4.1 Principal Findings
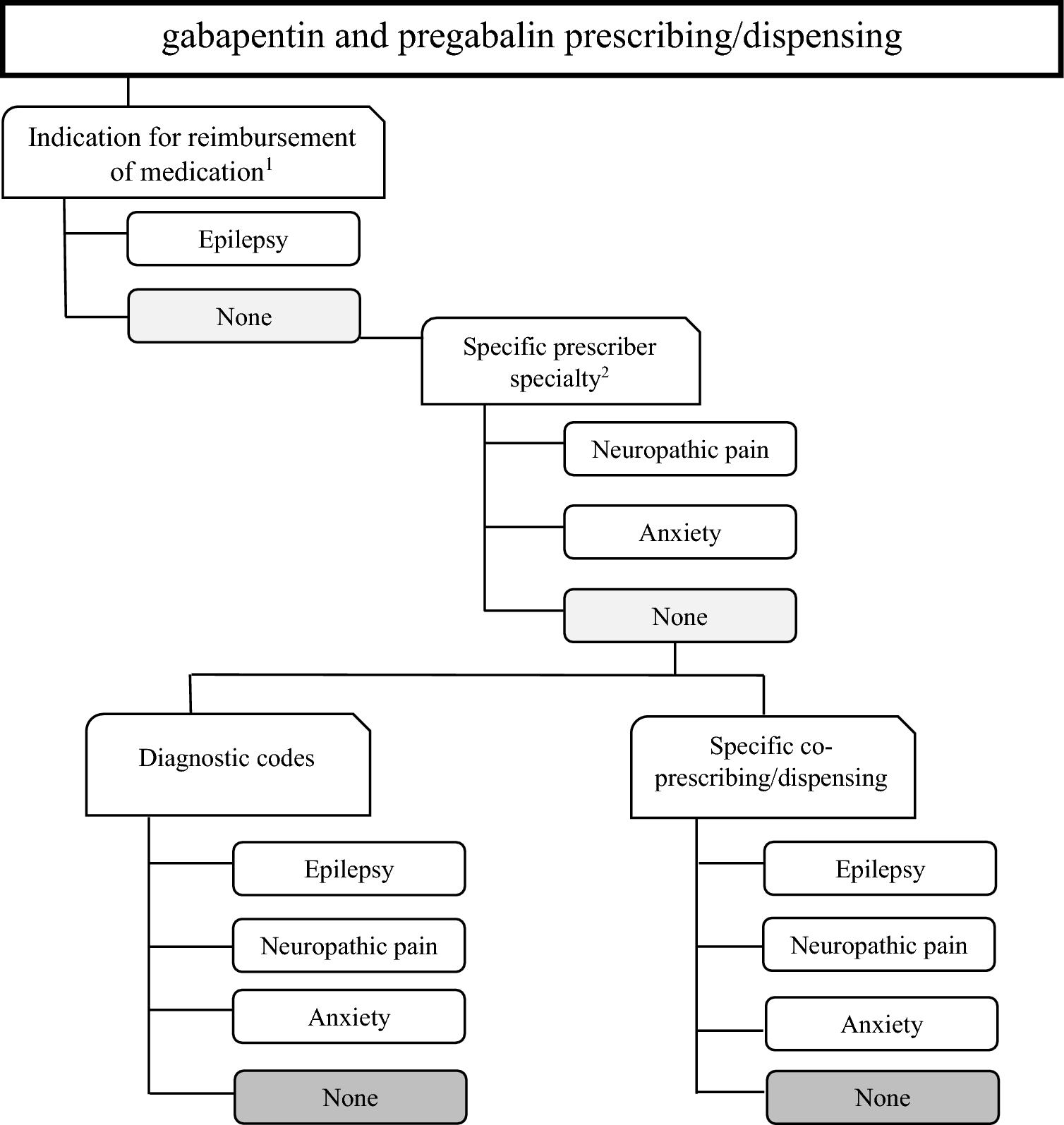
Our study aimed to identify maternal conditions leading to gabapentinoid prescribing among pregnant women using EHR data across Europe. Although our study focuses on pregnant women, condition identification relied, also, on data from periods outside of pregnancy. Nevertheless, differences in healthcare utilization patterns between pregnant women and the general female population may still limit generalizability [5, 13]. Using markers within various data components, including prescriber specialty, primary and specialized health care diagnoses, and prescribed/dispensed co-medications, we identified maternal conditions for 43–90% of pregnancies. Detection improved when the assessment window was extended. Epilepsy was the least frequently captured maternal conditions across all data sources, falling below 15%. Conversely, anxiety was the most common maternal condition captured in Wales, Spain, Finland, and Italy, whereas neuropathic pain predominated in Norway and France. Further analyses suggested unlicensed use in 0–13% of pregnancies depending on the data sources. Analyses also suggested potential for abuse of gabapentinoids in 3–23% depending on the data sources. These findings emphasize the importance of comprehensive data to better understand prescribing practices and potential areas of concern.
4.2 Differences in Prevalence of Gabapentinoid Prescription/Dispensation Between European Countries
Almost three million pregnancies were identified in six data sources, including 11,428 pregnancies where gabapentinoids were prescribed/dispensed (3.9 [95% CI 3.9–4.0] per 1000). This prevalence varied by country, ranging from 1.9 per 1000 in France to 6.6 and 7.7 per 1000 in Wales and Spain, respectively. Our results align with previous studies in Europe [12,13,14,15,16] showing higher prevalence in the UK compared with other European countries in the most recent years [13]. The lower prevalence in Finland and France was expected as medication data were only available from a shorter period before pregnancy, compared with 1 year in the other countries. We also observed differences between specific medications; pregabalin was dispensed/prescribed more often than gabapentin in Finland, France, Italy, and Spain, whereas the opposite was observed in Norway and Wales. Similar patterns were reported in previous studies for the UK, France, and Italy [7, 13, 15, 26].
4.3 Differences in Maternal Conditions Leading to Gabapentinoid Prescribing Between European Countries
The literature on potential indications for use of gabapentinoids among pregnant women is limited and methods greatly varied, making comparisons challenging. Gabapentinoids are rarely used for epilepsy [11], which our study confirms. Previous findings have reported gabapentinoid use for epilepsy in around 6–7% of pregnancies in US data [17, 19] and from 1.5 to 6.6% in European data [7, 14, 15, 18, 27, 28]. Although epilepsy was the least frequently identified condition, exact figures varied from 6.3% and 7.1% of pregnancies in France and Wales to 14.0% and 15.0% in Italy and Finland, respectively.
Data on neuropathic pain and anxiety are scarce. A Nordic study reported neuropathic pain in 16% and 7.5% of pregnancies where pregabalin was dispensed in Finland and Norway, respectively, and anxiety in 22% and 8.5% [14]. Our study found higher proportions for both conditions, likely due to the use of multiple data components, which improved the capture of conditions compared with methods relying only on hospital discharge codes.
By including potential diagnoses for unlicensed indications (including fibromyalgia, restless legs syndrome, bipolar disorder, or insomnia), we identified additional cases classified as ‘other use’. This varied by country, from 2 to 3% in Spain and Italy to 12% in Finland and Wales. A previous study reported records of migraine in 8.1% and 9.8% of pregnancies where pregabalin was prescribed/dispensed in Norway and Finland, respectively, and records of bipolar disorder in 2.8% of Finnish pregnancies [14]. Another study on UK primary care data (1993–2017) found that when diagnostic codes up to 1 year before the prescription were used, indications were identified for only 60% of the individuals, half of which were considered unlicensed [8]. The high prevalence of ‘other use’ in Finland and Wales can be attributed to the inclusion of primary care data, where a wider range of conditions are treated. In Finland, gabapentinoids are recommended for fibromyalgia and restless legs syndrome, both common during pregnancy. While not formally indicated for insomnia, they are acknowledged to improve sleep disorders. These conditions (insomnia, fibromyalgia, and restless legs) likely explain the higher prevalence in these countries.
Our additional analyses revealed a concerning proportion of pregnancies with records of substance use disorders and/or alcohol withdrawal (within 1 year before and after the prescription/dispensation date of gabapentinoid), ranging from 3 to 5% in Italy and France to 17–23% in Finland and Wales. These results add to the growing concerns about gabapentinoid abuse worldwide [29,30,31,32].
4.4 Analysis of the Methodological Approach
In our main analyses, a notable proportion of pregnancies had no identified maternal conditions leading to gabapentinoid prescribing. This proportion varied greatly across data sources, from 11.6% in Norway to 56.4% in Italy. This can be attributed to several factors: (i) differences in available data components; some data sources, like France and Spain, provided data for only two or three components; (ii) differences in data coverage; France, for instance, only covered from 2.5 months before pregnancy to its end, whereas Norway, Italy, Spain, and Wales had full study period coverage; (iii) variations in how maternal conditions were defined across data sources. These factors likely impacted the algorithm’s capacity to detect relevant maternal conditions that motivate prescribing, particularly in Italy, raising concerns about its accuracy when capture rates were low.
In addition, recorded anxiety was observed in many women prescribed gabapentin ranging from 18.6% in France to over 60% in the Spain and Wales. However, gabapentin is not licensed for anxiety in Europe, suggesting possible unlicensed prescribing.
A previous study that was used as a foundation of our methodology [5] reported a higher percentage of neuropathic pain indications for gabapentin and pregabalin. That study classified neuropathic pain by exclusion, if no epilepsy, bipolar, anxiety, or migraine markers were found; this meant no women were left without an identified indication, but at the risk of misclassification. In contrast, our approach did not make such assumptions, leading to a non-negligible proportion of pregnancies with no detected condition.
Similar findings were reported elsewhere. A Swedish study (2005–2009) found no record of approved indication for pregabalin in 60% of individuals [33], using only hospital and primary care data within 1 year of pregabalin prescription. A UK study (1993–2017) found no identified indication for 40% of the individuals, using primary care data up to 1 year before the gabapentinoid prescription [8]. These high percentages observed in both studies might reflect limited data availability, and/or follow-up. However, in Wales, where we integrated hospital discharge diagnoses and co-medications, maternal conditions were identified in 78% of pregnancies using a similar assessment window, suggesting that additional data components improve the capture of maternal conditions. Nevertheless, differences in the study populations may also explain variations. The UK study [8] included a more affluent population than our data from Wales, and pregnant women generally have more frequent contacts with primary care services than the general population due to prenatal monitoring. As in the Swedish study [33], these differences likely contribute to variations in identifying maternal conditions leading to gabapentinoid prescribing.
By integrating multiple data components such as prescriber specialty specialized health care diagnoses, and prescribed/dispensed co-medications, our algorithm improves upon previous methods relying solely on inpatient diagnoses [33]. Our findings suggest that co-medication data may contribute to the identification of maternal conditions leading to gabapentinoid prescribing. However, its use as a proxy remains subject to limitations, particularly regarding the specificity of the identified conditions. The inclusion of primary care data, when available, is particularly valuable for detecting maternal conditions typically managed in this setting. Whereas hospital data are commonly used to identify diseases and infer maternal conditions leading to prescribing, our results show that this component contributes less than co-medications and primary care data. Notably, outpatient data had a greater impact than inpatient data, possibly reflecting the nature of the conditions studied. Indeed, epilepsy, anxiety, and neuropathic pain are chronic conditions primarily managed in primary or specialized care, with few requiring overnight hospitalization. Healthcare system differences in primary care versus outpatient care use may also influence these patterns. Therefore, the contributions of each data component dependents on both the conditions studied and the healthcare settings from which the data originate.
Extending the assessment window improved the recoding of maternal conditions leading to gabapentinoid prescribing in most of the data sources, with variations by condition. Epilepsy detection remained stable, whereas anxiety detection increased. As a chronic condition, epilepsy is unlikely to be affected by the length of the assessment window, and extending it beyond 1 year did not identify additional cases. However, a longer assessment period may increase the detection of co-morbidities, such as anxiety, and misattribute resolved conditions as potential reasons for prescribing.
4.5 Strengths and Limitations
The main strength of the study is its comprehensive and multi-faceted approach to assessing maternal conditions that motivate gabapentinoid prescribing among pregnant women. By integrating multiple data components, such as prescriber specialty, primary and specialized healthcare diagnoses, prescribed/dispensed co-medications, and prospectively recorded data, our study enhanced our understanding of the reasons for gabapentinoids use during pregnancy. Notably, our study includes three million pregnancies identified in six European countries with 11,428 pregnancies with gabapentinoid prescription/dispensations. It covers entire national populations (Finland, Norway, and Wales) as well as regions (Valencian region—Spain, Emilia Romagna—Italy and Haute-Garonne—France). Additionally, the inclusion of data from various countries strengthens the generalizability of the findings throughout, at least, high-income countries.
The main limitation of the study is the absence of detailed clinical data to validate our approach using detailed medical records at the individual level. Whereas data quality is generally high in the Medical Birth Register, prescription databases and hospital discharge records are considered good. However, data quality of primary health care databases may be more challenging as validity of codes have been less studied [34, 35]. Moreover, dispensed medications for inpatient use were not recorded in any of the participating data sources. In addition, identification of early terminations and miscarriage are either impossible or incomplete, leading to an under-estimating of the prevalence of gabapentinoid prescribing/dispensing among pregnant women, especially if medication use is associated with early terminations [18]. Another limitation is that we were unable to distinguish between co-incidental co-morbidities and the true maternal condition driving the prescription, especially for common conditions and unlicensed indications, such as anxiety. Furthermore, coding practices varied both between and within data sources, introducing inconsistencies in the identification and classification of maternal conditions. Differences in data availability across data sources further limit direct comparisons. Furthermore, the ability of the algorithm to detect maternal conditions depended on the data components available, as seen in Italy and France. Consequently, controlling for indication bias using our approach may be more effective in some data sources than others. Lastly, comparing our findings with other studies is challenging due to multiple factors: (i) differences in data availability; (ii) variation in disease coding; (iii) differences in study periods; (iv) differences in healthcare settings and population demographics; and (v) differences in gabapentinoid prescription patterns over the study period. Consequently, these factors must be considered when interpreting and extrapolating our results.
4.6 Implications
Our results provide a picture of the reasons why gabapentinoids are being prescribed to pregnant women. Understanding the prevalence of different maternal conditions, such as neuropathic pain and anxiety, can help regulatory agencies and health authorities to guide recommendations and decision making. Healthcare providers should carefully consider the potential risks and benefits of prescribing these medications during pregnancy, while also considering alternative treatment options. We found that a non-negligible proportion of women prescribed/dispensed gabapentinoids were at risk of substance or alcohol abuse and dependence, highlighting the need for careful consideration when prescribing gabapentinoids to avoid iatrogenic effects.
Our approach allows for detailed drug utilization analyses according to maternal conditions that could help to explain drivers behind the growing use of gabapentinoids during pregnancy, and further to examine their safety in different maternal contexts. In addition, in cases where diagnostic codes are less specific, integrating multiple data components becomes crucial to improving the detection of these conditions. Notably, incorporating primary care data significantly improved the detection process. This study explores the potential of EHR data as proxies for identifying maternal conditions leading to gabapentinoid prescribing. While our findings suggest that this approach may provide valuable insights, it remains exploratory and subject to limitations, particularly regarding its ability to correctly distinguish true maternal conditions leading to gabapentinoids prescription from unrelated co-medication use.
Lastly, further validation of our approach using detailed individual-level medical records would help strengthen confidence in its accuracy. One potential approach for validation could involve analyzing demographic characteristics and healthcare trajectories within a sample of pregnancies. Maternal conditions may cluster with specific demographic profiles or typical sequences of medical care (e.g., specialist consultations, hospital admissions, prescription patterns). Comparing these elements with clinical expert assessments would allow evaluation of the concordance between algorithm-based classifications and expert judgment.

Comments (0)