioid treatment [39, 40]. In our study, 43% of patients admitted for drug-related constipation/fecaloma did not receive a laxative. In cases where a laxative had been prescribed, it was sometimes ineffective in preventing constipation, likely owing to the combination of several drugs (psychotropic drugs, anticholinergics, opioids), the inappropriate choice of laxative, dietary factors, and the overall profile of NHRs (e.g., lack of physical activity, dehydration).
Among the identified ADRs, 45% were deemed avoidable, with two cases assessed as totally avoidable corresponding to a medication error with a fentanyl patch (failure to remove the previous patch before applying a new patch) and an inappropriate dose of levetiracetam. Gurwitz et al. reported a similar rate of 51% of avoidable ADRs (including both partially and totally avoidable cases) primarily involving psychoactive drugs and anticoagulants [41]. Field et al. found a rate of 55% for avoidable ADRs, which involved anti-infective drugs, antidepressants, antipsychotics, antiepileptic drugs, and opioids [42].
Concerning the risk factors for NHRs admission for ADRs, several studies have identified the number of drugs, polypharmacy, and/or the use of potentially inappropriate medication as risk factors for ED admission of NHRs [18, 43, 44]. However, the method of this study did not allow the identification of potentially inappropriate medication, owing to missing complete medical records in some cases. Moreover, we did not analyze the atropinic burden in this study because it is now well recognized as a factor that increased the risk of falls, cognitive impairment, frailty status, and mortality in older patients [45]. We found that each additional drug was associated with a 1.09-fold increase in the risk of ED admission of NHRs for ADRs (95% CI 1.05–1.13). Moreover, compared with NHRs exposed to fewer than five drugs, those exposed to five to nine drugs had a 1.8-fold increased risk of ED admission for ADRs, while this risk rose to 2.6-fold for those exposed to ten or more drugs. Few studies have suggested the Charlson Comorbidity Index score as another risk factor for ED admission for ADRs [30, 42]. However, this criterion was not significant in this study. However, we did find that a previous ED admission within the year preceding P1 was strongly associated with ED admission for ADRs. More generally, repeated hospital admissions in older patients have been identified as a risk factor of readmission by a large number of studies: Picker et al. reported that more than one ED visit in the previous 6 months could be an independent predictor of 30-day readmission, regardless of age [46]. In patients aged 75 years and older, Deschodt et al. found a previous ED admission within the last 3 months as an independent predictor of ED readmission within 3 months post-discharge [47]. In France, data from the PAERPA study in patients aged 75 years or over, the relative risk of hospital readmission progressively increased from 1.8 (95% CI 1.7–1.9) after one previous hospital stay to 3.0 (95% CI 2.6–3.5) after five previous hospital stays [48]. Lanièce et al. investigated the risk of early unplanned readmission in inpatients aged 75 years and over and suggested a significant association with prior hospitalization within the prior 3 months [49]. In fact, according to the literature, hospital admission is linked to the frailty process in older adults [50, 51]. Moreover, according to our results, the median length of stay in TUH for NHRs admitted for ADRs was 1 day and more than half of these patients stayed 1 day or less, highlighting the questionable relevance of ED admissions and the lack of capacity for NHs to care for NHRs. Thus, NHRs are frail and repeated unplanned admissions could increase the risk of readmission because of ADRs or other reasons. Our findings could be because of a statistical bias related to an imbalance in sample size between different BMI categories.
This study was not designed to specifically assess ED admissions for underuse, but during the review of medical records, we were able to clearly identify 21 cases of ED admissions because of drug underuse, involving the use of anticoagulants, hypoglycemiant drugs, and anticonvulsants. According to Lombardi et al., drug underuse in older people remains associated with frailty, dementia, a risk of adverse events, or the absence of specific clinical trials particularly concerning cardiovascular, anticoagulant, and anti-osteoporotic drugs [17]. As far as we know, only a few studies have analyzed the hospital admissions for drug underuse in NHRs. Park et al. suggested similar results in older patients, with 4.6% of ED admissions because of drug underuse [52].
This study has several limitations. First, it is a retrospective analysis of electronic medical records from a single institution (TUH), a tertiary hospital that serves emergency admissions for a population of over one million inhabitants. However, some patients may have been admitted to other public or private hospitals outside of TUH. During P1, 115,369 patients were admitted to the ED of TUH of whom 26,188 were aged over 65 years (medico-administrative data from TUH not shown). As a result, the prevalence of ED admissions for NHRs may be underestimated. Additionally, cases with ICD-10 codes that were unrelated to ADRs were excluded, although some rare codes, such as inhalation pneumonitis, could potentially correspond to ADRs. Furthermore, the analysis of medical records depended on the availability and completeness of data, particularly regarding drugs. For long-term treatment, the initiation date of medications was often missing from medical records, while this information was more readily available for recently introduced medications.
This study also presents some strengths. We performed a proactive study based on a large dataset of NHRs admitted to the ED without restricting ICD-10 codes corresponding to ADRs, and we analyzed data including all clinical and/or biological information allowing a relevant analysis of ADRs and suspected drug(s). Thus, the method was sensitive and we were able to address the biases related to ICD-10 code misclassification and exclude all false-positives or false-negatives. Another study performed in TUH between 2002 and 2003 in people aged older than 65 years (not only NHRs) admitted to the ED, which analyzed clinical/biological data for each patient, suggested an incidence of ED admission for ADRs of 8.37 per 100 admissions (95% CI 6.52–10.52) [53]. Indeed, ED administrative data have not been fully assessed for their completeness in adverse drug event reporting: Hohl et al. found that only 6.8% of patients admitted to the ED could be identified in administrative records with ICD-10 codes clearly indicating an adverse drug event [54]. Moreover, our data allowed us to follow patients over 2 years and identify cases of readmission for ADRs.

Comments (0)