
Remember me



This retrospective study utilized Medicare 100% Limited Data Set (LDS) administrative claims from January 1, 2017, to March 31, 2021. The LDS standard analytical files include beneficiary-level information such as demographics, diagnosis, procedure, claim dates, cost, and payment information. The LDS contains data for both institutional and non-institutional providers (i.e., inpatient hospital, outpatient hospital, skilled nursing facility, home health, and hospice).
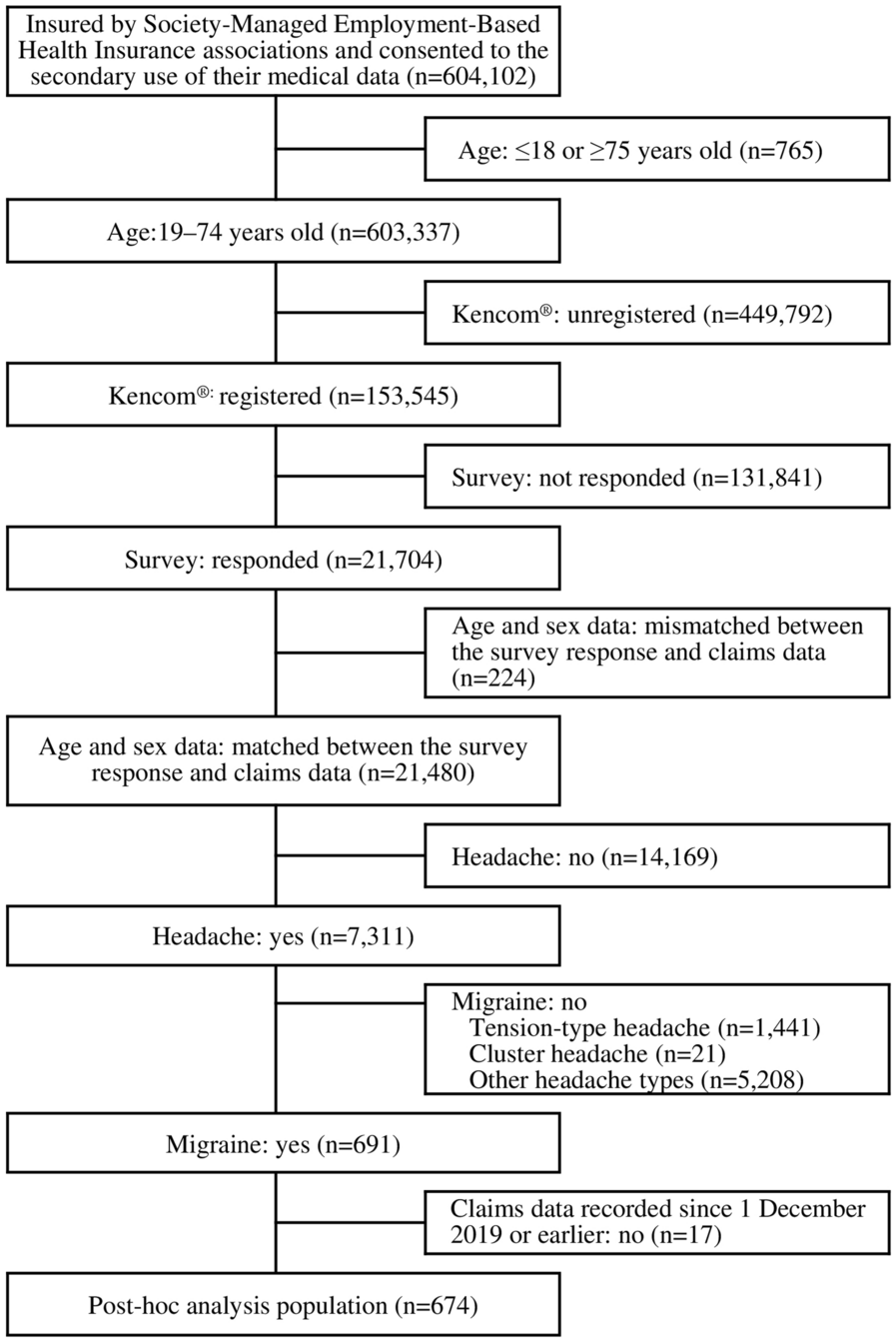
Patient Selection and Study DesignThe patient identification period was July 1, 2017, to March 31, 2021. Medicare beneficiaries aged 18 years or older were categorized into 2 groups: patients with postsurgical chronic HypoPT (n = 1,166) and those without HypoPT (n = 11,258). For individuals with chronic postsurgical HypoPT, the first claim for HypoPT (ICD-10 codes E200, E208, E209, or E892) after a related surgical procedure acted as the index diagnosis (i.e., index date). A patient needed at least 1 claim of a HypoPT-related surgical procedure in the 6-month baseline period prior to index diagnosis, and an additional confirmatory second HypoPT diagnosis in the ≥ 6–12 months from index diagnosis to be considered a patient with postsurgical chronic HypoPT.
The control group included those without a HypoPT diagnosis in the patient identification period but with at least 1 medical claim of any type during the study period. For enrollees without HypoPT, a synthetic index date was assigned based on the distribution of time between the first medical claim of any kind and the index date as observed among individuals with postsurgical chronic HypoPT. Both patient groups had to have had continuous enrollment in Medicare for at least 6 months before and 12 months after the index date. Patients were followed from the index date until the time of death, end of data coverage, or Medicare enrollment, whichever occurred first. Figure 1 illustrates the study design.
Fig. 1
Study design. *Patients were followed from the index date until the time of death, end of data coverage, or end of Medicare enrollment, whichever occurred first. HypoPT hypoparathyroidism
Ethical ApprovalDue to the de-identified nature of the retrospective dataset, the study did not require ethics committee review. Permission for reuse of the Medicare 100% Limited Data Set was granted by its owner.
Patient and Baseline CharacteristicsBaseline sociodemographic characteristics (age, gender, race, ethnicity, census region), clinical characteristics (Charlson Comorbidity Index [CCI] score, cardiovascular complications, infections, renal complications, mental ill-health, fracture, cataract, hypocalcemia, neurological complications), and HCRU and costs (number of hospitalizations, number of outpatient visits, total medical costs) were considered for inclusion in this analysis.
Healthcare Resource Utilization and CostsTo quantify the economic burden, three definitions of HCRU and costs were determined for each patient: all-cause, HypoPT-only, and HypoPT plus related long-term complications. The all-cause burden definition included HCRU and costs from any type of claim. The HypoPT-only definition comprised HCRU and costs from claims with a HypoPT diagnosis code only, which, by definition, would result in 0 values for that particular burden definition for control patients without HypoPT. The HypoPT plus related long-term complication definition included HCRU and costs from claims with either a HypoPT diagnosis code and/or a relevant HypoPT-related long-term complication diagnosis code. The use of the third burden definition allows for a more thorough assessment of HCRU and costs associated with both HypoPT and its related complications. A list of these complications is provided in Table S1 in the Supplementary Material.
HCRU was measured in terms of the number of hospitalizations, ED visits, home health visits, hospice visits, skilled nursing facility visits, and outpatient visits. Costs were assessed both as total medical costs and individually for each category mentioned.
Study OutcomesStudy outcomes included the number and proportion of patients receiving each type of HCRU among the two study cohorts. Also calculated was the average use per patient per year (PPPY) for each resource type and its cost, comparing the two groups. Costs were adjusted for inflation to 2021 US dollars based on the medical care component of the Consumer Price Index.
Statistical AnalysisAnalyses for all study objectives were conducted among both unmatched and matched cohorts and then compared with their respective control groups. Via a matching algorithm, a 1:2 matching ratio was employed where individuals with postsurgical chronic HypoPT were matched to potential controls based on age, gender, race, region, CCI score, and index year. The algorithm allowed for a variable ratio between the number of matched cases and control patients, as guided by Faries et al. (2020) and Stuart et al. (2010) [25, 26]. The decision to use a 1:2 matching ratio aimed to optimize sample size retention while ensuring a balance in baseline characteristics.
Within both the unmatched and matched samples, descriptive statistics were reported for baseline characteristics, HCRU, and costs, stratified by patients with postsurgical chronic HypoPT versus those without HypoPT. Baseline sociodemographic and clinical characteristics are described; frequencies and percentages are reported for categorical variables, and mean, median, and range are reported for continuous ones.
Adjusted multivariable regression analysis was performed to compare all-cause total medical costs and specific HCRU (i.e., all-cause hospitalizations and outpatient visits) between the unmatched study groups. Generalized linear models with a gamma distribution and log-link function were used for modeling costs, while Poisson distribution with a log-link function was used for modeling resource utilization. The main model (i.e., Model 1) was fully adjusted for age, gender, race, region, and comorbidities and complications at baseline. Additional models aimed to investigate the specific factors influencing all-cause total medical costs and specific HCRU. Model 2 did not adjust for baseline nephrocalcinosis, nephrolithiasis, or stage 3–5 CKD to explore the effect of renal complications on the burden coefficient for postsurgical chronic HypoPT. Model 3 explored the determinants of all-cause total medical costs and specific HCRU, irrespective of whether or not patients were flagged as having postsurgical chronic HypoPT. A cost ratio > 1.0 with a P value below 0.05 indicated a significant influence on all-cause total medical costs. All analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC, USA).
Comments (0)