
Remember me


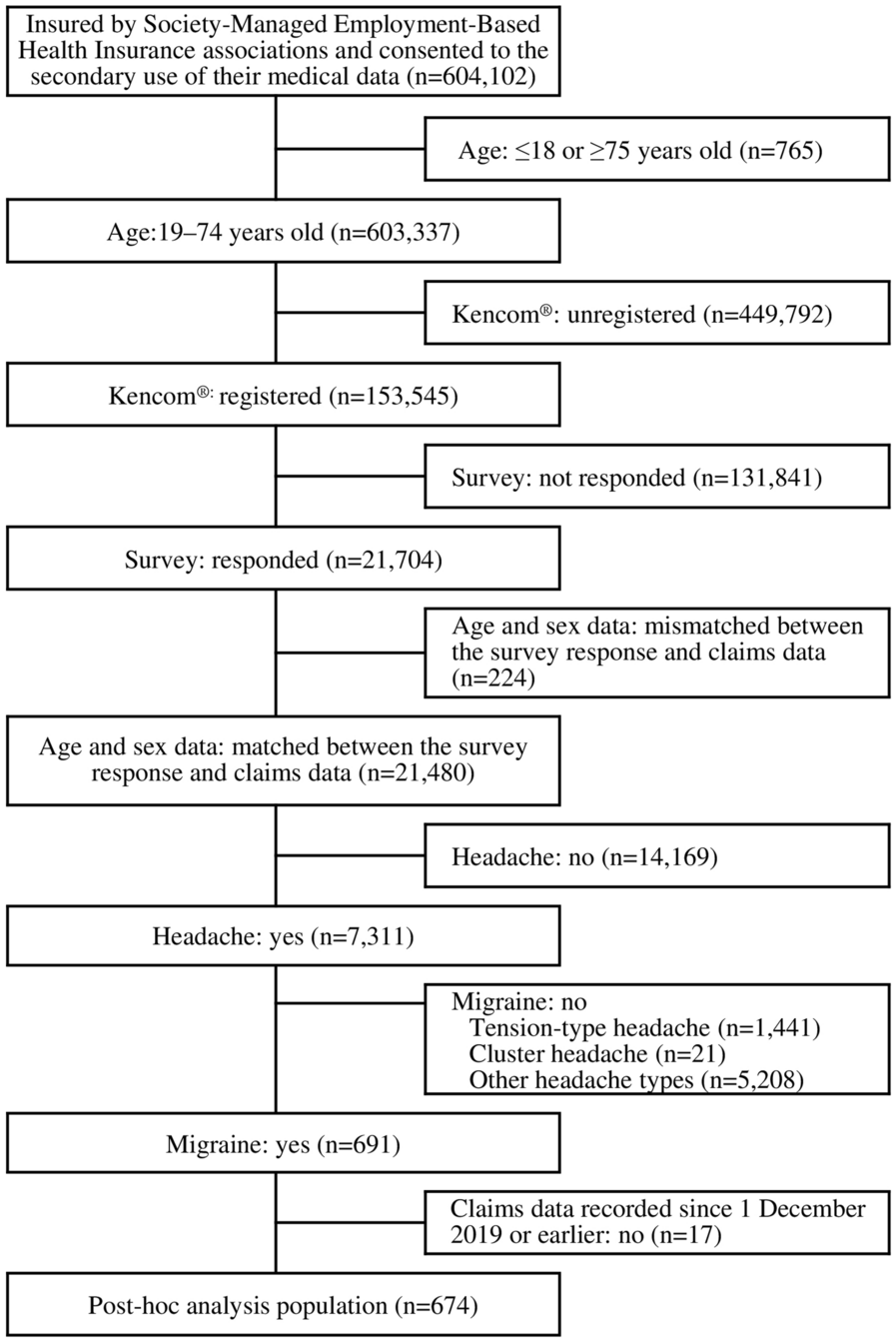

Overall, 2973 patients met the study criteria (Fig. 1). The key sub-studies included 2549 patients with CKD, 879 patients with HF and 395 patients receiving treatment with MRA, respectively. The supplemental sub-studies included 1893 patients with hyperkalemia, 2668 patients with CKD or HF, 119 patients with HF and no CKD, and 903 patients with resistant hypertension, respectively (Supplementary Table S2).
Fig. 1
Sample selection. CKD chronic kidney disease, ESKD end-stage kidney disease, HF heart failure, MRA mineralocorticoid receptor antagonist, RAASi renin-angiotensin-aldosterone system inhibitor, SZC sodium zirconium cyclosilicate
Baseline CharacteristicsIn the overall sample (Table 1), the mean (SD) patient age was 66.3 (14.2) years, and 41.6% of patients were female. The most common type of pharmacy insurance was Medicare Advantage (50.1%), followed by Medicaid (21.8%) and commercial insurance (19.4%). The mean (SD) Charlson Comorbidity Index (CCI) was 3.0 (1.9), with common comorbidities being hypertension (89.8%), stage 1–4 CKD (85.7%) and diabetes (75.5%).
Table 1 Baseline characteristics of overall sample and CKD, HF and MRA sub-studiesWhile all patients in the overall sample had RAASi use at index, as per study design, most patients (85.1%) also had ≥ 1 prescription fill for a RAASi during the baseline period. At index, the most commonly used RAASi were angiotensin-converting enzyme inhibitors (ACEis; 47.4%) and angiotensin-receptor blockers (ARBs; 45.4%). Over half of patients (59.7%) had an optimized RAASi dose at index, and just under one-fourth of patients (23.7%) had a maximized RAASi dose at index. Other commonly used medications during baseline included diuretics (59.8%), beta blockers (58.0%) and calcium channel blockers (49.4%).
Patient characteristics were generally similar to the overall sample in the CKD sub-study, with some differences in the HF and MRA sub-studies (Table 1). Patients in the HF sub-study were slightly older than the overall sample, with a mean (SD) age of 68.5 (12.8) years, and were generally sicker, with a mean (SD) CCI score of 4.8 (1.7). The prevalence of several comorbidities tended to be higher in the HF sub-study than in the overall sample; these included coronary artery disease (59.0%), resistant hypertension (51.0%), peripheral vascular disease (49.8%) and acute kidney injury (45.6%). At index, patients with HF were more likely to receive MRAs (19.2%) than the overall sample. The use of some medications during baseline also tended to be higher in patients with HF than in the overall sample, including diuretics (80.7%), beta blockers (79.9%) and vasodilators (23.8%).
In the MRA sub-study, patients with MRA use were slightly less likely to be female (37.2%) and were sicker than the overall sample on average, with a mean (SD) CCI score of 3.7 (2.3). Patients with MRA use tended to have a higher prevalence of acute kidney disease (38.0%), coronary artery disease (44.6%), HF (52.9%) and resistant hypertension (64.3%) during baseline than the overall sample. Patients with MRA use were also more likely to use certain medications, including diuretics (93.2%) and beta blockers (74.7%), than all patients included in the study.
Patient characteristics were generally similar in the supplemental sub-studies (Supplementary Table S2).
RAASi Dosing During Follow-UpDuring the 6-month follow-up period, the overall sample had a mean (SD) SZC use duration of 107.0 (72.7) days. Among 2973 patients in the overall sample, 1894 (63.7%) had an optimized (≥ 50% of target) RAASi dose and 809 (27.2%) had a maximized (≥ 100% of target) RAASi dose during follow-up (Fig. 2).
Fig. 2
Proportion of patients with an optimized or maximized RAASi dose during the follow-up period in the overall sample and among the CKD, HF and MRA sub-studies. CKD chronic kidney disease, HF heart failure, MRA mineralocorticoid receptor antagonist, RAASi renin-angiotensin-aldosterone system inhibitor
In the CKD and HF sub-studies (mean [SD] follow-up: 109.9 [71.8] and 104.3 [77.0] days, respectively), similar results were observed—63.5% of patients in the CKD sub-study and 63.9% of patients in the HF sub-study had an optimized RAASi dose during follow-up, and 27.0% of patients in the CKD sub-study and 27.5% of patients in the HF sub-study had a maximized RAASi dose during follow-up. In the MRA sub-study (mean [SD] follow-up: 112.2 [81.7] days), a slightly higher proportion of patients had an optimized RAASi dose (86.3%) and a maximized RAASi dose (32.7%) during follow-up than the overall sample were observed (Fig. 2). In the supplemental sub-studies, the proportions with an optimized or maximized RAASi dose during follow-up were similar to those in the overall sample (Supplementary Figure S1).
Characteristics Associated with RAASi Dosing During Follow-UpResults of the multivariable logistic regression model examining potential predictors of having an optimized RAASi dose in the overall sample are summarized in Fig. 3. Predictors statistically significantly associated with higher odds of having an optimized RAASi dose included arrythmia (OR: 2.72 [95% CI 1.45, 5.49]), use of any diuretic (1.66 [95% CI 1.37, 2.02]), use of any central alpha-2 receptor agonists (1.46 [95% CI 1.04, 2.10]) and use of any RAASi during baseline (1.85 [95% CI 1.47, 2.31]) (all p < 0.05). Predictors statistically significantly associated with lower odds of having an optimized RAASi dose included being in the Northeast (OR: 0.66 [95% CI 0.53, 0.82]), Midwest (0.55 [95% CI 0.42, 0.71]) or West (0.77 [95% CI 0.61, 0.96]) compared to the South, having Medicare Advantage (0.58 [95% CI 0.45, 0.75]) or Medicaid (0.59 [95% CI 0.45, 0.78]) pharmacy insurance coverage compared to commercial and having any all-cause outpatient visits (0.48 [95% CI: 0.36, 0.63]) (all p < 0.05).
Fig. 3
Characteristics associated with an optimized RAASi dose during follow-up. CI confidence interval, CKD chronic kidney disease, COVID-19 coronavirus disease 2019, ED emergency department, ESKD end-stage kidney disease, HK hyperkalemia, IP inpatient, K potassium, NSAIDs non-steroidal anti-inflammatory drugs, OP outpatient, OR odds ratio, RAASi renin-angiotensin-aldosterone system inhibitor, Ref reference, SGLT2i sodium-glucose cotransporter-2 inhibitors, SZC sodium zirconium cyclosilicate
Similar results were found in the model examining potential predictors of maximized RAASi dose (Fig. 4). Specifically, predictors statistically significantly associated with higher odds of having a maximized RAASi dose included resistant hypertension (OR: 1.32 [95% CI 1.04, 1.68]), liver disease (1.48 [95% CI 1.11, 1.95]), use of any diuretic (1.47 [95% CI 1.18, 1.83]), use of any central alpha-2 receptor agonists (1.67 [95% CI 1.21, 2.29]), use of any calcium channel blockers (1.35 [95% CI 1.13, 1.62]), use of any RAASi during baseline (1.61 [95% CI 1.23, 2.12]) and use of any sodium-glucose cotransporter-2 inhibitors (SGLT2i; 1.32 [95% CI 1.03, 1.69]) (all p < 0.05). Predictors statistically significantly associated with lower odds of having a maximized RAASi dose included being in the Northeast (OR: 0.67 [95% CI 0.53, 0.84]), Midwest (0.75 [95% CI 0.57, 0.99]) or West (0.76 [95% CI 0.60, 0.97]) compared to the South and having Medicare Advantage (0.72 [95% CI 0.55, 0.93]) or Medicaid (0.67 [95% CI 0.51, 0.89]) pharmacy insurance coverage relative to commercial (all p < 0.05).
Fig. 4
Characteristics associated with a maximized RAASi dose during follow-up. CI confidence interval, CKD chronic kidney disease, COVID-19 coronavirus disease 2019, ED emergency department, ESKD end-stage kidney disease, HK hyperkalemia, IP inpatient, K potassium, NSAIDs non-steroidal anti-inflammatory drugs, OP outpatient, OR odds ratio, RAASi renin-angiotensin-aldosterone system inhibitor, Ref reference, SGLT2i sodium-glucose cotransporter-2 inhibitors, SZC sodium zirconium cyclosilicate
Comments (0)